


Abstract
Fluorescence imaging is an emerging imaging technique that has shown many benefits for clinical care. Currently, the field is in rapid clinical translation, and an unprecedented number of clinical trials are performed. Clinicians are inundated with numerous opportunities and combinations of different imaging modalities. To streamline this process, a multidisciplinary approach is needed with drug discovery, software and systems engineering, and translational medicine. Here, we discuss the main constituents of a uniform fluorescence imaging protocol to match the clinical need and ensure consistent study designs and reliable data collection in clinical trials. In an era in which the potential of fluorescence imaging has become evident, consistent conduct of studies, data analysis, and data interpretation is essential for implementation into the standard of care.
Wide-field fluorescence imaging (FI) is a rapidly evolving imaging technique. By probing optical contrast, FI visualizes biochemical, physiologic, or pathophysiologic processes that human vision cannot detect (1). In medicine, and specifically in surgery, the potential of FI has been shown for nontargeted indications such as assessment of tissue perfusion, retinal vasculature, and sentinel lymph node mapping (2–5). Efforts to improve the specificity of the signal have led to the development of targeted FI for the detection of malignant or premalignant lesions and locoregional metastases (e.g., lymph node or peritoneal metastases), delineation of tumor margins, evaluation or prediction of treatment response, and, more recently, visualization of critical anatomic structures, such as nerves (6–10). Although the field has grown exponentially in FI camera system performance and fluorescent tracers, broad implementation into the standard of care has not yet been established (11–13).
Currently, the first phase II and III trials are being reported—overviews of currently ongoing clinical trials have been presented recently (12,14), and the first Food and Drug Administration breakthrough therapy designation has been assigned for use in breast cancer surgery (15). As such, the number of clinicians having access to FI camera systems (e.g., surgical robot–assisted systems with incorporated FI) is also rapidly increasing. Choosing the appropriate imaging approach for a clinical problem is based on the strengths and weaknesses of the available FI imaging systems and fluorescent tracers. This requires a basic understanding of the underlying physics of FI and the chemistry of the fluorescent tracers used.
Swift implementation of FI into the standard of care requires a multidisciplinary approach, which is especially important when conducting a clinical study with FI. We strongly advise clinicians to partner with FI experts (e.g., engineers, physicists, and chemists) in early phases of trial design. The fluorescent tracer and FI camera system must be chosen carefully. Perhaps most importantly, it requires the users to be cognizant of both the drug and device limitations for clinical use. The protocol should result from multiple constituents, such as clinical indication, applied FI camera system, target moiety, signaling compound, standardized imaging acquisition, data processing, and, finally, image interpretation. An inadequate imaging approach leads to a flawed clinical trial or individual imaging procedure but, more importantly, comes with unnecessary patient risk and societal burden. These risks include elongated anesthesia and operation time, unnecessary health-care costs, and exposure to novel compounds without a fully elucidated pharmacologic profile.
Clinical FI studies should be based on a scientifically substantiated imaging approach that relies on the cornerstones of science, standardization, and reproducibility. This paper aims to provide a guideline for clinicians who want to perform wide-field FI trials that lead to clinical implementation or for translational research and development.
DEFINING THE CLINICAL INDICATION AND IDENTIFYING THE APPROPRIATE TARGET
The driving motivator for a new trial is a clinician with a clinical challenge and the desire to test a new optical imaging approach, potentially leading to the birth of a new relevant application. In contrast to radiographic imaging techniques, FI can be seamlessly integrated into the standard of care. It relates directly to the surgeon’s vision and uses portable and relatively low-cost instrumentation, nonionizing radiation, and real-time feedback (16). Yet, the clinician needs to think of the clinical value and practical issues. For example, an urgent surgical procedure requires fluorescent tracers that accumulate rapidly at the target site.
When such practical issues have been addressed, a more refined imaging approach can be developed (Fig. 1). FI imaging in the visible spectrum (e.g., fluorescein or methylene blue) is often not sufficient because of its low penetration depth resulting from strong photon absorption in this spectrum. Most clinical indications require assessment of subsurface structures (i.e., >1 mm), with the absorption and scattering of light being the main limiters of penetration depth. The user should be aware of the tissue of interest’s optical properties (i.e., scattering and absorption) and its impact on light propagation (17). Tissue types exhibit specific optical properties; for example, more absorption occurs in a highly vascularized liver than in muscle tissue. Penetration depth can be improved by imaging in the near-infrared window (i.e., 750–1,700 nm). This spectral region benefits from reduced scattering and lowest absorption by tissue chromophores (e.g., hemoglobin and water). A critical note here is that the signal is heavily surface-weighted because of light attenuation in tissue (i.e., absorption and scattering) and that the spatial resolution decreases with depth because of scattering (Fig. 2) (18).

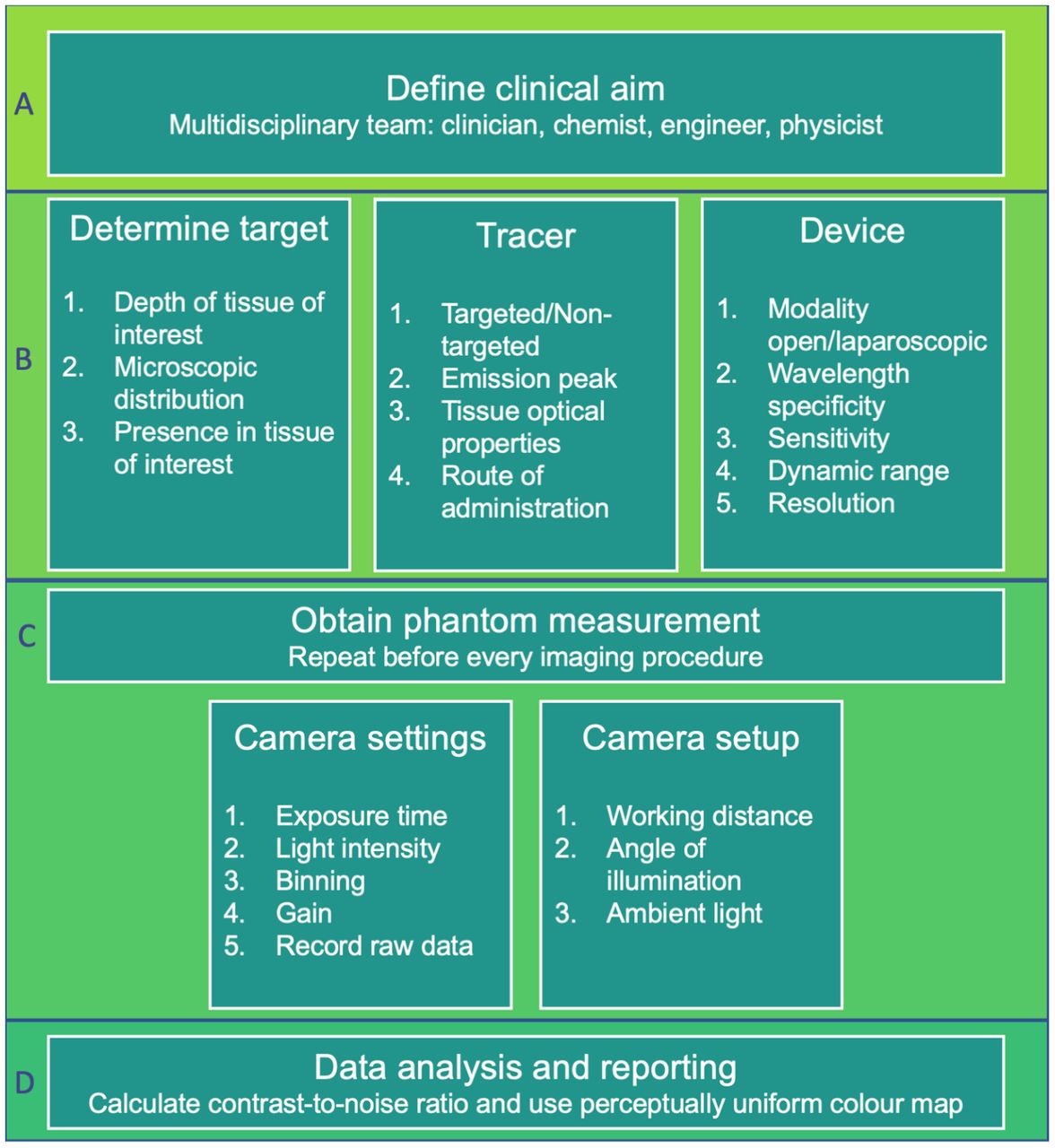
Checklist for performing in vivo FI studies. Step-by-step approach is used to ensure standardized and reproducible FI clinical trial, including trial design, imaging acquisition, data analysis, and reporting results. First, clinician involved should define clear and specific clinical aim in close cooperation with chemist, engineer, and physicist. Team then defines biologic target with microscopic distribution and required penetration depth in mind. Tracer must match target and should be selected on basis of targeted or nontargeted approach, tracer’s emission peak, tissue optical properties, and administration route. Simultaneously, device emission and excitation filters must match tracer’s wavelength. Also, form factor should be determined, along with desired resolution, sensitivity to light, and dynamic range. Before every imaging procedure, phantom measurements should be obtained to evaluate performance characteristics over time. User should set camera settings such as exposure time, binning, gain, and emission light intensity, and data should be recorded without any preprocessing. Moreover, camera setup should be identical in every procedure, with respect to working distance, angle of illumination, and ambient light levels, to compare results across patients. After data analysis, performance of fluorescent tracer and imaging device combination should be reviewed on basis of CNR ratio. Images should be processed using perceptually uniform color maps.
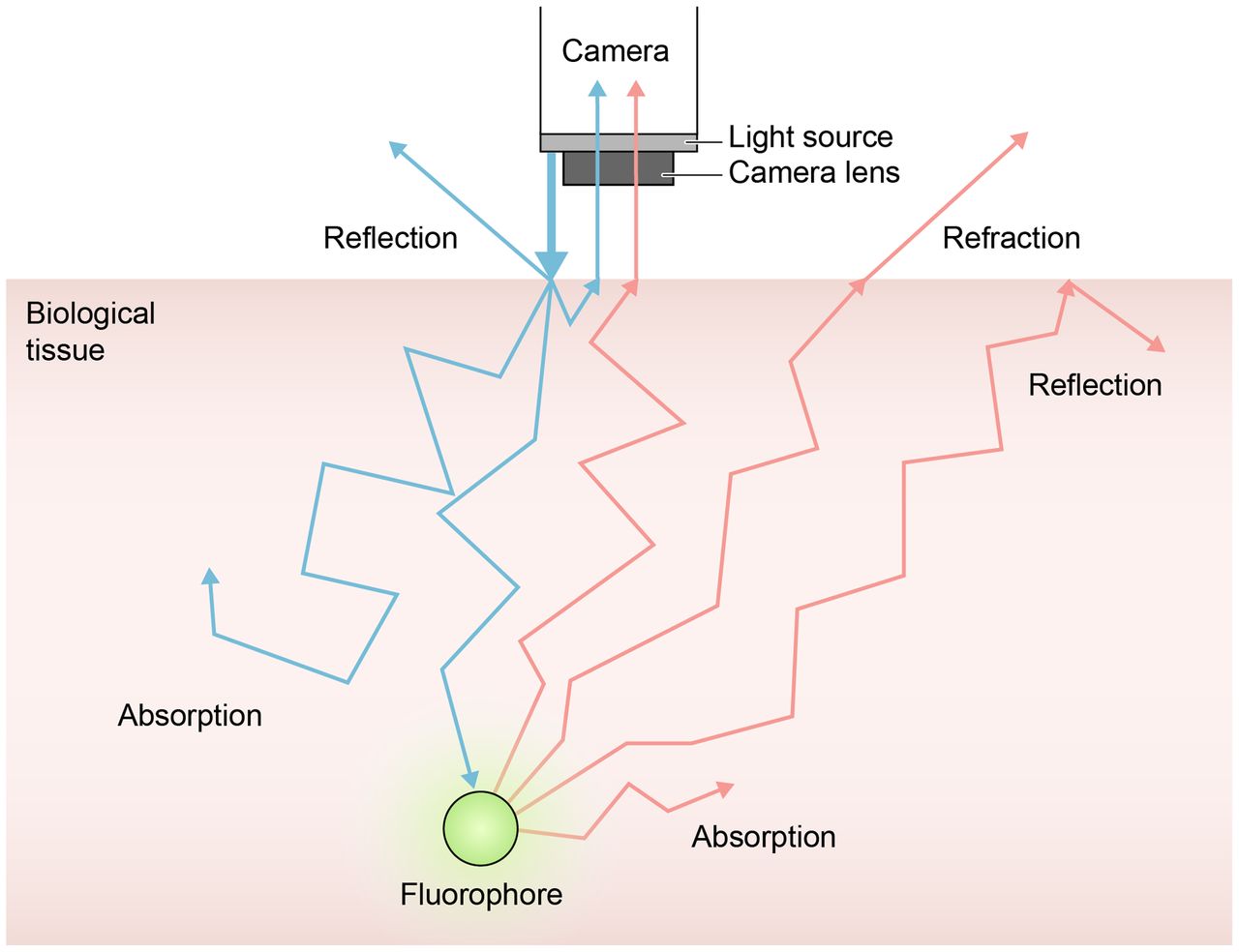
Basic principles of fluorescence and tissue optical properties. Fluorescent contrast generation starts with illuminating tissue at appropriate wavelength for excitation of fluorophore (i.e., endogenous or exogenous contrast). Fluorophore is excited from ground state to excited state by short-lived light absorption. Immediately after excitation, fluorophore relaxes to lower energy state and emits light of lower energy and longer wavelength than excitation light. Emitted light propagates out of tissue and is detected by fluorescence detector, which converts recorded light into image demonstrating number of photons detected. Light propagation and imaging depth are limited by tissue optical properties. Absorption causes light energy to be transferred to tissue, decreasing light intensity. Scattering is process of short-lived absorption of photon (typically) without energy loss but with change of initial direction. Also, scattering decreases ability to distinguish details. If there is no correction for tissue optical properties, signal registered is rather qualitative than quantitative.
When the user is aware of the tissue of interest’s optical properties, the biochemical phenomenon or the physiologic or pathophysiologic process should be concretized. All possible targets, including biomarkers and phenomena or processes, should be examined to determine which is most suitable for localization or evaluation of the target tissue. For example, one can image breast cancer through visualizing nonspecific intratumoral phenomena (e.g., enhanced permeability and retention effect), a specific cell membrane–bound receptor, or a pathophysiologic phenomenon in the tumor microenvironment. Methods for target selection have been reported previously (19,20). Briefly, the potential target should prevail in the target tissue compared with directly adjacent tissue, benefiting high binding sensitivity and specificity as well as improving the contrast. Target expression is commonly determined by immunohistochemistry. However, it is increasingly questioned whether the target is representative of the complete tumor because of tumor heterogeneity and variations in target expression over time. Data-driven methods based on genomic alterations are studied to identify and prioritize relevant targets for clinical trials (21). In addition, many targets (e.g., cell membrane receptors) are present in a microscopically heterogeneous pattern. For solid tumors that require wide local excision, the latter does not per se impede guiding the surgeon in tumor resection since the margin is of primary interest (22–24). In contrast, in debulking surgery procedures (e.g., glioblastoma surgery), homogeneous contrast is of clinical importance since microscopic residues should be identified in order to excise all tumor tissue (25,26).
SELECTION OF THE APPROPRIATE IMAGING MODALITY
When selecting FI camera systems for a clinical trial, the system’s form factor must fit in the expected clinical setting. For instance, in oral cancer, tumors can be visualized using an open system, but perfusion assessment during minimally invasive surgery requires a laparoscopic system. Next, the user should be aware of the system’s performance characteristics to obtain the desired imaging data, as these parameters greatly affect the results (11). There are numerous parameters to consider, but one should focus on those that directly influence imaging data, such as the camera detection sensitivity to the desired tracer, depth sensitivity, field illumination homogeneity, spatial and temporal resolution, and dynamic range. These minimum requirements for these parameters should be fine-tuned for a specific imaging study, preferably in cooperation with an engineer and a physicist.
The camera detection sensitivity describes the ability of an FI camera system to detect a certain concentration of a specific contrast (i.e., fluorescent dye and corresponding emission wavelength). This determination should be made for every combination of an FI camera system and a fluorescent tracer since the system’s foremost influential characteristic is the sensitivity to the fluorescent tracer’s emission peak. Commercially available FI camera systems are equipped with specific narrow-band optical filters. A mismatch between the optical filters and the fluorescent tracer results in a low fluorescence intensity and could lead to an erroneous conclusion that a fluorescent tracer dose or microdose does not accumulate in the region of interest since the contrast-to-noise ratio (CNR) is low (Fig. 3B).
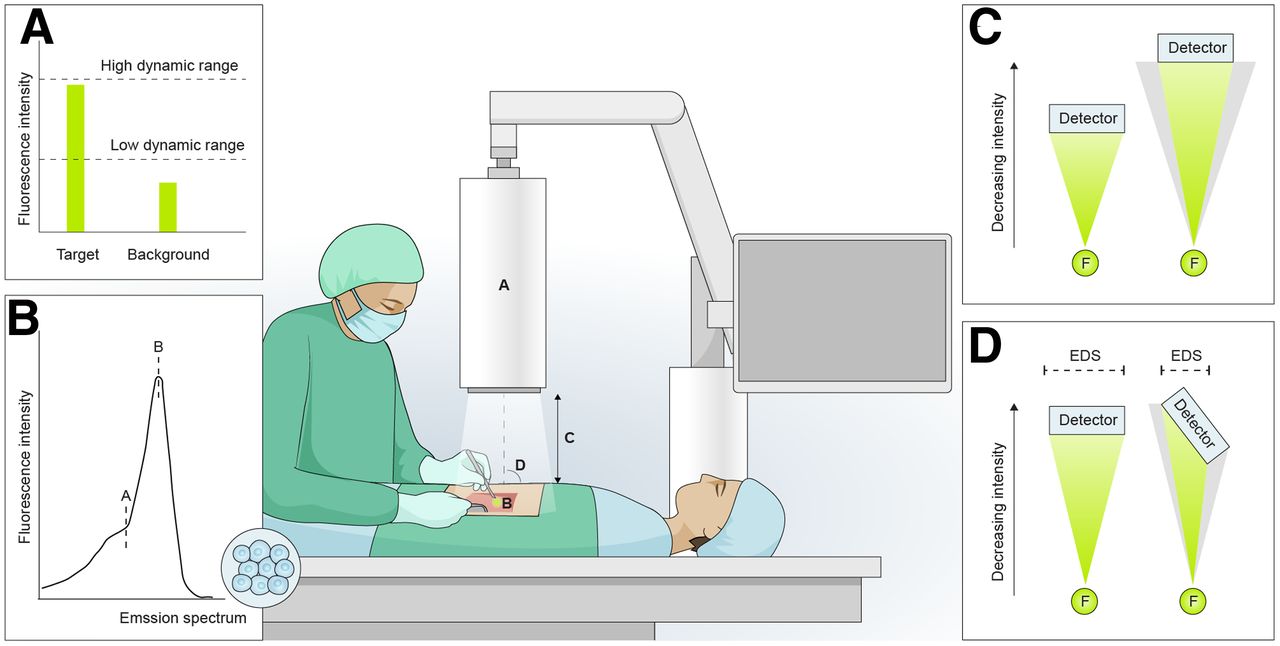
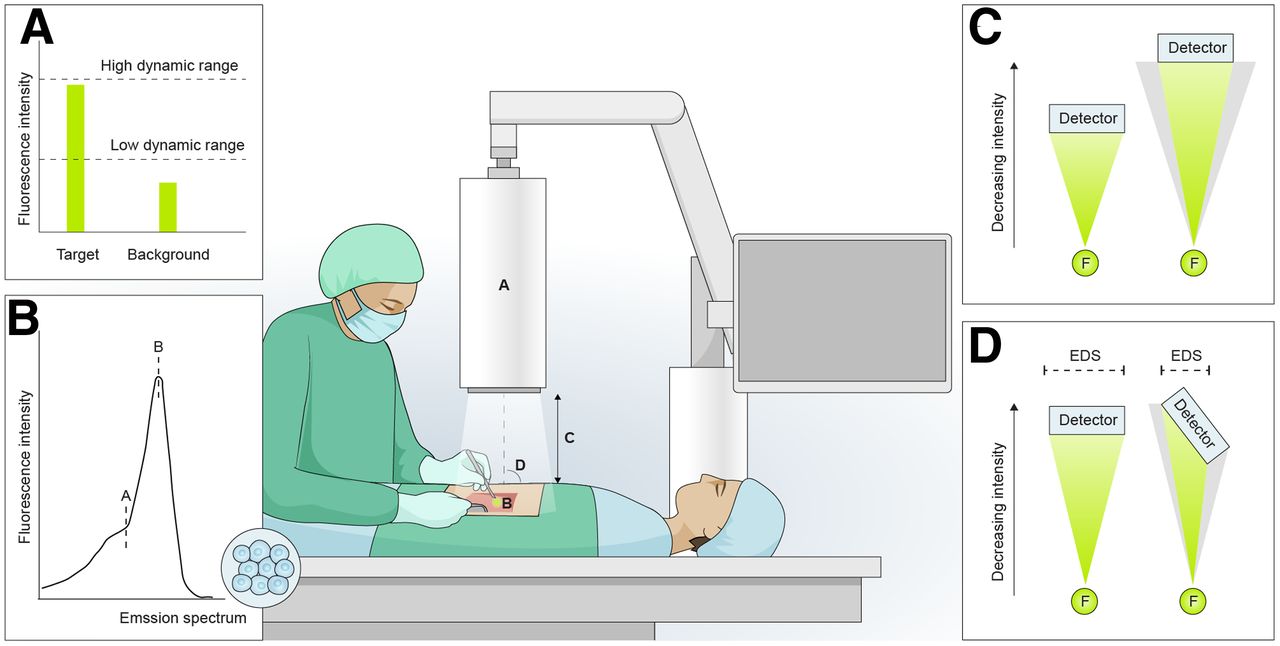
Potential pitfalls in FI studies. (A) CNR ratio is strongly dependent on dynamic range of FI camera system concerning fluorescent tracer. When imaging tissue using fluorescent tracer with high quantum yield, system with high dynamic range would result in higher CNR ratio than would system with low dynamic range. (B) Fluorescence intensity detected by FI camera system is dependent on match between system’s optical filter and emission peak of fluorescent tracer used. Mismatch between emission peak and optical filter will result in suboptimal fluorescence intensity detected (wavelength A) compared with most optimal (wavelength B). (C) Fluorescence intensity exponentially decreases with increased working distance because of diverging nature of light. (D) When detector is not placed perpendicular to tissue of interest, effective detection surface that can detect emitted photons is smaller. As such, fluorescence intensity is falsely reduced, possibly leading to erroneous conclusions. EDS = effective detection surface.
Depth sensitivity is the ability to measure fluorescent signal at a certain depth. This is largely dependent on the type of light (i.e., coherent or noncoherent) and the wavelength-specific penetration depth of the excitation light. Ideally, devices should evolve to account for this automatically, yet the user should be aware for each clinical application of interest (27). For margin assessment, the imaging depth may vary among different tumors, since the definition of an adequate margin is different. Head and neck cancer requires a tumor-free margin of at least 5 mm, whereas for breast cancer this is at least 1 mm. Although the penetration depth of light increases with longer wavelengths (i.e., near-infrared versus visible spectrum), this does automatically translate to increased measurement depth. When deeper tissues are imaged because of increased scattering, the discrimination between target and surrounding tissue is impaired because of a decreasing CNR with imaging depth (i.e., low depth sensitivity) (Fig. 2).
Field homogeneity describes how uniformly the region of interest is illuminated. Inhomogeneous field illumination can lead to over- or underestimation of the fluorescent signal throughout the field of view. Perfect field homogeneity is rarely achieved in practice, and only a few FI camera systems have implemented algorithms to improve field homogeneity. Most systems, especially endoscopic ones, have highly inhomogeneous light fields that lead to steep intensity fall-off toward the edge of the field. The user should validate the field homogeneity before every imaging procedure using a calibration phantom. An inhomogeneous field illumination is not an insurmountable problem, as long as the user is aware and knows how to interpret and correct for it (28).
The resolution of an FI camera system is characterized by spatial and temporal resolution. The spatial resolution dictates the modality’s ability to differentiate between the smallest fluorescent sources. The spatial resolution should at least be half the size of the smallest feature that has to be detected, as described by the Nyquist theorem. The temporal resolution dictates the modality’s ability to detect changes in signal over time. This ability is of importance when a dynamic phenomenon is of interest, such as organ perfusion (e.g., semiquantitative indocyanine green) (29).
The dynamic range greatly influences the ability to measure fluorescent signal. The dynamic range (i.e., the detector’s quantum efficacy) is the measure for the highest and lowest amount of measurable light for a set exposure time. A camera system with a low dynamic range can measure either very high or very low signals, depending on exposure time. However, the camera cannot do so both at the same time. Hence, a camera with a high dynamic range can measure both very bright (i.e., high quantum yield) and very dim (i.e., low quantum yield) fluorescent signals (Fig. 3A).
BENCHMARKING OF FLUORESCENCE IMAGING CAMERA SYSTEMS
To compare different FI camera systems, universal standards are required for benchmarking their performance, as is common in the other medical imaging modalities (30). As such, solid-tissue–mimicking phantoms have been developed to characterize the different FI imaging systems quantitatively. Wells filled with different concentrations of nanoparticles (i.e., quantum dots) are used to measure camera detection sensitivity versus optical properties, depth sensitivity, dynamic range, field homogeneity, and spatial resolution (28). We advise that users acquire an FI camera system with high camera detection sensitivity in combination with a high dynamic range. Also, the camera wavelength specificity and emission light sources should match the excitation and emission spectra of the fluorescent tracer (Fig. 3B) (27,31,32).
Performing phantom measurements before each imaging procedure informs on system stability over time and provides users better insight into the performance capabilities. A standardized image of an FI phantom should be taken under strict imaging acquisition parameters (i.e., camera distance, incidence angle, and ambient light) and processed according to a strict protocol (28,31,32). Automated log files should be constructed according to a standardized format and recorded for review purposes, safeguarding a quality management system for FI in clinical use. Ideally, these log files are archived with the patient data and imaging results, allowing for calibration in later analysis of batch data, similar to the metadata archived in DICOM images taken with radiologic imaging systems. We propose a quality management system to enable comparative multicenter clinical trials and implementation in general practice, enabling uniformity.
Additionally, FI camera systems should have the option to export raw data without interference from undesired image postprocessing to obtain quantitative or semiquantitative data rather than qualitative images. However, some commercial intraoperative imaging devices often opt for an underlay for the surgeon’s orientation purposes, which impedes the possibility of quantification (11).
FLUORESCENCE CONTRAST
Fluorescence contrast can be either endogenous (i.e., autofluorescence of intrinsic tissue compounds) or exogenous (i.e., administered fluorescent tracer) (33). Although the use of endogenous contrast has some advantages, such as inherent nontoxicity and absence of regulatory issues, we focus on the use of exogenous contrast as this has been shown to increase specificity and detection sensitivity (34). The main criteria for selecting a fluorescent tracer include efficient fluorescent light output (i.e., quantum yield), biodistribution and pharmacokinetic characteristics, signal enhancement strategies (i.e., “always-on” versus “activatable” or “smart”), and regulatory approval (12). Lastly, the clinician must be aware of regulatory issues that can result in tremendous costs when designing and using new fluorescent tracers, such as intellectual property, animal toxicology studies, availability of compounds in a good-manufacturing-practice facility. and regulatory approval (35,36).
Generally, exogenous fluorescent tracers can be divided into targeted and nontargeted tracers. Nontargeted tracers do not bind to biomarkers for disease specificity but accumulate passively into the tissue through metabolism or nonspecific uptake (e.g., enhanced permeability and retention effect in tumors). A well-known nontargeted fluorescent tracer is indocyanine green, which has Food and Drug Administration approval for tissue perfusion assessment, sentinel lymph node mapping, and biliary duct visualization. As fluorescent dyes themselves are not tumor-specific, efforts to improve specificity have led to the development of targeted fluorescent tracers that bind to receptors or biomarkers (37). Particularly in interventional oncology (e.g., surgery or gastroenterology), phase I studies have shown the potential of these tracers for margin assessment and characterization of lesions. Recently, breakthrough therapy designations have been assigned by the Food and Drug Administration (i.e., Pegloprastide [Avelas Biosciences], a ratiometric fluorescent probe for breast-conserving surgery) (15).
The clinical indication should be leading when one is deciding between a targeted and nontargeted approach. The targeted approach is generally more complex and thus not always preferred. A nontargeted tracer could suffice for sentinel lymph node mapping as such a tracer generates contrast between the lymph nodes and the adjacent tissue. Contrarily, tumor delineation requires a targeted tracer with higher tumor specificity. Even though targeted tracers are used, one should realize that the signal is not proportional to the concentration of the target but is confounded by nonspecific sources of contrast. This nonspecific accumulation of fluorescent tracer is intrinsically determined by its receptor affinity but is also affected by physiologic phenomena, such as vascularity, vascular permeability, interstitial pressure, and lymphatic drainage (38). Paired imaging methods are currently being studied to correct for the nonspecific tracer accumulation by coadministering an untargeted control agent with similar pharmacokinetics (39,40). A wide range of fluorescent tracers is currently being studied in clinical trials, including small molecules, peptides, proteins, and nanoparticles, as described elsewhere (37).
Current developments to improve fluorescent contrast include the use of activatable or smart fluorescent tracers that fluoresce only after interaction with or binding to the target (41,42). Rather than visualizing one fluorescent tracer in a single lesion, multispectral imaging (i.e., imaging fluorescent probes at different or multiple wavelengths) could simultaneously visualize multiple fluorescent tracers that report on different targets within the same patient. The advantages include the delivery of a more homogeneous signal, increased sensitivity, and the ability to obtain anatomic–molecular information (43). For example, one might strive to both perform molecular imaging of the tumor and identify critical structures (e.g., nerves), both contributing to an optimal surgical outcome and both requiring a specific tracer with different fluorescent excitation and emission wavelengths. Technical challenges include accurately separating signals and correcting for differences in fluorescent dyes (i.e., efficiency of fluorescent signal generation and wavelength-dependent tissue optical properties), as described elsewhere (44). The clinical introduction, safety, and applicability of multispectral FI remain to be investigated in clinical trials.
IMAGE ACQUISITION: REPRODUCIBILITY AND STANDARDIZATION
Reproducibility and standardization should be central within the 2 primary components of an FI study protocol: tracer administration and image acquisition. Similarly to PET, the tracer administration must be dosed and timed consistently throughout the entire study population (45). The exact dose is commonly determined using dose-escalation schemes, with pharmacokinetics, biodistribution, and toxicology studies in animals, healthy volunteers, or subjects belonging to the target population. Whether timing between tracer administration and image acquisition is crucial depends on the biodistribution and pharmacokinetic profile of the tracer. When studying a dynamic perfusion assessment (i.e., semiquantitative use of indocyanine green), the timing comes down to seconds. In such a setting, the administration can be standardized by using a syringe pump with a preprogrammed infusion rate. On the other hand, many targeted fluorescent tracers need substantial time (i.e., days) to bind to the target moiety and ensure clearance of unbound tracer from the blood.
The detected fluorescence is dependent on different specifications of the FI camera system (e.g., exposure time and gain) in combination with the contrast, as well as variable imaging parameters of the experiment itself (e.g., working distance, incident angle, and ambient light). Imaging with varying working distances substantially impacts the data consistency since the intensity measured is distance-dependent (Fig. 3C). Consequently, higher fluorescence intensity is detected when the distance from the tissue of interest to the detector decreases, even when the fluorescent light emitted is the same. The camera should be perpendicular to the tissue to maximize the effective surface area of the detector (Fig. 3D). When all variable imaging parameters are standardized in every FI measurement, the imaging data allow for reproduction and represent the tracer distribution more realistically (27). Ideally, all imaging parameters should also be registered to allow for post hoc correction.
Although the impact of ambient light in FI has never been underestimated (46), it is rarely standardized or corrected for. The most common solution is to keep the ambient light to a constant minimum, as relatively few systems can deal with high ambient-light intensity. The choice of lighting in the operating room can be optimized, typically by minimizing near-infrared light. This is specifically emitted from commonly used tungsten bulbs, which could simply be replaced by light-emitting diodes. Needless to say, this solution reduces the problem only for near-infrared-based emission probes such as indocyanine green.
REPORTING ON FI DATA
Apart from a standardized imaging protocol, standardized data processing, representation, and reporting are necessary for the implementation of FI in the standard of care. Contrary to some other imaging techniques (e.g., CT), wide-field FI does not provide quantitative data. Even when imaging parameters are standardized, variations in tissue optical properties affect the fluorescent signal. Additionally, the signal is heavily surface-weighted, meaning that anything closer to the surface will generate more fluorescent signal. These factors need to be taken into account when analyzing FI data. The most used semiquantitative unit is mean fluorescence intensity, defined as the average pixel intensity within a region of interest. Yet, reporting the mean fluorescence intensity as an absolute and quantitative measure without a thoroughly standardized protocol can lead to incorrect conclusions.
Since FI is a detection or discrimination method, relative measures (i.e., ratios) are more appropriate for FI as these demonstrate the ratio between the target and the background. Commonly used ratios in clinical FI include tumor-to-background ratio, signal-to-background ratio, and CNR (47). We advocate the use of CNR, defined as the target’s mean fluorescence intensity subtracted by the background’s mean fluorescence intensity, divided by the SD of the background. Using a CNR is favorable since this is more informative on the detectability of the contrast (i.e., target) of interest (48). A high CNR indicates good discrimination between the target and background tissue. Still, the CNR is influenced by the FI camera system’s dynamic range and quantum efficiency. For example, using a fluorescent tracer with a relatively high quantum yield together with 2 different FI camera systems with a low and high dynamic range may result in 2 very different CNRs. In other words, an FI camera system with a low dynamic range may underestimate the CNR because the signal of the tumor is limited (Fig. 3A). Also, despite the seemingly straightforward definition, these quantities are prone to bias due to the strong dependency on the definition of the surrounding tissue. Ideally, the target and the background are based on the gold standard (i.e., histopathology). The appropriate background must be adjacent tissue, as it mimics the clinical scenario.
Clinical use of FI relies on the interpretation of data that are typically shown as an image or video, even though the ratios are most important in clinical trials. Fluorescence images should be uniformly reported across the field to avoid difference in image interpretation. This reporting includes the choice of color map, functions for the lookup table, and image compression. Perceptually uniform science-derived color maps represent actual data variations, reduce complexity, and are accessible for color-deficient people (49). Yet, even when data are uniformly reported, the interpretation of FI signal without correction for tissue optical properties may lead to inaccurate conclusions. Lack of correction may, for example, lead to erroneous tumor delineation (due to scattering) in margin assessment when interpreted by different clinicians, Lastly, the used FI camera system settings must be described in detail. Reporting these settings is essential for the reproducibility of study results, as the FI camera system settings severely influence the obtained FI data.
CONCLUSION
The rapidly increasing interest in FI has led to serious improvements in the FI camera systems and fluorescent tracers available. Although FI has shown enormous potential for a variety of indications, the field has not yet established clinical implementation. Here, we have provided a guideline for clinicians to perform FI clinical trials (Fig. 1). The same conceptual thinking applies to other optical imaging modalities, such as laser speckle contrast imaging or spectroscopy-based techniques. Similar to the classic medical imaging field, the FI field should focus on training clinicians and supportive staff in a multidisciplinary way to better understand the underlying physics and chemistry. Still, we advise clinicians to collaborate with researchers who have experience with FI camera systems and fluorescent tracers in order to correctly acquire, analyze, and interpret the imaging data in an accurate and reproducible manner. To establish the clinical implementation of FI, phase II and III trials need to commence using a consistent study design, imaging protocol, and data analysis. By emphasizing standardization and reproducibility, we can realize the full potential of FI and prove its clinical value.
DISCLOSURE
Vasilis Ntziachristos is an equity owner and consultant of iThera Medical GmbH, an owner of Spear UG, and a member of the Scientific Advisory Board of SurgVision B.V./Bracco Sp.A. Gooitzen M. van Dam is the chief executive officer and a founder and shareholder of TRACER Europe B.V./AxelaRx. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Feb. 10, 2022.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
Immediate Open Access: Creative Commons Attribution 4.0 International License (CC BY) allows users to share and adapt with attribution, excluding materials credited to previous publications. License: https://creativecommons.org/licenses/by/4.0/. Details: http://jnm.snmjournals.org/site/misc/permission.xhtml.
REFERENCES
- Received for publication July 28, 2021.
- Revision received January 14, 2022.
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- DEFINING THE CLINICAL INDICATION AND IDENTIFYING THE APPROPRIATE TARGET
- SELECTION OF THE APPROPRIATE IMAGING MODALITY
- BENCHMARKING OF FLUORESCENCE IMAGING CAMERA SYSTEMS
- FLUORESCENCE CONTRAST
- IMAGE ACQUISITION: REPRODUCIBILITY AND STANDARDIZATION
- REPORTING ON FI DATA
- CONCLUSION
- DISCLOSURE
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.