


Abstract
It is unknown whether assessment of potential bone lesions in metastatic breast cancer (MBC) by 18F-FDG PET instead of 99mTc bone scintigraphy (BS) supports clinically relevant changes in MBC management. Therefore, we retrospectively compared management recommendations based on bone lesion assessment by 18F-FDG PET plus contrast-enhanced CT (ceCT) or BS plus ceCT, for patients with newly diagnosed MBC. Methods: Baseline ceCT, BS, and 18F-FDG PET for all patients included in the IMPACT-MBC study (NCT01957332) at the University Medical Center Groningen were reviewed for bone lesions. If bone lesions were found by any imaging modality, virtual MBC management recommendations were made by a multidisciplinary expert panel, based on either 18F-FDG PET plus ceCT or BS plus ceCT. The panel had access to standard clinicopathologic information and baseline imaging findings outside the skeleton. Clinically relevant management differences between the 2 recommendations were defined either as different treatment intent (curative, noncurative, or unable to determine) or as different systemic or local treatment. If no bone lesions were found by any imaging modality, the patients were included in the analyses without expert review. Results: In total, 3,473 unequivocal bone lesions were identified in 102 evaluated patients (39% by ceCT, 26% by BS, and 87% by 18F-FDG PET). Additional bone lesions on 18F-FDG PET plus ceCT compared with BS plus ceCT led to change in MBC management recommendations in 16% of patients (95% CI, 10%–24%). BS also changed management compared with 18F-FDG PET in 1 patient (1%; 95% CI, 0%–5%). In 26% (95% CI, 19%–36%) of patients, an additional 18F-FDG PET exam was requested, because BS provided insufficient information. Conclusion: In this exploratory analysis of newly diagnosed MBC patients, 18F-FDG PET versus BS to assess bone lesions resulted in clinically relevant management differences in 16% of patients. BS delivered insufficient information in over one fourth of patients, resulting in an additional request for 18F-FDG PET. On the basis of these data, 18F-FDG PET should be considered a primary imaging modality for assessment of bone lesions in newly diagnosed MBC.
Breast cancer is the most common malignancy among women worldwide, with the second highest rate of cancer-related deaths in both developing and developed countries (1). At a median of 6 y after surgery for primary breast cancer, about 15% of patients develop distant metastases. The annual hazard of recurrence peaks in the second year after diagnosis, but the annual risk remains 2%–5% in years 5–20 (2). In half the patients with a history of breast cancer who develop metastases, the first relapse occurs in the bone (3). Diagnostic imaging assessments are required to evaluate the presence of bone lesions. Standard staging frequently is performed by means of contrast-enhanced CT (ceCT), but this is not considered an optimal imaging modality for detecting bone lesions. CT is especially helpful for characterizing sclerotic bone lesions and lesions with mineralized matrix (4). Currently, European Society of Medical Oncology guidelines do not specify which type of assessment is preferred for the evaluation of bone lesions (5). National Comprehensive Cancer Network guidelines advise either 99mTc-diphosphonate whole-body bone scintigraphy (BS) or 18F-NaF PET and consider 18F-FDG PET an optional modality in addition to standard imaging (6). For this reason, the CT is commonly complemented with planar BS (without technical refinement with SPECT/CT). This imaging technique, however, visualizes only osteoblastic activity; therefore, osteolytic metastases can be missed, especially when growing rapidly, when bone turnover is slow, or when the site is avascular. False-positive findings can occur in cases of inflammation or trauma (7,8). 18F-FDG PET visualizes glucose uptake reflecting metabolically active tissue and is therefore capable of imaging a broad spectrum of malignancies, including both osteoblastic and osteolytic bone lesions. The clinical relevance of the ability of 18F-FDG PET to visualize more bone lesions is unclear. Many studies have compared BS and 18F-FDG PET, but head-to-head comparisons of clinical relevance are lacking (9–17).
It has been established that 18F-FDG PET changes management for patients with primary breast cancer at stages IIA–IIIC (18). We retrospectively compared management recommendations based on bone assessment by 18F-FDG PET plus ceCT, versus BS plus ceCT, for patients with newly diagnosed metastatic breast cancer (MBC).
MATERIALS AND METHODS
Patients
Patients with a first presentation of non–rapidly progressive MBC were enrolled in the multicenter IMPACT-MBC study (Imaging Patients for Cancer Drug Selection—Metastatic Breast Cancer) (NCT01957332) between August 2013 and November 2017. All patients provided written informed consent for enrollment in the IMPACT-MBC study, which was approved by the Medical Ethical Committee of the University Medical Center Groningen and the Central Committee on Research Involving Human Subjects. Within IMPACT-MBC, patients underwent extensive diagnostic assessment at baseline, including biopsy of a metastasis (the biopsy site was dictated by safety assessments) ceCT, BS, and 18F-FDG PET, before treatment initiation (19). For the present exploratory, retrospective analysis, baseline ceCT, BS, 18F-FDG PET, and standard clinicopathologic data were used of all patients enrolled in IMPACT-MBC at the University Medical Center Groningen. Patients did not undergo extra bone biopsies to confirm metastatic bone lesions if imaging modalities were discordant. Actual treatment decisions and patient outcome are not included in the present analysis. According to Dutch law, for the current retrospective data analysis without medical intervention, no additional consent was required.
Patient Imaging
Contrast-enhanced full-dose CT from the neck to the pelvis was performed with oral and intravenous contrast material and a slice thickness of 2 mm for the body and 1 mm for the neck on a multislice Somatom Definition CT scanner (at least a 64-slice scanner; Siemens/CTI). Planar whole-body BS was performed 2.5–4 h after intravenous injection of 500 ± 10% MBq of 99mTc-diphosphonate on a double-head γ-camera (a Symbia S, a T2, or a T16; all Siemens/CTI) equipped with a low-energy, high-resolution collimator. 18F-FDG PET/CT was performed 1 h after the intravenous administration of a 3 MBq/kg dose of 18F-FDG from the head to the upper thigh at 1–3 min per bed position on a Biograph mCT PET/CT system (either a 40- or a 64-slice CT scanner) (Siemens/CTI), accredited by European Association of Nuclear Medicine Research Limited. Scan acquisition and reconstructions were performed following the recommendations of the European Association of Nuclear Medicine guideline for oncologic 18F-FDG PET/CT imaging (20). Before the PET acquisition, the patients underwent a low-dose CT scan during tidal breathing for attenuation correction (80–140 kVp; quality reference, 30 mAs; pitch, 1).
Assessment of Bone Lesions
CeCT and 18F-FDG PET were performed within 28 d before treatment initiation, and BS was within 50 d, according to the protocol. Two dedicated musculoskeletal radiologists and 2 dedicated nuclear medicine physicians reported all unequivocal metastatic bone lesions and equivocal findings (bone lesions that could not be merely dismissed as benign) on ceCT, BS, and 18F-FDG PET, masked to the other scans. Each scan was assessed by 1 physician. Window levelling to the bone setting was used to assess the ceCT scans in axial, coronal, and sagittal planes, and the low-dose CT accompanying 18F-FDG PET was not evaluated separately for bone lesions. A maximum of 1 lesion per vertebra was included in the database. For all other bone structures, the physicians were asked to count and report every single lesion.
MBC Management Recommendations by Expert Panel
The expert panel consisted of 3 medical oncologists and 2 radiation oncologists with broad experience in MBC management. Patient data were anonymized, mixed, and discussed twice during 10 expert panel meetings between June 2017 and March 2018. The dedicated radiologists and nuclear medicine physicians informed the expert panel about unequivocal and possible bone lesions on either 18F-FDG PET plus ceCT or BS plus ceCT, either in person (in complex cases) or through their reports (in clear cases). The expert panel provided MBC management recommendations for 2 scenarios: bone lesion assessment by 18F-FDG PET plus ceCT or by BS plus ceCT. To isolate the clinical relevance of the difference in bone lesion detection ability of BS and 18F-FDG PET, the 2 scenarios differed solely in information on bone lesions, either bone lesions detected by BS or bone lesions detected by 18F-FDG PET. All other information needed to compose management recommendations was equal between the 2 scenarios and consisted of standard clinicopathologic information, including age, tumor receptor status of the primary tumor and metastasis, patient performance status and complaints, relapse time, visceral involvement on both ceCT and 18F-FDG PET, and standard biochemistry results. Information on actual administered treatment and patient outcome was not provided to the expert panel. Patients without bone lesions on any of the imaging modalities were included in the total study population but not discussed by the expert panel. For these patients, it was assumed that management recommendations would be concordant between the scenarios with 18F-FDG PET plus ceCT and BS plus ceCT and that there would be no requests for additional imaging to evaluate bone lesions.
The expert panel reviewed either 18F-FDG PET plus ceCT or BS plus ceCT by reading the reports of the unequivocal and possible bone lesions as established by—and, if applicable, receiving further elucidation from—the dedicated radiologists and nuclear physicians and viewing the maximum-intensity projections of the BS or 18F-FDG PET or all images if requested. On the basis of these 2 scenarios, and standard clinicopathologic information, the expert panel gave separate MBC management recommendations for treatment intent, systemic and local therapy, and the need for additional imaging. Clinically relevant management differences between the 2 scenarios were defined as different treatment intent (curative vs. noncurative or unable to determine) or different systemic or local therapy.
Statistical Analysis
Descriptive statistics were used for bone lesion detection rates on ceCT, BS, and 18F-FDG PET separately. Only unequivocal metastatic bone lesions were used to calculate detection rates. Multilevel κ-coefficients were used to describe lesion detection agreement among the 3 modalities (21). Differences between MBC management recommendations of the expert panel were described as the percentage of patients for which the management recommendation based on 18F-FDG PET plus ceCT and BS plus ceCT differed, accompanied by 95% CIs. Whether routine clinical characteristics (histology, receptor status, Elston tumor grade of primary tumor, clinical suspicion of bone lesions, time to recurrence, and number of bone lesions on ceCT) could potentially predict lack of added value of 18F-FDG PET was explored with both uni- and multivariable regression (the latter by the least absolute shrinkage and selection operator (22)), using the area under the under the receiver-operating-characteristic curve to evaluate discriminative ability. A P value of 0.05 or less was considered significant.
Costs were calculated using Dutch national prices for the scans, as established by the Dutch Healthcare Authority (23). Other costs, such as travel expenses, were not considered.
RESULTS
Patients
Between August 2013 and November 2017, 116 female MBC patients were enrolled in the IMPACT-MBC study at the University Medical Center Groningen (Fig. 1: Consolidated-Standards-of-Reporting-Trials diagram). Ten patients were excluded from the study and thus from the current analysis because of violation of entry criteria (n = 9) or withdrawal of consent (n = 1). Four other patients were excluded from the current analysis for an analysis-related protocol violation (50 or more days between the baseline scans; n = 3) or nonevaluable 18F-FDG PET images (n = 1) due to diffuse malignant uptake consistent with extensive bone involvement for which it was not possible to count separate lesions. The remaining 102 MBC patients were included in this analysis. In 97 patients, histologic proof of MBC was available. Fifty-seven of 97 biopsies (56%) were obtained from bone lesions. In the remaining 5 patients, 2 had a cytologic biopsy proving MBC, 2 had no tumor cells in the biopsy sample, and 1 patient refused a biopsy. For these 3 patients without pathologic proof, the diagnosis of MBC was based on imaging and laboratory findings. For all 102 patients, baseline ceCT, BS, and 18F-FDG PET scans were evaluated for the presence of bone lesions. In 93 of 102 patients, equivocal or unequivocal bone lesions were found on ceCT, BS, or 18F-FDG PET, and 9 patients had only extraosseous metastases. The median time frame in which all 3 scans were performed was 12 d (range, 0–49 d). Table 1 shows the patient characteristics.
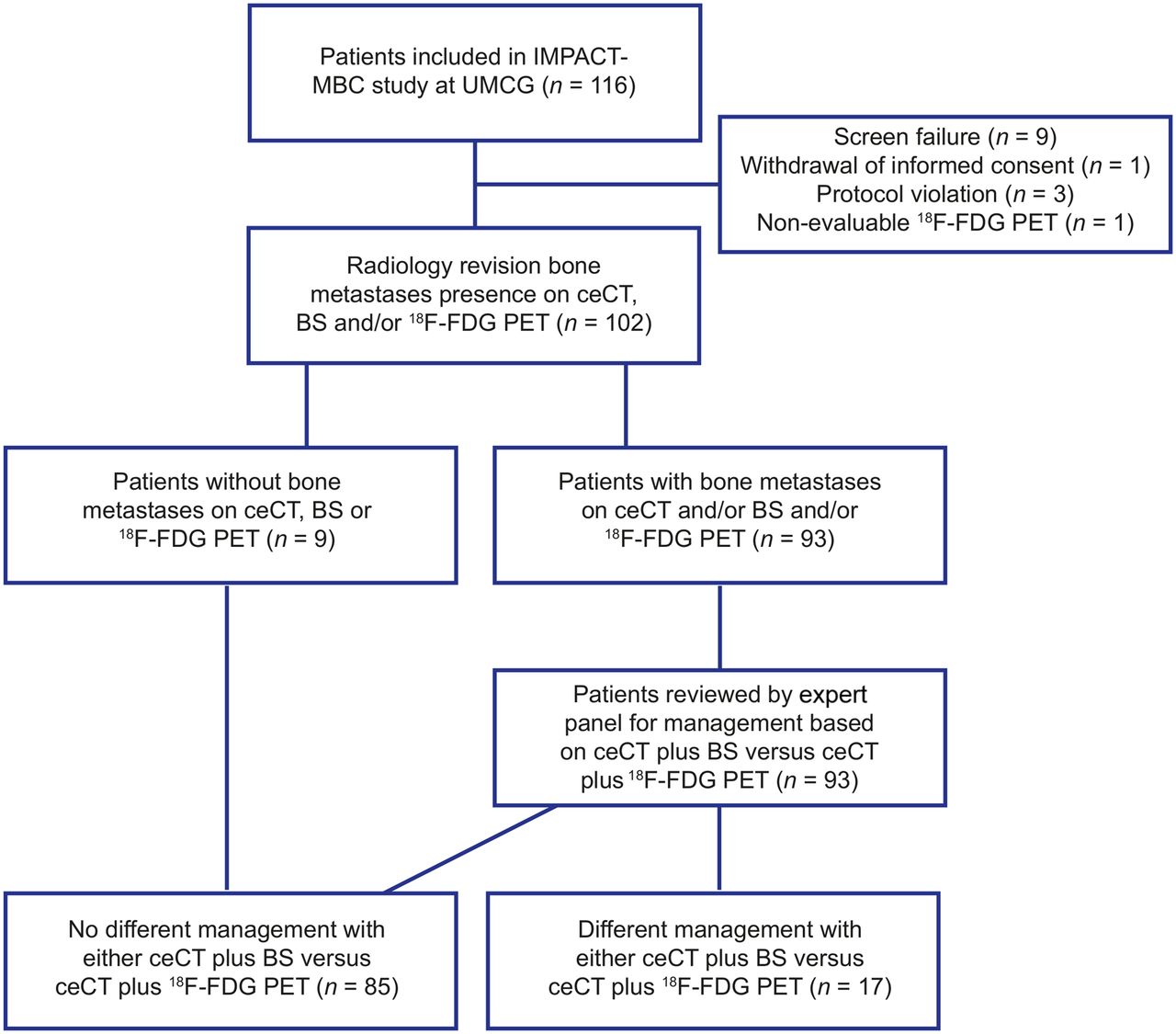
Flow chart visualizing selection of patients and how they are analyzed. UMCG = University Medical Center Groningen; CAD = calcium, vitamin D.
Patient Characteristics
Detection of Bone Lesions
In 9 of 93 MBC patients with bone lesions, only equivocal bone lesions were observed on ceCT, BS, or 18F-FDG PET. In total, 3,473 unequivocal bone lesions were identified in 84 patients (median per patient, 27; 25th–75th percentiles, 3–58). Of these lesions, 1,004 (39.3%) were on ceCT, 655 (26.3%) on BS, and 2,285 (87.4%) on 18F-FDG PET (18F-FDG PET vs. CT, P < 0.0001; 18F-FDG PET vs. BS, P < 0.0001; CT vs. BS, P < 0.0001). The agreement between imaging modalities in identifying patients with and without unequivocal bone lesions was weak to moderate, whereas there was poor agreement at the lesion level (Supplemental Fig. 1 and Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org). On average, 18F-FDG PET detected 20 more bone lesions per patient than BS (95% CI, 14–27; P < 0.0001) and 16 more lesions than ceCT (95% CI, 10–22; P < 0.0001). ceCT detected on average 4 more bone lesions than BS (95% CI, 1–8; P = 0.022). Nine patients had bone lesions only on 18F-FDG PET, 1 patient only on BS, and none only on ceCT.
Bone Lesion Detection by ceCT Alone
ceCT visualized 1,004 bone lesions, of which 299 (29.8%) were not visible on either BS or 18F-FDG PET. The 299 bone lesions that were visualized only by ceCT were in 33 patients (median of 3 per patient, range of 1–77). In 6 of 102 patients, ceCT alone detected more bone lesions than BS alone or 18F-FDG PET alone; these patients all had extensive disease with palliative treatment intent.
Differences in MBC Management Recommendations by Expert Panel When Based on Bone Lesions Detected by BS Plus ceCT and 18F-FDG PET Plus ceCT
In 16 of 102 patients (16%; 95% CI, 10%–24%), MBC management recommendations differed because of additional bone lesions on 18F-FDG PET plus ceCT compared with BS plus ceCT. More systemic treatment was recommended, and either curative radiotherapy was canceled or palliative radiotherapy added. In 9 patients, treatment intent was changed. Furthermore, in 6 patients there was a new indication for bisphosphonate and calcium plus vitamin D, and for 1 patient palliative radiotherapy was recommended because of the additional findings on 18F-FDG PET.
BS also changed management compared with 18F-FDG PET in 1 patient (1%; 95% CI, 0%–5%). These management differences are shown in Figure 2 and described in Table 2. Figure 3 shows the images of one of these patients as example.
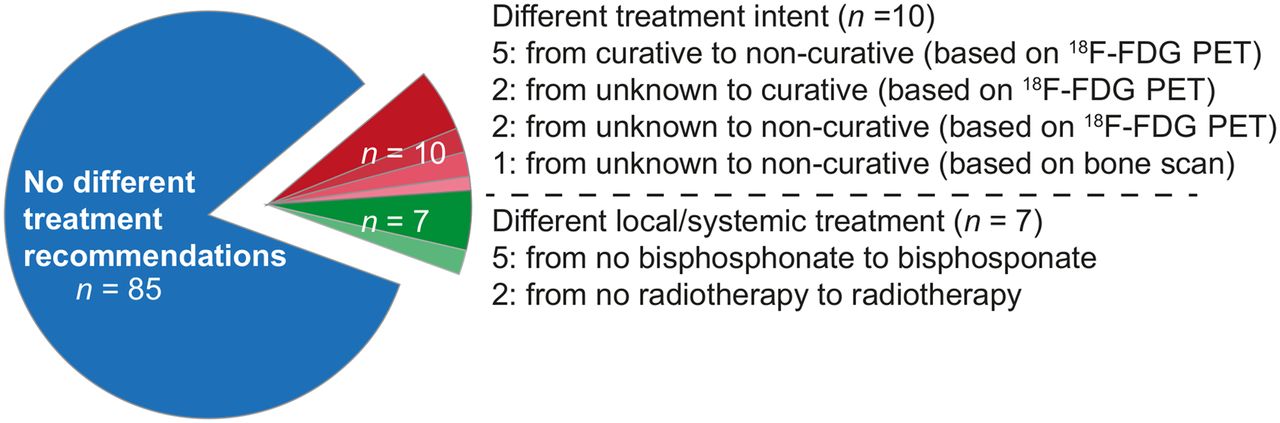
Pie chart visualizing number of patients with clinically relevant difference in management recommendations after 18F-FDG PET plus ceCT (n = 16) and BS plus ceCT (n = 1).
Concordance of Management Recommendations by Expert Panel Based on Evaluation of Bone Lesions on BS Plus ceCT or 18F-FDG PET Plus ceCT

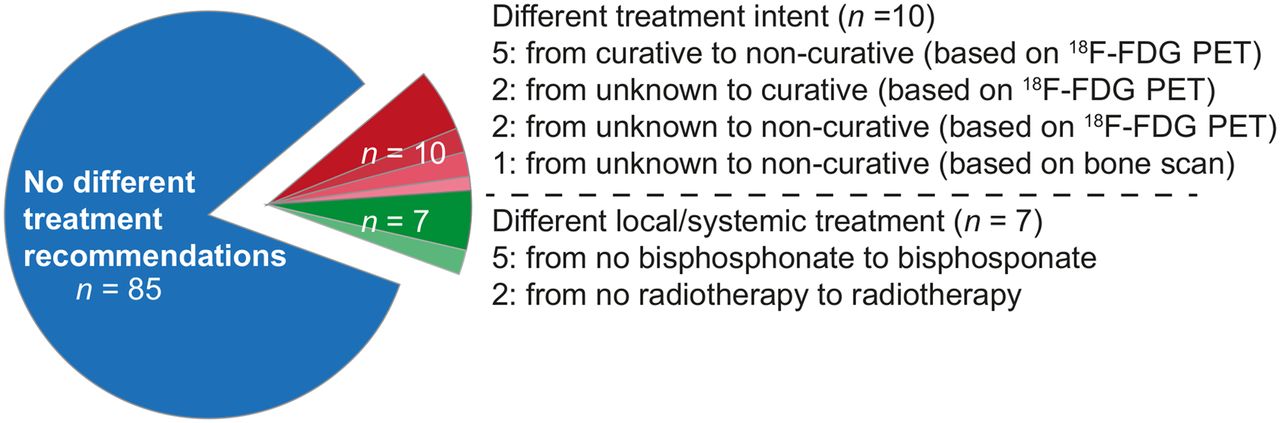
Example patient with clinically relevant difference in management recommendation after 18F-FDG PET plus ceCT compared with BS plus ceCT (patient 14 of Table 3). (A) ceCT visualized 1 bone metastasis in T5 (transversal section of ceCT through T5) and 3 equivocal lesions in iliac bone (1 on left, 2 on right). (B) BS visualized no bone lesions. (C) Maximum-intensity-projection 18F-FDG PET visualized 13 bone lesions (C) (C3, C5, T5, L3, L4, sacral bone [2], left acetabulum, right costa 7, left costa 5 [2], right humerus, and sternal bone). No equivocal lesions on ceCT were detected as metastases on 18F-FDG PET.
Individual patient management differences are shown in Supplemental Table 2. According to the expert panel, BS plus ceCT provided insufficient information to evaluate bone lesions in 27 cases, and additional 18F-FDG PET was requested (Table 2). For all included patients, this means that BS plus ceCT was insufficient in 26% (95% CI, 19%–36%) of cases. In 1 patient, 18F-FDG PET plus ceCT provided insufficient information to evaluate bone lesions according to the expert panel, and an additional BS was requested.
Added Value of 18F-FDG PET in Breast Cancer Subgroups Based on Standard Clinicopathologic Parameters
The 9 patients for whom 18F-FDG PET plus ceCT led to a change in treatment intent had rather limited metastatic disease; 5 had bone-only disease, 3 also had lymph node metastases, and 1 had both lymph node involvement and pleuritis carcinomatosa besides bone lesions. Five of the 7 patients for whom local or systemic treatment recommendations were expanded after 18F-FDG PET plus ceCT compared with BS plus ceCT had extensive metastatic disease with visceral involvement.
18F-FDG PET plus ceCT resulted most often in a different MBC management recommendation in patients with hormone receptor–negative primary breast cancer (5/17 patients, 29%; 95% CI, 13%–53%), compared with hormone receptor–positive disease (11/85 patients, 13%; 95% CI, 7%–22%). A higher number of bone lesions on ceCT was associated with a lower chance of added clinical value of 18F-FDG PET (area under the receiver-operating-characteristic curve, 0.68; 95% CI, 0.58–0.79) (Table 3). The patients who showed a clinically relevant management difference between 18F-FDG PET plus ceCT and BS plus ceCT had a maximum of 13 bone lesions on ceCT.
Predictors of Clinically Relevant Change in Management Recommendations After Evaluation of Bone Lesions by 18F-FDG PET Plus ceCT Instead of BS Plus ceCT
A multivariable prediction model based on all candidate routine clinical characteristics did not show a promising increase in discriminatory ability between patients with and without added clinical value from 18F-FDG PET, compared with the number of bone lesions on ceCT alone (optimism-corrected area under the receiver-operating-characteristic curve, 0.70; 95% CI, 0.59–0.81).
Cost Analysis
The costs of an 18F-FDG PET examination were €1,359 ($1,614), versus 570 ($677) for BS (at the time of the IMPACT-MBC trial). However, with the additional 18F-FDG PET after BS for 27 patients, the mean cost per patient would have been €929 ($1,103) when performing BS (apart from additional use of hospital resources and patient burden due to 2 separate scan appointments).
DISCUSSION
In this study, we showed that baseline 18F-FDG PET instead of BS would have had a clinically relevant impact on MBC management in 16 patients (16%), mostly resulting in more palliative treatment. In 7 of 16, the treatment intent switched from either curative or unable to determine to palliative; systemic or local management recommendations changed accordingly. This study also showed that in 26% of the patients an additional 18F-FDG PET examination would have been performed to assess bone metastases because BS was considered to deliver insufficient information.
This was the first study to assess clinically relevant management differences based on evaluation of bone lesions on 18F-FDG PET or BS in patients with newly diagnosed, non–rapidly progressive MBC. The strength of the present analysis is that we studied a representative group of patients with newly diagnosed, non–rapidly progressive MBC of all subtypes, with standardized imaging procedures and all scans performed shortly before the start of first-line therapy. In all patients but 5, MBC was pathologically proven by means of a histologic biopsy, mostly from a bone metastasis.
Nine of 102 MBC patients only had extraosseous disease; all 3 imaging modalities showed no sign of bone lesions. This finding is a clear reflection of BC at the first presentation of metastatic disease. At the start of staging procedures, the absence or presence of bone metastases is unknown. The clinical impact of choice of a particular staging procedure would have an influence on all patients, not just those who later demonstrate bone metastases; therefore, we have included all 102 patients in this analysis.
Several studies compared 18F-FDG PET with BS. In the literature, sensitivity and specificity were 88.3%–100% and 83.8%–99.4%, respectively, for 18F-FDG PET and 81%–98% and 71%–100%, respectively, for BS (9–14). The positive predictive value was 91.7%–100% and the negative predictive value 77.8%–100% for 18F-FDG PET, whereas the respective values for BS were 86.6%–90% and 80.8%–90% (9,12). One study concluded that BS is superior to 18F-FDG PET in determining BC bone lesions (9). Other studies showed that no BS is required in cases of bone metastases on 18F-FDG PET (15), as more bone metastases are seen on 18F-FDG PET than on BS (16,17); that when 18F-FDG PET shows no bone involvement, neither does BS with or without SPECT/CT (18); and that BS results in significantly more misclassifications than 18F-FDG PET (24). One study evaluated the influence of estrogen receptor expression. Better agreement between 18F-FDG PET and BS was seen for estrogen receptor–positive disease than for estrogen receptor–negative disease (16). All but one of these studies suggest better bone lesion detection with 18F-FDG PET than with BS; however, no firm conclusions can be drawn, as they were performed retrospectively, without a consistent comparison of imaging modalities and without pathologic confirmation. Furthermore, the impact on clinical decision making remained unknown. We confirmed a higher detection rate for 18F-FDG PET than for BS in this current study. Furthermore, we found that 18F-FDG PET was more likely to reveal additional findings leading to a clinically relevant change-in-management recommendation in hormone receptor–negative patients, as is in line with previous work (16).
We focused on bone lesions, but 18F-FDG PET can also visualize distant metastases in other organs; therefore, one might speculate that 18F-FDG PET may have an overall additional value in an even higher percentage of patients. For this analysis, 18F-FDG PET information on visceral involvement or other nonbone disease was presented to the expert panel both when making management recommendations based on BS plus ceCT and when making management recommendations based on 18F-FDG PET plus ceCT. Changes seen on serial 18F-FDG PET furthermore could be an interesting marker for time to progression and time to skeleton-related events in patients with bone-dominant MBC (25).
Interestingly, we demonstrated that a thorough revision of the CT by dedicated radiologists yielded more bone lesions than the BS (1,004 vs. 655). Because bone lesions detected on ceCT were presented to the expert panel together with BS and 18F-FDG PET, this also resulted in abatement of the difference between BS and 18F-FDG PET. This finding supports the need for imaging expertise in this challenging field of bone lesions. In addition, detailed assessment of all bone lesions in MBC at baseline might aid treatment decisions later in the course of the disease, such as if new bone pains arise. One could argue that ceCT for MBC staging is potentially enough for bone lesions also. However, in our analysis such was not the case, as bone-only disease could not be found just by ceCT. In view of the frequent occurrence of bone-only disease, particularly in newly diagnosed MBC, additional assessment of bone metastases, besides just on ceCT, obviously remains warranted. We found that in 26% of the patients in our cohort, additional 18F-FDG PET would be required besides BS and ceCT. This addition would have resulted in higher costs, although the overall costs for all patients would still have been lower with the BS–versus–18F-FDG PET strategy in this analysis. However, patient and hospital burden is smaller for 18F-FDG PET plus ceCT because they can be combined. Therefore, even apart from the MBC management implications, performing 18F-FDG PET is a patient-friendly alternative to BS for initial assessment of bone lesions in newly diagnosed MBC.
This study had limitations. First, 18F-NaF PET, now regularly used for bone lesion detection in staging of MBC, was not considered standard practice in The Netherlands at the time this study was conducted. A recent study showed that simultaneous PET/MRI with combined 18F-NaF and 18F-FDG showed more bone lesions than BS (26). However, 18F-NaF PET has false-positive results (27), and findings are not yet confirmed with biopsies in breast cancer. Furthermore, because application of BS remains widespread, this analysis remains of clinical relevance for daily practice. Second, the IMPACT-MBC study included patients with non–rapidly progressive MBC, because of the extra time that was needed for additional imaging at baseline. Thus, translation of our findings onto all MBC patients is limited. However, in some of the patients with rapidly progressive MBC, such as those with a visceral crisis who could not wait 2 extra weeks for initiation of chemotherapy, more or fewer bone lesions would likely not be of clinical relevance. Lastly, we did not investigate whether the adopted treatment plans after 18F-FDG PET led to better patient outcomes such as disease-free survival, overall survival, or quality of life, because patients were not treated according to the hypothetical regimens composed by the expert panel; their treatment was initiated according to all available diagnostics and information.
CONCLUSION
This study shows that 18F-FDG PET plus ceCT for assessment of bone lesions in newly metastatic MBC has a clinically relevant impact on disease management compared with a standard BS plus ceCT. Performing 18F-FDG PET upfront may reduce patient and hospital burden. Therefore, 18F-FDG PET should be considered a standard method of imaging assessment for bone lesions in newly diagnosed MBC.
DISCLOSURE
This work was supported by the Dutch Cancer Society, grant 2012-5565. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What is the clinical relevance of additional bone lesions on 18F-FDG PET compared with BS in patients with a first presentation of MBC?
PERTINENT FINDINGS: In this retrospective analysis, we found that in 16% of patients bone lesion assessment with 18F-FDG PET plus ceCT led to clinically relevant management differences compared with bone lesion assessment with BS plus ceCT. Furthermore, BS plus ceCT provided insufficient information in 26% of patients.
IMPLICATIONS FOR PATIENT CARE: 18F-FDG PET should be considered a primary imaging modality for assessment of bone lesions on suspicion of MBC.
Footnotes
Published online Aug. 17, 2020.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication March 6, 2020.
- Accepted for publication May 7, 2020.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.