


Visual Abstract

Abstract
Spontaneous intracranial hypotension due to spinal cerebrospinal fluid (CSF) leakage causes substantial disease burden. In many patients, the course is protracted and refractory to conservative treatment, requiring targeted therapy. We propose PET of the CSF space with 68Ga-DOTA as a state-of-the-art approach to radionuclide cisternography (RC) and validate its diagnostic value. Methods: This study is a retrospective analysis of patients with suspected intracranial hypotension due to spinal CSF leaks and who underwent whole-body PET/CT at 1, 3, and 5 h after intrathecal lumbar injection of 68Ga-DOTA. Two independent raters unaware of the clinical data analyzed all scans for direct and indirect RC signs of CSF leakage. Volume-of-interest analysis was performed to assess the biologic half-life of the tracer in the CSF space and the ratio of decay-corrected activity in the CSF space at 5 and 3 h (simplified marker of tracer clearance). Comprehensive stepwise neuroradiologic work-up served as a reference; additional validation was provided by surgical findings and follow-up. Results: Of 40 consecutive patients, 39 patients with a working diagnosis of intracranial hypotension due to a spinal CSF leak (spontaneous, n = 31; postintervention, n = 8) could be analyzed. A spinal CSF leak was verified by the neuroradiologic reference method in 18 of 39 patients. As the only direct and indirect diagnostic signs, extrathecal tracer accumulation at the cervicothoracic junction (67% sensitivity and 90% specificity) and lack of activity over the cerebral convexities (5 h; 94% sensitivity and 67% specificity) revealed a high diagnostic value for spinal CSF leaks. Their combination provided little improvement (71% sensitivity and 95% specificity). Additional quantitative analyses yielded no benefit (94% sensitivity and 53% specificity for biological half-life; 94% sensitivity and 58% specificity for the ratio of total radioactivity within the CSF space at 5 and 3 h). The location of direct signs (extrathecal tracer accumulation) did not correlate with verified sites of spinal CSF leakage. Conclusion: We propose CSF PET with 68Ga-DOTA as a novel, fast, and convenient approach to RC for verification but not localization of spinal CSF leaks with high sensitivity and specificity. CSF PET may fulfill an important gatekeeper function for stratifying patients toward escalation (ruling in) or deescalation (ruling out) of diagnostic and therapeutic measures. Further prospective studies are needed to validate the present results and determine the potential of the methods to reduce the burden to patients.
Spontaneous intracranial hypotension (SIH) is an increasingly recognized condition caused by spinal leakage of cerebrospinal fluid (CSF) (1). The clinical situation can be very diverse, especially in individuals with chronic disease, making the diagnosis of SIH difficult (2). Despite its name, it has been reported that only 34%–50% of patients show a low opening pressure on lumbar puncture (2,3). Postural headache and either the presence of stereotypical imaging signs or an opening pressure of <6 cm of H2O is required for the diagnosis (4). Despite conservative therapy (bed rest, caffeine) and epidural blood patches (EBP), symptoms persist in 10%–30% of patients. This situation warrants verification and localization of leakage to allow for targeted treatment (2,5). Typical diagnostic algorithms propose a combination of different imaging modalities, including often repetitive digital subtraction myelography (1), which misses a substantial fraction of leaks (45%–74%) (3). Considering the invasive nature of and possible extensive radiation exposure with these modalities (6), it is desirable to select patients with a high likelihood for a leak before escalating the diagnostic work-up.
The unsurpassed measurement sensitivity of radionuclide imaging techniques and the ability to repeat imaging for hours without causing additional radiation burden underscore the potential of radionuclide cisternography (RC) in this setting. After seminal reports (e.g., Dichiro (7)) and the introduction of 111In-labeled diethylenetriaminepentaacetic acid (DTPA) (8) and 99mTc-DTPA (9), RC gained rapid acceptance in the field, being considered the diagnostic gold standard for the proof and localization of CSF leaks over the years (10–13). Common criticisms of RC, however, include poor image quality and spatial resolution, low sensitivity and specificity, lack of standardization, and long examination (up to 48 h). Despite methodologic improvements, such as cross-sectional imaging with SPECT (14) and hybrid SPECT/CT (15) and quantitative analysis (10,13,16,17), RC was removed from the International Classification of Headache Disorders, third edition, as a diagnostic imaging tool (4). To date, RC is still commonly performed as planar scintigraphic imaging without taking advantage of state-of-the-art imaging, such as PET/CT, which offers improved sensitivity, spatial resolution, and quantification. In fact, CSF PET (e.g., using 68Ga-labeled ethylenediaminetetraacetic acid) was proposed 40 y ago (14) but has only rarely been applied, in single cases (18).
Against this background, in the present study we propose a convenient CSF PET methodology and validate its diagnostic value for the presence and localization of spinal CSF leakage.
MATERIALS AND METHODS
Patients
The University of Freiburg institutional review board approved this study, and all subjects gave written informed consent to the examination and the retrospective analysis. Forty consecutive patients referred for CSF PET because of suspected intracranial hypotension due to a spinal CSF leak between May 2020 and March 2021 were eligible, and 39 could be included (see the Results section).
Reference Standard
Patients underwent a standard work-up, including often repeated cranial and spinal MRI, gadolinium MR myelography, and digital subtraction myelography/CT myelography (supplemental materials, available at http://jnm.snmjournals.org).
Demonstration of a spinal CSF leak by comprehensive neuroradiologic imaging defined the positivity of the target condition (spinal CSF leak) and its localization. This process involved a stepwise approach aimed at localizing or excluding a spinal CSF leak by dynamic digital subtraction myelography followed by dynamic CT myelography in the prone or lateral decubitus position (1). The result served as a reference for the definition of true-positive, true-negative, false-positive, and false-negative results of various PET outcome measures for the presence or absence of a spinal CSF leak (index test). In patients with verified CSF leaks, localizations provided by the reference method and PET (direct signs) were directly compared. Surgical findings (genuine gold standard, applicable only in those with a positive target condition) and clinical follow-up data were also assessed.
PET Acquisition
PET/CT scans (with low-dose or ultra–low-dose CT) covering the entire CSF space were acquired on a fully digital PET/CT system (Vereos; Philips Healthcare) at 1, 3, and 5 h after lumbar intrathecal injection of 68Ga-DOTA (45–50 MBq in 0.5–1.0 mL of saline solution). The preparation of 68Ga-DOTA and the acquisition protocol are described in detail in the supplemental materials.
Visual PET Readings
Two experienced nuclear medicine physicians, unaware of all other clinical and diagnostic data as well as the results of quantitative PET analyses, evaluated all 68Ga-DOTA PET scans independently. Using the 1-, 3-, and 5-h PET/CT datasets, visual readings of direct and indirect RC signs were done and a summary rating was assigned using a 3-step scale (0, none; 1, questionable/mild signal; 2, strong signal) (the supplemental materials provide details).
Direct signs of a spinal CSF leak included uni- or bilateral extrathecal tracer accumulation, witnessed at least at 1 time point and localized according to 28 spinal segments. Extrathecal tracer accumulations in multiple consecutive segments were rated in combination, assuming that they stemmed from the same process.
Indirect signs of a spinal CSF leak included radiotracer accumulation in the bladder (1 h) and radiotracer accumulation in the basal cisterna and over the cerebral convexities. In addition, iatrogenic tracer extravasation at the injection site was assessed.
Finally, a 3-step summary rating was independently recorded by each rater for each individual case (0, 1, and 2 for no, questionable/possible, and probable CSF leakage, respectively). After discussion of discrepant cases, the raters reached a consensus.
Quantitative PET Analysis
The time course of total radioactivity within the CSF space was characterized in terms of biologic half-life (t1/2,biol) and, as a simplified approach, using the ratio of total radioactivity within the CSF space at 5 and 3 h (R5/3; decay-corrected data). Volume-of-interest analyses were performed after coregistration of all 3 PET/CT scans in each patient (supplemental materials).
Statistical analyses are provided in the supplemental materials.
RESULTS
Patient Characteristics
Forty consecutive patients (age, 46.2 ± 14.1 y, 32 women and 8 men) were eligible. Thirty-two patients were diagnosed with SIH (4) (in 1 patient, spinal puncture failed, leaving 31 patients), 4 had a possible persistent/relapsing CSF leak after previous open surgical treatment for SIH, and 4 had questionable SIH; in the latter, a former lumbar puncture or peridural anesthesia was assumed by the referring doctor to be causal. For 37 of 39 included patients (95%), data from a follow-up at 3.6 ± 2.5 mo were available. CSF PET was well tolerated by all patients. There were no side effects, except for those commonly associated with lumbar puncture.
In 18 of 39 patients (46%), stepwise neuroradiologic imaging localized a spinal CSF leak at C7–T3 (n = 6) or T7–L1 (n = 12) (Suppl. Fig. 1) (supplemental materials are available at http://jnm.snmjournals.org). CSF leaks were only verified in patients with SIH but without previous surgery or alternative causes (detection rate, 18/31 [58%]). A ventral dural tear was found in 12 patients (coinciding with a microspur on surgery in 9 patients), whereas a lateral leak and a direct CSF venous fistula were diagnosed in 3 patients each. Except for 1 patient, who refused surgery and was successfully treated with untargeted EBP, all patients with proven leaks underwent surgery; symptom improvement (n = 10) or resolution (n = 6) was seen in 16 of 17 patients (94%). In the remaining patient, a 60-y-old man with long-standing symptoms, cerebral MRI findings of SIH markedly improved while symptoms remained unchanged.
Of the 21 patients in whom no leak could be identified, 15 were treated with EBP. Follow-up data, which were available for 14 of these 15 patients (27 EBP in total), showed an improvement or resolution of symptoms in only 2 patients each (response rate, 4/14 [29%]). The remaining patients either refused treatment or received alternative diagnoses and treatments. Taken together, the clinical outcomes strongly support the validity of the neuroradiologic reference standard.
Visual PET Readings
Visual readings (examples are shown in Figs. 1⇓–3 and Suppl. Fig. 2) of direct signs of a spinal CSF leak were highly consistent between both raters (agreement in 86% of ratings; supplemental materials). Supplemental Figure 1 summarizes the sites of extrathecal tracer accumulation. The findings clustered at the craniocervical and cervicothoracic junctions (Fig. 3), over the lower thoracic spine, and in the lumbosacral region (Suppl. Fig. 1). To further analyze the data, we sorted all sites of extrathecal tracer accumulation in these regions (selecting the most prominent if >1 site) (Table 1). Extrathecal tracer accumulation at the craniocervical and cervicothoracic junctions showed no significant dependence on scan time, whereas that in the lower thoracic spine and lumbosacral region decreased significantly with time (supplemental materials).

Normal CSF PET in patient without verified spinal CSF leak. (A) Maximum-intensity projections of PET images (posterior view; scaled for optimal display) at 1, 3, and 5 h after injection of 68Ga-DOTA and sagittal PET/CT fusion image (at 5 h; far right). (B) Transaxial PET slices at level of centrum semiovale at 1, 3, and 5 h and PET/CT fusion image (far right). Note time-dependent cephalad ascent of tracer with normal accumulation of activity over cerebral hemispheres. Patient (no. 38) was treated with epidural blood patch, without response.

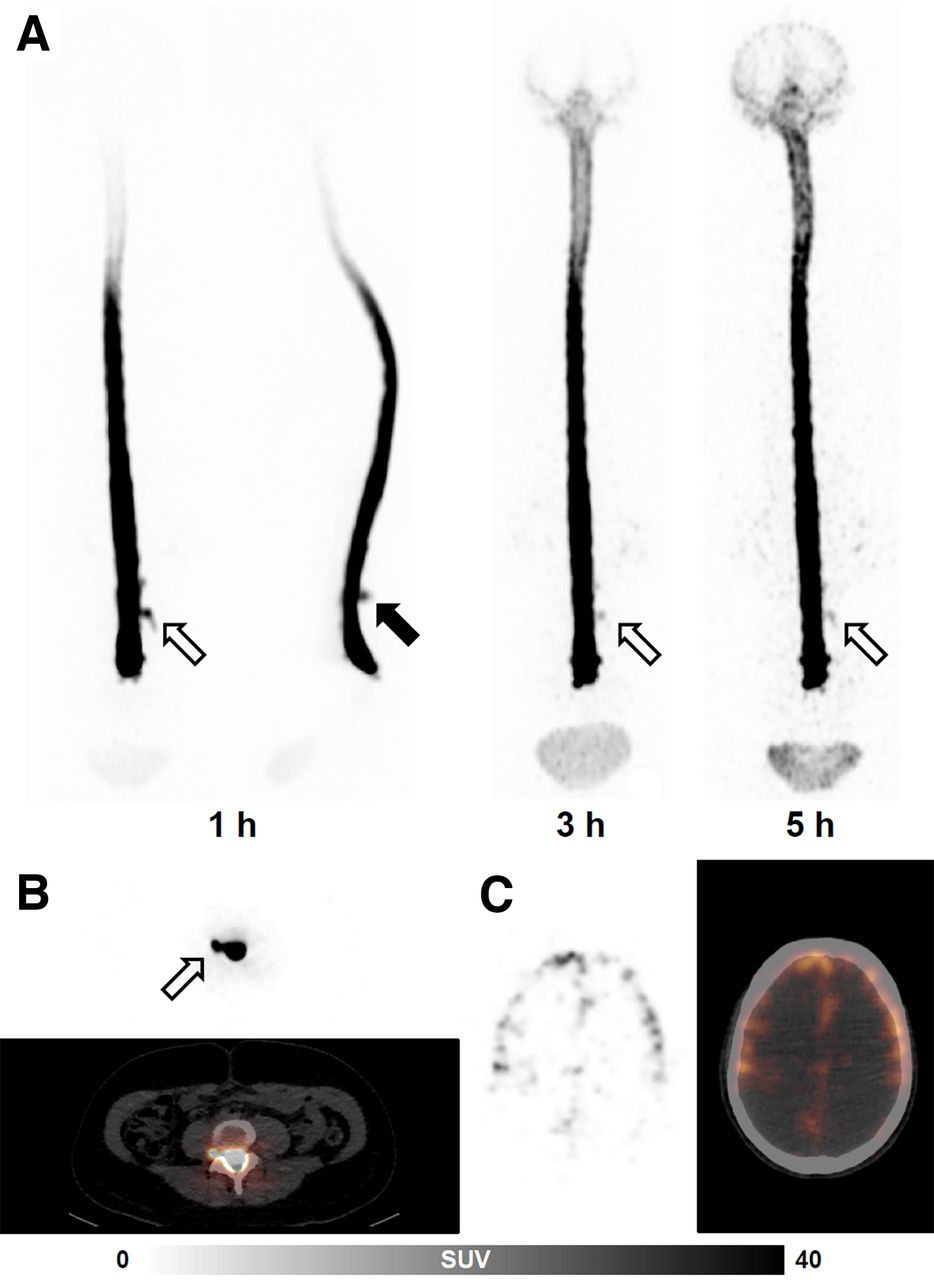
CSF PET with iatrogenic extrathecal tracer accumulation in patient without verified spinal CSF leak. (A) Maximum-intensity projections of PET images at 1, 3, and 5 h (posterior view and, at 1 h, lateral view as well; scaled for optimal display) after injection of 68Ga-DOTA. (B and C) Transaxial PET and PET/CT fusion images at levels of L3–L4 (1 h; B) and centrum semiovale (5 h; C). Although strong iatrogenic egression of tracer that was observed in trajectory of injection needle (filled arrow) and to right side at levels of L3–L4 (open arrows) vanished with time, cephalad ascent of tracer was normal, with tracer accumulation over cerebral convexities. Patient (no. 15) was treated with epidural blood patch, without response.

Pathologic CSF PET in patient with verified spinal CSF leak. (A) Maximum-intensity projections of PET images at 1, 3, and 5 h (posterior view; scaled for optimal display) after injection of 68Ga-DOTA. (B) Transaxial PET and PET/CT fusion images at levels of C7–T1 and C2 (3 h), respectively. Compatible with surgically verified, lower thoracic lateral CSF leak, there were moderate and mild extrathecal tracer accumulations at level of cervicothoracic junction (open arrows) and in upper cervical region (filled arrows), respectively. There was a lack of tracer accumulation over cerebral convexities (asterisk). Patient (no. 27) was treated by surgery, with improvement of symptoms.
Results of Visual and Quantitative PET Analyses
Mean ratings (across raters and scans) of direct signs at the lower thoracic spine and in the lumbosacral region did not differ between patients without and patients with verified spinal CSF leaks, whereas in the cervicothoracic junction there was a highly significant difference between the groups. This finding allowed for an accurate diagnostic separation of groups (receiver operating characteristic [ROC] area under the curve [AUC], 0.81; 67% sensitivity; 90% specificity; cutoff, 0.33; i.e., mild extrathecal tracer accumulation in at least 1 scan) (Table 1). Extrathecal tracer accumulation at the craniocervical junction was rarely observed (3/39 patients) and occurred only in patients with verified spinal CSF leaks (P = 0.055). There was no obvious association between the location of verified spinal CSF leaks and extrathecal tracer accumulation on PET. In fact, sites of extrathecal tracer accumulation usually extended over multiple segments and overlapped the site of a verified leak in only 3 of 18 patients (locations differed by only 1 segment in 3 patients and by >1 segment in 12 patients) (Suppl. Fig. 1).
Ratings of indirect signs of CSF leakage and tracer extravasation at the injection site were also highly consistent between observers (agreement on 80%–85% of ratings; supplemental materials). Ratings for the basal cisterna and tracer accumulation over the cerebral hemispheres showed a significant increase with time and dependence on the presence or absence of a spinal CSF leak, whereas tracer extravasation at the injection site decreased significantly with time (supplemental materials).
The only indirect sign that showed a highly significant difference between patients without and patients with verified spinal CSF leaks was a lack of tracer accumulation over the cerebral hemispheres on the 5-h scan. This finding allowed for an accurate diagnostic group separation (ROC AUC, 0.79; 94% sensitivity; 67% specificity; cutoff, >1.0; i.e., more than only mild tracer accumulation over the cerebral hemispheres at 5 h) (Table 1).
Considering all direct and indirect signs, both raters also filed a summary score that was highly consistent between raters (agreement in 77% of cases; Supplement). The consensus rating of both raters yielded a highly significant group difference between patients without and patients with verified spinal CSF leaks (0.43 ± 0.68 vs. 1.39 ± 0.78; P = 0.0006; ROC AUC, 0.80; 83% sensitivity; 67% specificity; cutoff, 1) (Table 1).
Similar results were obtained when analyses were restricted to patients with SIH but without previous surgery or alternative causes (Suppl. Table 1).
Quantitative PET Analysis
Quantification was omitted in 2 patients because of partial epidural tracer injection and out-of-field-of-view artifacts (both scans were still read visually). As expected, t1/2,biol and R5/3 were highly correlated (rho, 0.94; P < 0.0001). t1/2,biol and R5/3 showed no significant association with age, sex, body weight, or body height, either in the entire group or in the patients with and the patients without verified spinal CSF leaks. However, t1/2,biol and R5/3 were significantly lower in patients with than in patients without spinal CSF leaks (Table 1). This finding allowed for a diagnostic group separation (for t1/2,biol: ROC AUC, 0.70; 94% sensitivity; 53% specificity; cutoff, <7.9 h; and for R5/3: ROC AUC, 0.78; 94% sensitivity; 58% specificity; cutoff, <0.82).
Combination of Qualitative and Quantitative Analyses
We used stepwise forward regression, including aforementioned significant parameters with the exception of t1/2,biol (highly correlated to R5/3), to explore which combined parameters best predicted a spinal CSF leak. A minimum Akaike information criterion (36.3) was reached by retaining extrathecal tracer accumulation at the cervicothoracic junction and a lack of tracer accumulation over the cerebral hemispheres (for the resulting multinomial logistic regression model: ROC AUC, 0.88; 71% sensitivity; 95% specificity).
DISCUSSION
We propose CSF PET with 68Ga-DOTA as a novel, state-of-the-art approach to RC that provides several possible advantages over conventional RC. By using a very rigorous diagnostic reference standard in an exceptionally large cohort of patients, we were able not only to validate the diagnostic accuracy of CSF PET for verifying—although not localizing—spinal CSF leakage but also to unravel several misconceptions and controversies concerning RC.
PET provides better spatial resolution (2–3 times higher) and sensitivity (2–3 magnitudes higher) than scintigraphy and SPECT (19), allowing the detection and quantification of the slow cephalad ascent of CSF even with short-lived radionuclides. The entire examination is completed within 5–6 h; in contrast, conventional RC often takes up to 48 h. In addition, individual PET scans are acquired within 20–30 min—thus comparing favorably with whole-body SPECT/CT examinations, which may take up to 1 h. The estimated dose for CSF PET with 68Ga-DOTA is approximately 1.24 mGy/MBq for the spinal cord (highest organ dose), and the effective dose equivalent is 0.16 mSv/MBq; these doses are slightly higher than those for 111In-DTPA (0.95 mGy/MBq and 0.14 mSv/MBq, respectively, assuming the same biokinetic model for both tracers [normal t1/2,biol] and accounting for differences in energy transfer and physical half-lives) (20). Thus, for a typical injected dose of 37 MBq of 68Ga-DOTA, the estimated effective dose is 5.9 mSv. CT scans add about 3–4 mSv, which may be further reduced with dose-sparing techniques. The fast decay of 68Ga-DOTA (as opposed to 111In-DTPA) also implies that there is no relevant radiation exposure to medical personnel if patients undergo spinal surgery shortly after diagnostics (often on the following day at our institution). The synthesis and quality control of 68Ga-DOTA are also very simple and readily available at most larger centers (at least in Europe), rendering it a convenient alternative to 111In-DTPA. Finally, the high image quality of PET/CT scans renders CSF PET with 68Ga-DOTA much more appealing and convincing than conventional RC—factors that, in our experience, strongly improve the acceptance of RC in clinical routines.
The average t1/2,biol for patients without verified leakage (9.5 ± 7.0 h) is somewhat lower than but still in line with that in the literature (13.5 ± 4.5 h) (10), considering that this group possibly includes patients with missed or iatrogenic leaks. We propose R5/3 as a simpler estimate of tracer clearance, circumventing the need for a 1-h scan and exponential fitting, with slightly higher diagnostic performance. However, quantitative analyses provided no additional benefit over visual readings, in line with findings for conventional RC (21). Still, we routinely perform quantification as a simple adjunct to visual reading, an approach that may be particularly valuable for follow-up assessments (10).
A particular strength of the present study is the use of a rigorous neuroradiologic reference standard that was additionally validated by surgical findings and outcomes. To the best of our knowledge, no previous study on RC included more patients with appropriate verification (e.g., in the seminal work by Schievink et al. (22), correlation of RC with CT myelography and surgery was available for only 8/11 and 4/11 patients, respectively), with earlier studies often using response to EBP as a reference (10,16,23,24). However, given the uncertainty about the efficacy and mechanism of action of EBP (e.g., success sometimes only after several attempts, targeted vs. nontargeted EBP, often only short-term efficacy, possible placebo effects) (25) as well as the current, improved understanding of SIH pathophysiology (see later text) (3,26–28), we are convinced that the reference standard in current use is the most appropriate. We were able to verify a spinal CSF leak in 18 of 31 patients (58%) with SIH but without previous surgery or alternative causes. Although a few spinal leaks may have been missed (see later text), this fraction is in line with those in the literature (3) and underscores the uncertainty associated with the clinical diagnosis of SIH, which does not require verification of a leak (4).
We made several important observations. First, the site of extrathecal tracer accumulation on CSF PET was not related to the actual location of leakage—something that has not been systematically shown before. We do not believe that this finding is related to the tracer used (e.g., later detection of actual sites of leakage with longer-lived isotopes) but assume that it represents a general shortcoming of RC. In fact, patterns observed in the present study and described in the literature are very similar. However, unlike investigators in earlier studies, we used a rigorous diagnostic reference standard that was a prerequisite for detecting this mismatch. Second, 68Ga-DOTA PET, like conventional RC (10,12,13,17,24), may show several sites of extrathecal tracer accumulation—which, however, do not indicate that there are multiple leaks but rather that the tracer leaves the spinal epidural space at multiple locations. This notion is in line with the current concept that spontaneous spinal CSF leaks most commonly occur in the lower cervical spine and thoracic spine (22,26), frequently being caused by well-defined singular lesions (e.g., dural tears due to diskogenic microspurs) (3,26,27). Thus assumption is also reflected by current excellent surgical outcomes. Third, lumbar/lumbosacral extrathecal tracer accumulations are very rarely (if ever) indicative of leaks in that region but are usually of iatrogenic origin instead, although frequently being reported in the RC literature (10,23). Fourth, early bladder activity as an indirect sign possesses little (if any) diagnostic value, in contrast to early RC reports (11) but in agreement with more recent studies (17,21). Fifth, the term direct sign for extrathecal tracer accumulation in the paraspinal space in RC is most likely misleading. In fact, the only direct signs associated with verified leaks in the present study were probably RC equivalents of cervicothoracic extrathecal fluid accumulation on x-ray myelography, commonly referred to as false localizing signs (29). We assume that this finding is simply due to anatomic reasons (e.g., more flexible spinal alignment). To the best of our knowledge, no other systematic studies have provided a detailed (segmental) comparison of neuroradiologic or surgical and RC findings. Even in the aforementioned seminal work (22), anatomic description of CT myelography or RC findings did not pinpoint locations of actual leaks but only provided approximate segmental heights or ranges of extrathecal findings. Given rapid epidural spread and the uncertain mechanism of action of EBP (see earlier text), a therapeutic response to EBP can hardly be taken as a confirmation of an apparent leak localization given by RC, as has frequently been done in the literature (22–24).
CSF PET shows high diagnostic performance in a particularly challenging clinical situation. Extrathecal tracer accumulation at the cervicothoracic junction provides a high diagnostic specificity (90%) but only a moderate sensitivity (67%) for the verification of spinal CSF leaks. The latter fits the observation that direct signs of CSF leakage on conventional RC might be absent in a highly variable fraction of patients with SIH (10%–70%) (13,22–24). In turn, indirect signs of CSF leakage on conventional RC are found in the vast majority (>90%) of patients (11,13,22,24). A lack of tracer appearance over the cerebral convexities on a 5-h scan provides a very high sensitivity (94%) at a moderate specificity (67%). A very high sensitivity of this sign was also suggested by conventional RC studies (13,17,21). The summary rating of both raters was motived by clinical practice with conventional RC and comprised all direct and indirect signs (including those of no or little value), with weighting left to the discretion and experience of the rater. Thus, it is not surprising that this consensus reading was not superior to a combination of both aforementioned features by logistic regression.
Given the considerable rate of negative findings of CT and MR myelography in SIH (45%–74%) (3), it is interesting that 4 of 14 patients (29%) with negative neuroradiologic imaging results and treated with EBP showed a clinically relevant response to EBP. All 4 patients fell into the groups of patients who were judged to show “questionable/possible” and “probable” (2 patients each) signs of a spinal CSF leak but in whom no leak could be verified (Suppl. Figs. 1 and 2). Aside from direct and indirect signs suggestive of spinal CSF leaks (in 3 patients and 1 patient, respectively), all 4 patients also showed below-threshold t1/2,biol and R5/3 values. Thus, it is tempting to speculate that these patients represented false-negative cases on neuroradiologic imaging, leading to an underestimation of the true sensitivity of CSF PET.
In light of these observations, the clinical role of CSF PET is clearly not to localize the site of a spinal CSF leak. CSF PET may, however, play an essential role in verifying spinal CSF leakage with high sensitivity (to rule out) or specificity (to rule in), depending on clinical need. For instance, extrathecal tracer accumulation at the cervicothoracic junction is most likely associated with a spinal CSF leak (90% specificity) and may prompt additional examinations. In turn, sufficient tracer accumulation over the cerebral convexities strongly argues against a spinal CSF leak (>90% sensitivity), leading to a defensive approach (see also Mokri (21)). One motivation would clearly be to minimize the exposure to ionizing radiation in a predominately young and female population. Patients have a long disease history of months to years and have already undergone a plethora of diagnostic and therapeutic actions. In the present study, on average, 2 combined digital subtraction myelography/CT myelography procedures were performed per patient at our institution only. The resulting median radiation exposure in the present study can be estimated to be about 52.6 mSv per patient (6) or, in other words, enough to cause 1 additional radiation-induced cancer death in 250–500 patients (30). This risk may be substantially reduced by including a gatekeeper examination.
The limitations of the present study include its retrospective nature, which warrants prospective validation. In particular, a direct comparison of CSF PET with conventional RC would be desirable (e.g., by coinjection of tracers). Furthermore, the limited number of cases did not allow for detailed statistical contemplation of interesting subgroups (e.g., SIH vs. non-SIH, type of leakage). Finally, the present study summarized the data for the first patients examined with this novel methodology that was developed in parallel. By retrospectively analyzing the data for this set of patients at once in a strictly masked fashion, we minimized possible effects of the raters’ learning curves and bias. However, optimal technical aspects, such as measures to avoid iatrogenic extrathecal tracer accumulation, still need to be defined. Moreover, although an earlier study showed that upright positioning or exercise does not affect CSF circulation under normal conditions (7), a preliminary report of 2 cases suggested that a sitting position may improve the rate of detection of spinal CSF leaks (31). Further studies are needed to explore whether such efforts or other technical refinements can increase the rate of detection of CSF leakage and possibly improve the localization of spinal CSF leaks by PET.
CONCLUSION
We propose CSF PET with 68Ga-DOTA as a novel, fast, and convenient approach to RC for verification but not localization of CSF leaks with high sensitivity and specificity. CSF PET may fulfill an important gatekeeper function for stratifying patients toward escalation (ruling in) or deescalation (ruling out) of diagnostic and therapeutic measures. Further prospective studies are needed to validate the present results and determine the potential of the methods to reduce the burden to patients.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is CSF PET with 68Ga-DOTA a valid method for the diagnosis of spinal CSF leakage when compared with comprehensive, stepwise neuroradiologic imaging?
PERTINENT FINDINGS: The present retrospective study included 39 consecutive adults with suspected intracranial hypotension and who underwent 68Ga-DOTA CSF PET. Extrathecal tracer accumulation at the cervicothoracic junction (67% sensitivity and 90% specificity) and lack of activity over the cerebral convexities (5 h; 94% sensitivity and 67% specificity) revealed a high diagnostic value for spinal CSF leaks.
IMPLICATIONS FOR PATIENT CARE: CSF PET with 68Ga-DOTA may serve as a gatekeeper for stratifying patients toward escalation or deescalation of further diagnostic and therapeutic measures and, thus, reducing the burden to patients.
Footnotes
Published online Aug. 18, 2022.
- © 2023 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication February 23, 2022.
- Revision received August 13, 2022.





{kind=link}
{kind=link}
{kind=link}
{kind=link}