


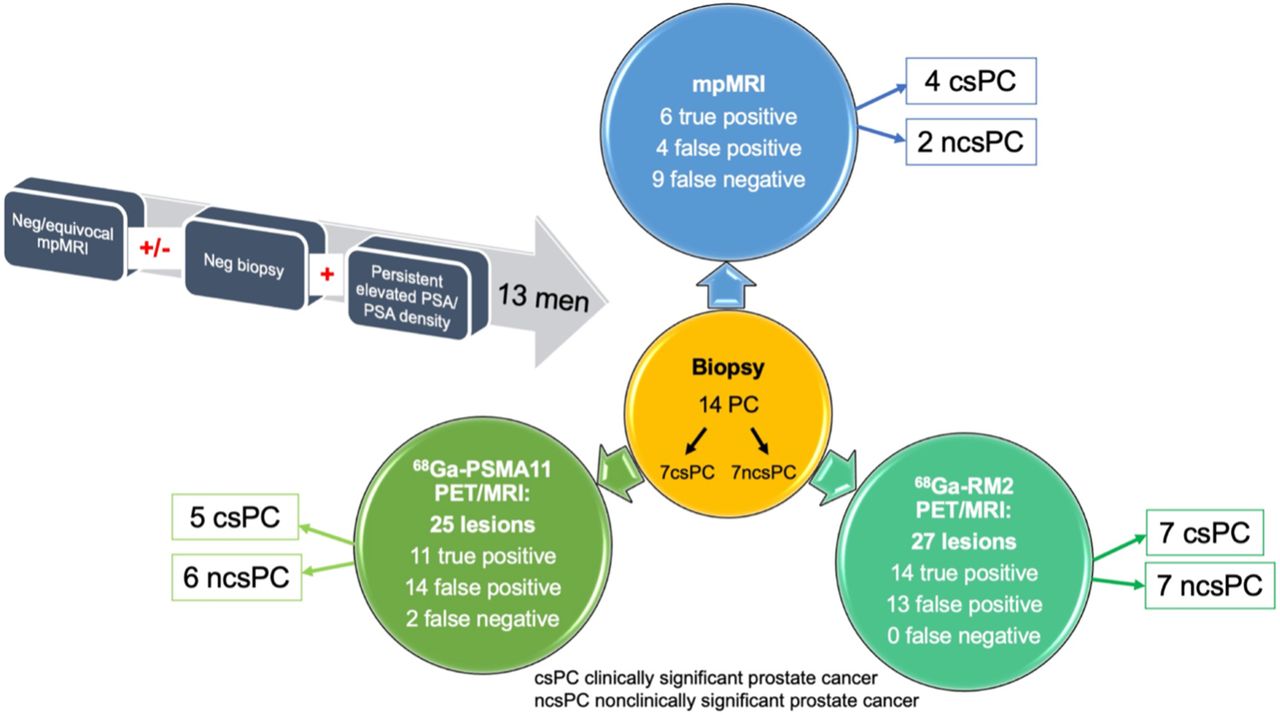
Visual Abstract

Abstract
Targeting of lesions seen on multiparametric MRI (mpMRI) improves prostate cancer (PC) detection at biopsy. However, 20%–65% of highly suspicious lesions on mpMRI (PI-RADS [Prostate Imaging-Reporting and Data System] 4 or 5) are false-positives (FPs), while 5%–10% of clinically significant PC (csPC) are missed. Prostate-specific membrane antigen (PSMA) and gastrin-releasing peptide receptors (GRPRs) are both overexpressed in PC. We therefore aimed to evaluate the potential of 68Ga-PSMA11 and 68Ga-RM2 PET/MRI for biopsy guidance in patients with suspected PC. Methods: A highly selective cohort of 13 men, aged 58.0 ± 7.1 y, with suspected PC (persistently high prostate-specific antigen [PSA] and PSA density) but negative or equivocal mpMRI results or negative biopsy were prospectively enrolled to undergo 68Ga-PSMA11 and 68Ga-RM2 PET/MRI. PET/MRI included whole-body and dedicated pelvic imaging after a delay of 20 min. All patients had targeted biopsy of any lesions seen on PET followed by standard 12-core biopsy. The SUVmax of suspected PC lesions was collected and compared with gold standard biopsy. Results: PSA and PSA density at enrollment were 9.8 ± 6.0 (range, 1.5–25.5) ng/mL and 0.20 ± 0.18 (range, 0.06–0.68) ng/mL2, respectively. Standardized systematic biopsy revealed a total of 14 PCs in 8 participants: 7 were csPC and 7 were nonclinically significant PC (ncsPC). 68Ga-PSMA11 identified 25 lesions, of which 11 (44%) were true-positive (TP) (5 csPC). 68Ga-RM2 showed 27 lesions, of which 14 (52%) were TP, identifying all 7 csPC and also 7 ncsPC. There were 17 concordant lesions in 11 patients versus 14 discordant lesions in 7 patients between 68Ga-PSMA11 and 68Ga-RM2 PET. Incongruent lesions had the highest rate of FP (12 FP vs. 2 TP). SUVmax was significantly higher for TP than FP lesions in delayed pelvic imaging for 68Ga-PSMA11 (6.49 ± 4.14 vs. 4.05 ± 1.55, P = 0.023) but not for whole-body images, nor for 68Ga-RM2. Conclusion: Our results show that 68Ga-PSMA11 and 68Ga-RM2 PET/MRI are feasible for biopsy guidance in suspected PC. Both radiopharmaceuticals detected additional clinically significant cancers not seen on mpMRI in this selective cohort. 68Ga-RM2 PET/MRI identified all csPC confirmed at biopsy.
The most common pathway to diagnose prostate cancer (PC) is through prostate needle biopsy driven by high serum prostate-specific antigen (PSA). PSA is a highly sensitive but not very specific marker for PC. Therefore, relying solely on elevated PSA for prostate biopsy leads to unnecessary biopsies with negative results or overdiagnosing of nonclinically significant PC (ncsPC) (1). Transrectal ultrasound (TRUS) is widely available and used to guide prostate biopsies. It consists of systematic sampling of the entire prostate using 12 passes through the rectum or perineum. This standardized procedure can miss cancers located in the prostate anteriorly (2). Multiple trials showed that multiparametric MRI (mpMRI)–guided prostate biopsy had higher accuracy in detecting clinically significant PC (csPC), that is, Gleason score ≥ 3 + 4, than TRUS (3–5). However, 20%–65% of suspicious lesions on mpMRI (PI-RADS [Prostate Imaging-Reporting and Data System] 4 or 5) are false-positives (FPs), while 5%–10% of csPC may be missed by mpMRI (6–10). Like TRUS, mpMRI also has blind spots in the transition and central zone of the prostate where PC lesions may be overlooked (11).
PET combined with MRI and prostate-specific membrane antigen (PSMA) targeting radiopharmaceuticals improved PC imaging significantly. However, PSMA-targeted compounds have certain limitations related to expression in other normal tissues and pathologies, while up to 10% of PC are PSMA-negative (12,13). 68Ga-RM2 is a PET radiopharmaceutical that targets gastrin-releasing peptide receptors (GRPRs), which are highly overexpressed in PC, while benign prostate tissues show lower expression (14). GRPR expression is particularly high at earlier stages of prostatic carcinogenesis, making it an interesting target for initial staging (15,16). PSMA- and GRPR-targeting radiotracers have been reported as being complementary (17,18). 68Ga-PSMA11 PET/CT–targeted prostate biopsy showed a high accuracy of 80.6% (19) whereas 68Ga-PSMA11 PET/MRI, with its high soft-tissue contrast and various functional sequences, performed better, with an accuracy of 90% (20).
In this prospective pilot study, we aimed to evaluate the potential of combined 68Ga-PSMA11 and 68Ga-RM2 PET/MRI for biopsy guidance in a highly selective patient cohort who had prior negative or equivocal mpMRI (PI-RADS 1–3) results or prior negative prostate biopsy but persistent elevated PSA and PSA density, therefore considered highly suspicious of having PC. We also assessed the potential for detection of csPC.
MATERIALS AND METHODS
Participants
Participants with negative or equivocal mpMRI (PI-RADS 1–3) results or prior negative prostate biopsy with clinical suspicion for PC, defined as persistently elevated and rising PSA and PSA density, were prospectively enrolled and underwent either 68Ga-PSMA11 PET/MRI first followed by 68Ga-RM2 PET/MRI within 2 wk or vice versa. This prospective, open-label, Health Insurance Portability and Accountability Act–compliant study was approved by the local institutional review board and was registered on ClinicalTrials.gov (NCT03809078). All patients provided written informed consent. The intended total number of participants was 20; however, the Food and Drug Administration approval for 68Ga-PSMA11 during the timeline of the protocol made funding and completion of planned enrollment unfeasible.
Scanning Protocols
PET/MRI
Imaging was performed using a 3T time-of-flight–enabled PET/MRI scanner (SIGNA PET/MRI; GE Healthcare), as previously described (17,21). Image acquisition started at 46 ± 3 (range, 40–51) min after injection of 176 ± 39 (range, 81–208) MBq of 68Ga-PSMA11 and at 45 ± 3 (range, 40–49) min after injection of 139 ± 9 (range, 116–155) MBq of 68Ga-RM2. Simultaneous PET/MRI was acquired from vertex to midthigh with an acquisition time of 4 min per bed position. Additional dedicated 20-min pelvic images were acquired after a delay of 26 ± 6 (range, 19–41) min for 68Ga-PSMA11 and 25 ± 6 (range, 13–38) min for 68Ga-RM2. The PET/MRI scans were acquired 7 ± 3 (range, 2–12) d apart. Synthesis of 68Ga-PSMA11 and 68Ga-RM2 was previously described (17).
mpMRI
mpMRI was performed as routine clinical scanning before prostate biopsy using a 3T scanner (MR750; GE Healthcare) with an external 32-channel body array coil. The imaging protocol consisted of T2-weighted imaging, diffusion-weighted imaging, and dynamic contrast-enhanced imaging sequences. Diffusion-weighted imaging was obtained using a combination of b-values (b50/800/1,400/calculated 2,000 s/mm2). Detailed acquisition parameters were previously described (22).
Image Analysis
Two nuclear medicine physicians reviewed and analyzed PET images independently and in random order. Any focal uptake of 68Ga-RM2 or 68Ga-PSMA11 with an SUVmax above adjacent prostate background and not associated with physiologic accumulation was recorded as suspicious for PC. A region of interest was drawn over suspected lesions to measure SUVmax and SUVpeak and served as an identification marker. SUVpeak is defined as the average SUV within a small, fixed-size region of interest (1 cm3) (23). The MR portion was used for anatomic and lesion (if any were seen) correlation. For segment-based sensitivity and specificity calculation, the prostate was divided into the same 12 segments as for systematic prostate biopsy on MR images.
mpMRI was analyzed using the PI-RADS criteria, version 2 (24). Lesions with a PI-RADS score ≥ 3 were recorded. A PI-RADS score of 3 was considered equivocal, PI-RADS of 4 likely, and PI-RADS 5 highly likely for PC.
Prostate Biopsy
Prostate biopsies were performed transrectally under peripheral nerve block anesthesia by a single urologist. 68Ga-RM2 and 68Ga-PSMA PET/MRI and mpMRI were reviewed by the urologist, radiologist, and nuclear medicine physician. Any PET-positive lesions were annotated on the correlating mpMRI. The transrectal ultrasound probe (Noblus; Hitachi Aloka) was attached to the robotic arm of a prostate fusion biopsy system (Eigen/Artemis), which enabled registration and fusion of mpMRI with real-time ultrasound to create a 3-dimensional model of the prostate with delineated annotations. PET-guided biopsy included a maximum of 3 cores per target lesion. Next, systematic 12-core biopsy was obtained consisting of 1 core through the apex, mid, and base regions, both medially and laterally, from left and right prostate lobes (25,26).
Statistical Analysis
Statistical analysis was performed using Stata 16.1 (StataCorp LP) and R version 4.1.1 (r-project.org). Continuous data are presented as median ± SD, minimum (min)–maximum (max) values. Sensitivity and specificity are given in percentage with 95% CI. A Student t test was used to assess significance between SUV of whole-body and delayed pelvic imaging. Comparison between biopsy-positive and biopsy-negative prostate segments for PI-RADS and SUVmax was done by Wilcoxon rank-sum testing adjusted for clustering.
RESULTS
Thirteen men, aged 58.0 ± 7.1 y (range, 41.0–69.0 y), with suspected PC were prospectively enrolled. PSA and PSA density at the time of PET/MRI were 9.8 ± 6.0 (range, 1.5–25.5) ng/mL and 0.20 ± 0.18 (range, 0.06–0.68) ng/mL2, respectively. Prostate biopsy before imaging was available in 12 of 13 patients of whom 9 were negative and 3 showed Gleason 3 + 4 cancer (negative mpMRI). All patients’ characteristics are summarized in Table 1.
Patients’ Characteristics
mpMRI
All participants underwent routine prebiopsy mpMRI: 5 participants had a negative scan result and 10 lesions were seen in 8 participants. There were 3 PI-RADS 3 (equivocal), 6 PI-RADS 4, and 1 PI-RADS 5 lesions. At study enrollment, 4 of the PI-RADS 4 lesions had a negative prostate biopsy result and 2 PI-RADS 4 and the 1 PI-RADS 5 lesion were equivocal on prior mpMRI from outside institutions (Table 1). Biopsy confirmed 3 true-negative (TN) participants and 6 true-positive (TP) lesions, of which all were csPC, and 4 FP lesions. The highest number of false-negatives (FNs) was seen in mpMRI with 9; however, only 2 FNs were csPC. Sensitivity and specificity were 30% (95% CI, 5, 77%) and 95% (95% CI, 85, 98%), respectively.
Prostate Biopsy
Prostate biopsies were performed 19 ± 12 (range, 2–38) d after PET/MRI. A median of 8 ± 3 (range, 2–13) additional PET-guided biopsies were performed in addition to systematic 12-core template. One patient refused to undergo systematic biopsy and had PET-guided biopsy only. Histopathology showed PC in 8 of 13 (61.5%) patients, with a total of 14 PC lesions (multifocal disease in 6 patients), of which 7 (50%) were csPC. Standard template prostate biopsy found 6 of 14 (42.9%) PC, of which 2 were csPC. PET-guided biopsy identified 8 of 14 (57.1%) PC lesions, of which 5 were csPC. Standard template biopsy was negative in 1 patient, for whom both 68Ga-RM2 and 68Ga-PSMA PET–guided biopsy showed Gleason 3 + 4 cancer.
68Ga-PSMA11 PET/MRI
68Ga-PSMA11 PET/MRI found 25 intraprostatic lesions in the 13 participants (Fig. 1). SUVmax decreased significantly from the whole-body to the dedicated pelvic images, but all lesions were identified at both time points. Biopsy confirmed 11 PC lesions, of which 5 were csPC, 14 FP, and 2 FN (both csPC). The SUVmax of TP lesions was significantly higher than FP on the delayed pelvic but not on the whole-body images. No other statistically significant differences were observed between SUVmax and SUVpeak for 68Ga-PSMA11 PET/MRI, including comparison of csPC and ncsPC. SUV measurements are summarized in Table 2. Sensitivity and specificity were 63% (95% CI, 19, 92%) and 83% (95% CI, 73, 94%), respectively.

Venn diagram of 68Ga-PSMA11 and 68Ga-RM2 positivity with their congruent lesional uptake compared with biopsy results.
SUVmax and SUVpeak of All PET-positive, True-Positive, and False-Positive Lesions, Stratified to Gleason Score at Whole-Body and Delayed Pelvic Imaging for 68Ga-PSMA11 and 68Ga-RM2
68Ga-RM2 PET/MRI
68Ga-RM2 PET/MRI showed 27 intraprostatic lesions in 12 of 13 participants. The participant with a negative 68Ga-RM2 PET result had negative prostate biopsies and was considered TN as cancer of unknown primary was found (FP in 68Ga-PSMA11 PET). No statistically significant changes were found between SUVmax and SUVpeak from whole-body and delayed pelvic images. 68Ga-RM2 PET detected all lesions identified on standard and PET-guided biopsy (14 TP, of which 7 were csPC and 7 ncsPC). There were 13 FP on 68Ga-RM2, of which 12 were the same lesions as on 68Ga-PSMA11. When the SUVmax and SUVpeak of TP and FP lesions were compared, no statistically significant changes were found on whole-body or delayed pelvic images (Table 2). Sensitivity was 83% (95% CI, 40, 97%), whereas specificity was 67% (95% CI, 40, 86%).
Comparison Between 68Ga-PSMA11 and 68Ga-RM2
Concordance between both radiopharmaceuticals was seen in 17 lesions in 11 participants. Of these, 11 lesions were PC, with 6 being csPC (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org). Noncongruent uptake was observed in 14 lesions in 7 patients. Among these, 3 were PC with 1 csPC seen on 68Ga-RM2 (Supplemental Fig. 2), whereas 10 were FP (68Ga-PSMA11 and 68Ga-RM2 each had 5 FP). In 3 patients, a difference in intensity of tracer uptake was observed (Fig. 2). Table 3 gives a semiquantitative measurement (target tumor–to–normal prostate ratio) of lesions for 68Ga-PSMA11 and 68Ga-RM2 PET.

A 58-y-old man presenting with PSA of 12.8 ng/mL and PSA density of 0.41 ng/mL2. (A and B) 68Ga-RM2 (B, axial PET [left-most image], fused PET/MRI [second image], MRI [third image], and maximum-intensity-projection images [right-most image]) shows intense uptake in anterior prostate (red arrows), which is less pronounced on 68Ga-PSMA11 PET/MRI (A). PET-guided biopsy demonstrated Gleason 3 + 4 prostate cancer. (C) Coregistration of biopsy needle tracks are shown in green; index tumor is outlined in red on mpMRI as well as on 3-dimensional–rendered image. A = anterior; P = posterior.
SUVmax and SUVpeak of All PET-Positive Lesions, Normal Prostate Tissue, and TNR for Whole-Body and Delayed Pelvic Imaging for 68Ga-PSMA11 and 68Ga-RM2
No lymph node or other distant metastases were identified on 68Ga-PSMA11 or 68Ga-RM2 PET/MRI.
DISCUSSION
In this pilot study, we evaluated the utility of 68Ga-PSMA11 and 68Ga-RM2 PET/MRI for prostate biopsy guidance in men with suspected PC but negative or equivocal mpMRI results or negative prostate biopsy. In this small cohort, PET-guided biopsy detected more PC lesions than systematic 12-core biopsy, which was not surprising given the plethora of work showing the superiority of mpMRI-guided over standard biopsy (3,4,8). When compared with mpMRI, PET-guided biopsy not only found more TP lesions, but also more importantly, more csPC.
A recently published study explored 68Ga-PSMA617 and 68Ga-RM26 PET/CT for biopsy guidance in 112 men with suspected PC (27). Of these participants, 35% had csPC and 4% ncsPC. Dual-tracer PET/CT-guided biopsy showed the highest detection rate without misdiagnosis of csPC (77%), followed by 68Ga-PSMA617 (70%), 68Ga-RM26 (56%), and mpMRI (36%). Despite the small number of participants and selective cohort, we identified a higher percentage of csPC (7/14 lesions, 50%) and ncsPC (7/14 lesions, 50%). The overall high sensitivity for PET-guided biopsy seen in Qiu et al. (27) was comparable with our study; however, we observed a higher sensitivity for 68Ga-RM2 (83%), leading to the detection of all biopsy-verified csPC and ncsPC with an FP rate similar to that of 68Ga-PSMA11. This might suggest that this specific subgroup of men with negative anatomic imaging despite persistent elevated PSA may have a different tumor biology. PSMA and GRPR expression have been reported as complementary (17,18), with GRPR showing particular overexpression in earlier stages of PC (15). Therefore, GRPR-targeting radiopharmaceuticals may be a suitable alternative for biopsy guidance in men with suspected PC.
68Ga-PSMA11 PET/MRI (sensitivity, 96%; specificity, 81%) showed a better performance than PET/CT (sensitivity, 100%; specificity, 68%) for guiding prostate biopsy (19,20). In this study, sensitivity for 68Ga-PSMA11 was slightly less at 63%, which might be related to the specific subgroup of patients; however, specificity was higher at 83%. These overall high rates for PET/MRI are certainly attributable to the high soft-tissue contrast of MRI but also related to the vast experience in MRI-fusion biopsy. The opportunity of switching from MRI to PET fusion for targeted prostate biopsy enables improved detection rates of csPC, especially in cases for which mpMRI is inconclusive, as seen in this present study. As PET/MRI scanners are not ubiquitously available, software fusion of MRI and PET has been shown to be feasible and demonstrated increased sensitivity of index lesion identification (28).
The PRIMARY trial investigated the added value of combining 68Ga-PSMA11 PET/CT with mpMRI for detecting csPC in men undergoing initial biopsy for suspected PC (29,30). Interestingly, all men with an SUVmax of ≥12 on 68Ga-PSMA11 PET had csPC at biopsy, independent of mpMRI results. In cases of PI-RADS ≥ 4, an SUVmax of ≥9 showed 100% specificity and positive predictive value in csPC detection. In our study, the median SUVmax for csPC on 68Ga-PSMA11 PET was 7. This again could indicate a different tumor biology and expression pattern of PSMA in this specific subgroup of patients or differences in imaging technique.
The SUVmax from 68Ga-RM2 PET was higher than that from 68Ga-PSMA11, but so was the SD for csPC and ncsPC, resulting in no significant differences. Despite earlier reports that GRPR expression is low to none in benign prostatic hyperplasia (BPH) (14,15), we observed uptake in BPH nodules.
We chose to additionally measure SUVpeak because SUVmax is a single pixel value that might be affected by noise (31,32). SUVpeak may be a more robust quantitative measure because of its larger volume (23,33). We did not find any significant differences in SUVpeak between TP and FP lesions or csPC and ncsPC for 68Ga-PSMA11 or 68Ga-RM2. SUVpeak might be a more suitable measure for assessment of treatment response than single-time-point measurements (34).
Prostate biopsy bears an array of risks such as hematuria, rectal bleeding, infection, and pain (35,36). It is critical to identify the patients who will benefit from biopsy and distinguish csPC from indolent cancers. An area of unmet need are men whose mpMRI results are negative or equivocal but who have a high suspicion for PC. These patients usually undergo serial imaging procedures, even multiple biopsies to find the source of their elevated PSA. Our results indicate that a combined approach of 68Ga-RM2 and 68Ga-PSMA11 PET/MRI has high sensitivity and specificity in localizing csPC and may help the urologist making subsequent treatment decisions. The higher upfront cost of such an approach may be cost-effective when compared with subsequent costs in its absence. This needs to be validated in larger studies.
The limitations of this study include the small number of participants, although this is common for pilot studies, and the highly selective patient cohort. However, the latter may be a positive differentiator for the use of PET/MRI in this clinical scenario. The sequence of biopsies performed—PET-guided prostate biopsy first, followed by standard template biopsy—might have affected the results of standard template biopsy due to swelling, bleeding, and tissue distortion.
CONCLUSION
68Ga-PSMA11 and 68Ga-RM2 PET/MRI are feasible for biopsy guidance in men with suspected PC despite negative or equivocal mpMRI results. Both radiopharmaceuticals detected additional csPC not seen on mpMRI. 68Ga-RM2 identified all csPC and ncsPC confirmed at biopsy. The incongruent uptake pattern for 68Ga-PSMA11 and 68Ga-RM2 reflect their different biologic targets and expression. Larger studies are needed to shed light on their respective expression pattern at various stages of PC as well as to guide future clinical use.
DISCLOSURE
The study was partially supported by GE Healthcare. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Are 68Ga-PSMA11 and 68Ga-RM2 PET/MRI useful tools for guiding prostate biopsies in patients with suspected PC despite negative or equivocal mpMRI results?
PERTINENT FINDINGS: 68Ga-PSMA11– and 68Ga-RM2–guided prostate biopsy led to the detection of additional csPC not seen on mpMRI in this selective cohort of patients with prior negative or equivocal mpMRI results or negative prostate biopsy but persistently elevated PSA and PSA density. 68Ga-RM2 PET/MRI accurately identified all csPC and ncsPC confirmed at biopsy.
IMPLICATIONS FOR PATIENT CARE: 68Ga-PSMA11– and 68Ga-RM2–guided prostate biopsy help detecting csPC and might therefore avoid unnecessary biopsies and associated risks.
Footnotes
Published online Nov. 17, 2022.
- © 2023 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication May 24, 2022.
- Revision received November 1, 2022.
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.