


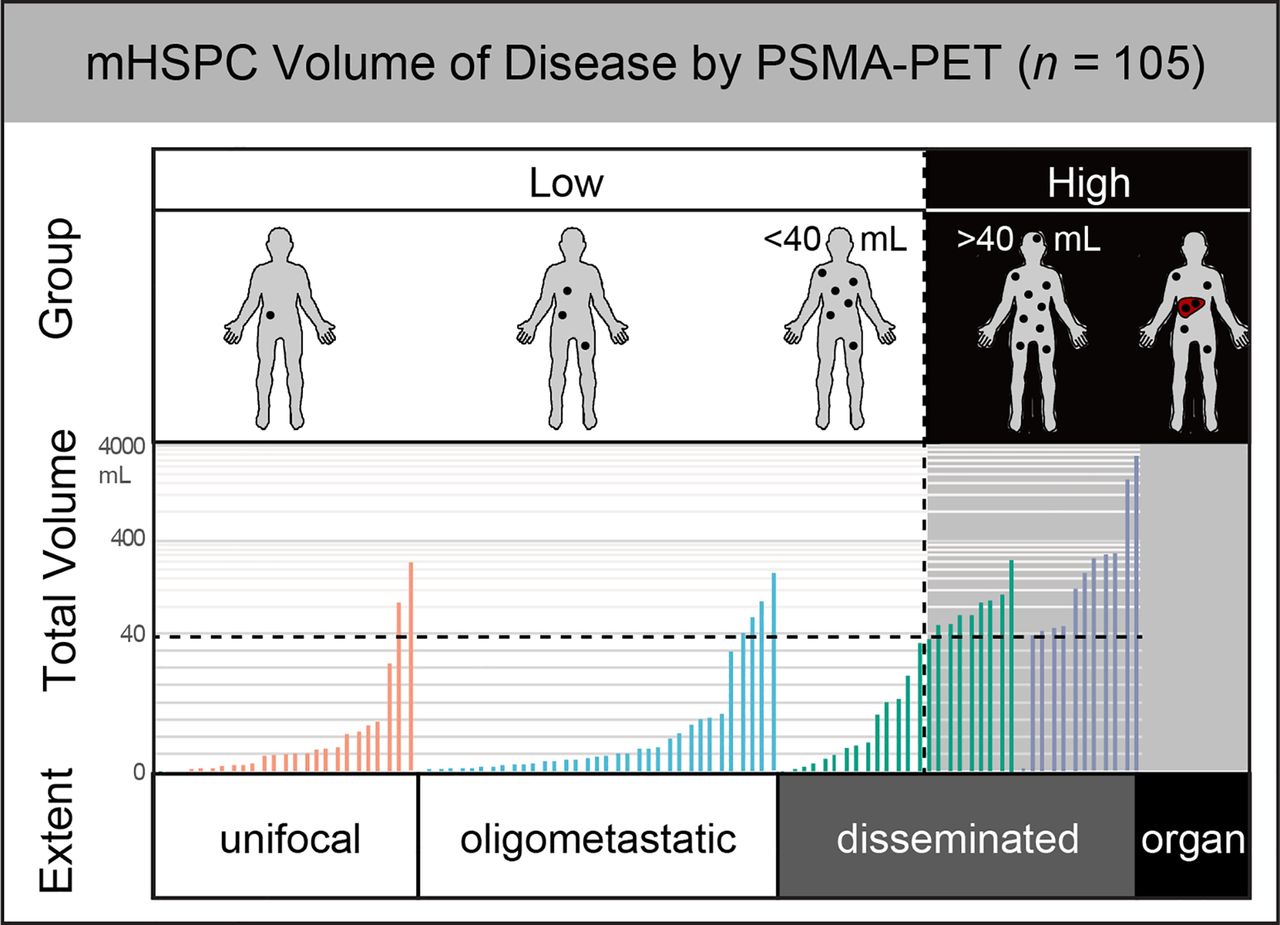
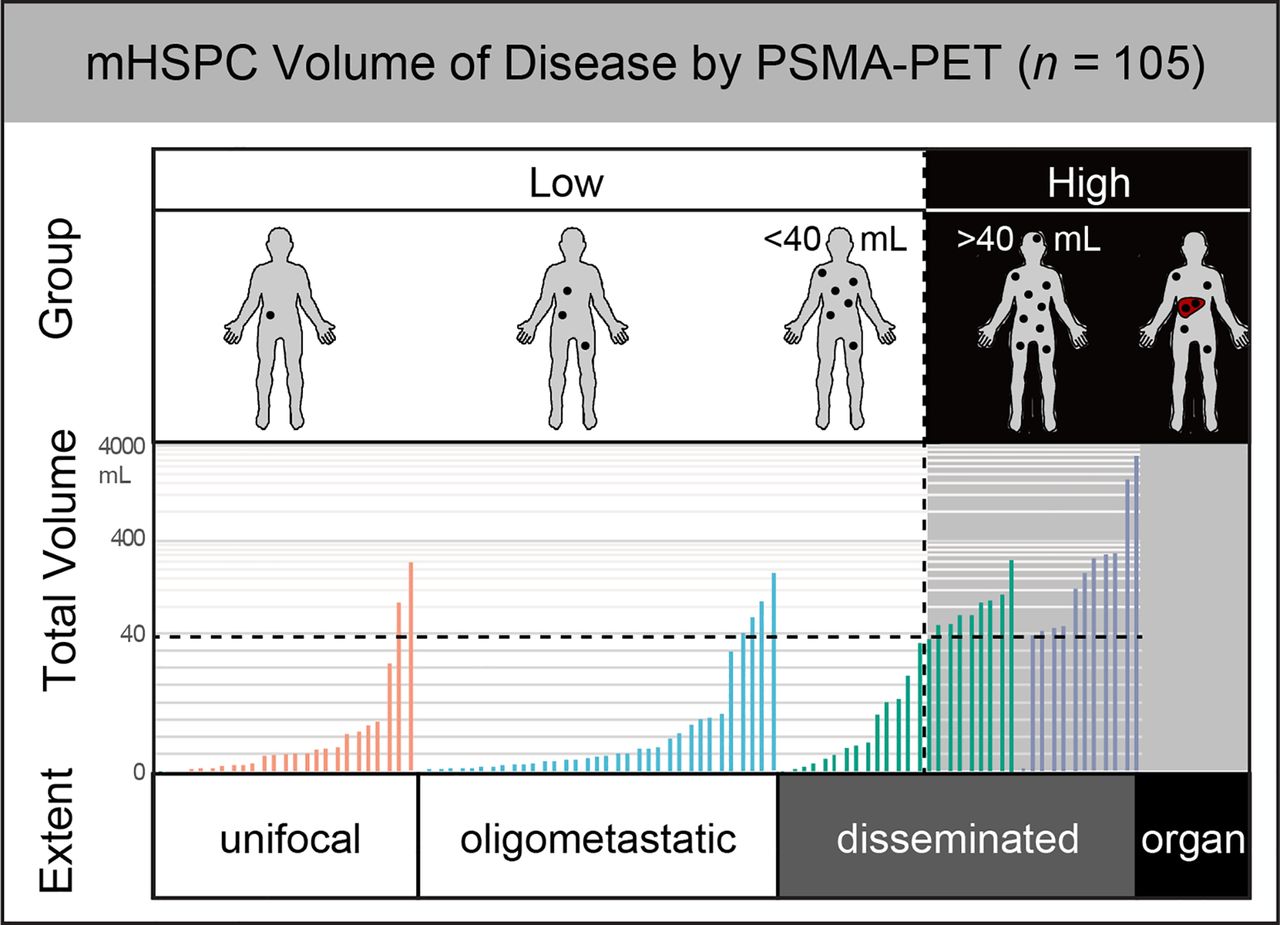
Visual Abstract
Abstract
Conventional imaging of low-volume disease (LVD) versus high-volume disease (HVD) is associated with survival in metastatic hormone-sensitive prostate cancer (mHSPC) according to the CHAARTED trial (Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer) and the STAMPEDE trial (Systemic Therapy for Advanced or Metastatic Prostate Cancer: Evaluation of Drug Efficacy). We propose a compatible quantitative PSMA PET framework for disease volume assessment in mHSPC. Methods: Three PET centers screened their PSMA PET database for mHSPC patients. CT versus PSMA PET stage, lesion number, and classification of LVD versus HVD were determined by 1 masked reader; PSMA-positive tumor volume was quantified semiautomatically. Results: In total, 85 CT-based CHAARTED LVD and 20 CT-based CHAARTED HVD patients were included. A PSMA tumor volume of about 40 cm3 was the optimal cutoff between CT-based CHAARTED LVD (nonunifocal) and HVD (non-M1c) (area under the curve, 0.86). Stratification into PET LVD (unifocal or oligometastatic/disseminated < ∼40 cm3) and PET HVD (oligometastatic/disseminated ≥ ∼40 cm3 or M1c) had 13% misalignment with the CHAARTED criteria. Conclusion: PSMA PET criteria with volume quantification deliver comparable LVD/HVD discrimination with additional subgroups for unifocal, oligometastatic, and disseminated disease, critical for guidance of targeted or multimodal therapy.
In the CHAARTED trial (Chemo Hormonal Therapy Versus Androgen Ablation Randomized Trial for Extensive Disease in Prostate Cancer), metastatic hormone-sensitive prostate cancer (mHSPC) patients with high-volume disease (HVD) particularly benefited from combined chemohormonal treatment (1). In addition, the STAMPEDE trial (Systemic Therapy for Advanced or Metastatic Prostate Cancer: Evaluation of Drug Efficacy) has shown improved failure-free survival in metastatic prostate cancer patients with low-volume disease (LVD) undergoing radiotherapy of the primary tumor (2). Beyond their primary goals, CHAARTED and STAMPEDE underline the importance of tumor burden assessment for the prediction of treatment response. In both trials, tumor burden assessment was based on conventional imaging, such as CT, MRI, and bone scans. However, novel prostate-specific membrane antigen (PSMA) ligand PET demonstrates superior accuracy for prostate cancer localization at initial diagnosis and biochemical recurrence and for advanced disease (3–5). PSMA PET further offers automatic disease volume quantification (6). Superior imaging properties, growing availability, and novel applications such as guidance of targeted therapy necessitate an updated framework for mHSPC tumor volume assessment.
PSMA PET accuracy improves selection of treatment pathways and guidance of local and systemic therapy. The potential of metastasis-directed treatment for disease control, which may delay the need for systemic treatment, has recently been shown (7).
The aim of this retrospective study was to define novel PSMA PET mHSPC disease volume criteria that are compatible with CHAARTED/STAMPEDE and offer improved assessment such as automatic or semiautomatic volume quantification and identification of unifocal to oligometastatic disease subgroups.
MATERIALS AND METHODS
Patients
PSMA PET databases of 3 high-volume PET centers (University Hospital Essen, Technical University of Munich, and University Hospital Münster) were screened for prostate cancer patients meeting the following 2 inclusion criteria, which were adapted from the criteria in the CHAARTED study: the first is metastases on CT, and the second is hormone-sensitive prostate cancer, defined as either no history of androgen deprivation therapy or concurrent androgen deprivation therapy for no more than 120 d without progression or prior androgen deprivation therapy (duration, ≤24 mo, no progression within 12 mo of completion).
The retrospective analysis was approved by the local ethics committee (University Duisburg–Essen, faculty of medicine; protocol 18-8094-BO), and the requirement for study-specific consent was waived.
Image Acquisition
All PET images were acquired on a Siemens Biograph mCT after administration of a mean of 128 MBq (interquartile range [IQR], 93.8–148.3 MBq) of 68Ga-PSMA11 (n = 79) or 333 MBq (IQR, 270.5–386.9 MBq) of 18F-rhPSMA (n = 17) or 328 MBq (IQR, 292.5–356.0 MBq) of 18F-PSMA1007 (n = 9) and an uptake interval of 70 min (IQR, 59–80 min).
Image Analysis
PET/CT and the corresponding CT dataset were anonymized separately and read by 1 masked central reader with at least 2 wk between PET/CT and CT reading sessions using OsiriX MD (Pixmeo SARL). Pathologic findings were assessed for 5 regions (prostate bed, pelvic lymph nodes, extrapelvic lymph nodes, bones, and viscera), including number of lesions and subregions involved in accordance with the PROMISE molecular imaging TNM classification (8). In accordance with CHAARTED, HVD was defined as the presence of visceral metastases or at least 4 bone metastases (≥1 beyond the vertebral bodies or the pelvis) based on the CT dataset (1). PSMA-positive tumor volume (PET volume) segmentation was performed semiautomatically using qPSMA software (6). For this segmentation, tumor lesions were localized on the CT scan and segmented on the PET scan with a freehand isocontour using an SUV higher than 3.0 (bone tissue) or higher than the mean liver uptake (soft tissue) as thresholds, respectively.
Statistical Analysis
Descriptive statistics are provided. To assess the PET volume optimal cutoff for CT-based CHAARTED HVD versus LVD, a receiver-operating-characteristic (ROC) area under the curve with the Youden J index was used after excluding patients with unifocal or M1c disease. The statistical analysis was performed using SPSS software, version 26.0 (IBM Corp.). ROC curves were compared using the methodology of Hanley and McNeil (9) on MedCalc Statistical Software, version 19.7.1 (MedCalc Software).
RESULTS
Patients’ Characteristics
One hundred five patients were included; the median age was 68.2 y (IQR, 65–73 y), and median PSA was 2.6 ng/mL (IQR, 0.9–7.9 ng/mL). Gleason score was at least 8 in 56 of 105 patients (53%). Primary treatment was radical prostatectomy in 78 of 105 patients (74%); 5 of 105 patients (5%) had undergone primary radiotherapy, and 16 of 105 (15%) had either prior or concurrent treatment with androgen deprivation therapy. A subgroup of 40 of 105 patients (38%) had 3 y of follow-up since PSMA PET. Of these, 5 patients (12.5%) died from prostate cancer (Fig. 1). Of these 5 patients, 4 had CT-based CHAARTED and PET HVD and 1 had CT-based CHAARTED LVD and PET HVD. Sixty-five of 105 patients (62%) had less than 3 y of follow-up and were alive.
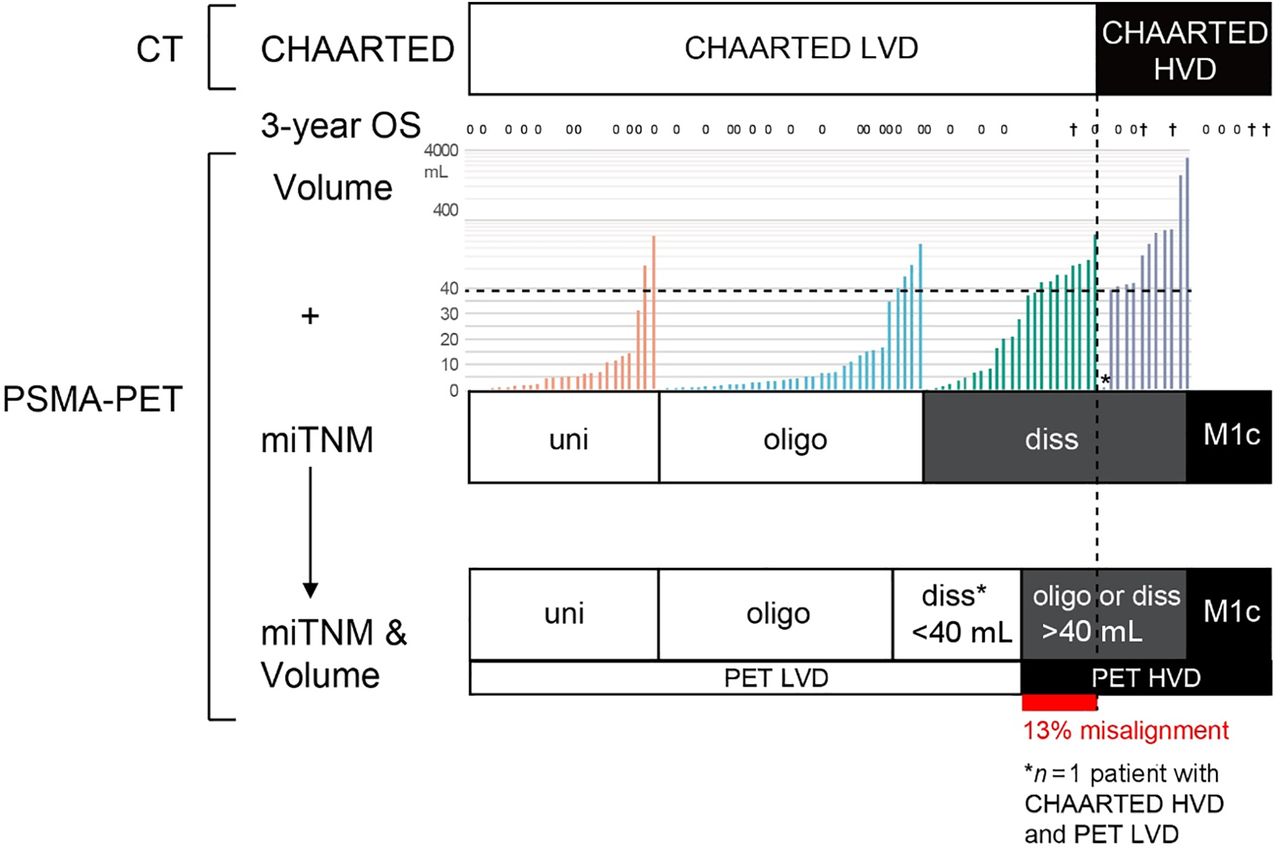
mHSPC disease extent as stratified by CT using CHAARTED criteria and PET using tumor volume and miTNM. Criteria for combined (miTNM and volume) PET volume-of-disease assessment are shown. Dashed line indicates area under curve for approximate 40-cm3 cutoff between PET LVD and PET HVD. Three-year overall survival is given for 40 patients (0 = alive; † = died; all others alive and 3 y after PET not yet reached). diss = disseminated; oligo = oligometastatic; uni = unifocal.
Supplemental Table 1 gives an overview of the patients’ characteristics (supplemental materials are available at http://jnm.snmjournals.org).
CT Disease Extent
Among the 105 patients, 1 (1%) had pelvic involvement only, 5 (5%) extrapelvic nodal involvement only (M1a), 8 (8%) any visceral involvement (M1c), and 91 (87%) any bone involvement. Eighty-five patients had CHAARTED LVD and 20 HVD (8 with visceral metastases and 12 with extensive bone involvement).
PSMA PET Disease Extent
Among the 105 patients, 1 (1%) had pelvic involvement only, 3 (3%) extrapelvic nodal involvement only (M1a), 10 (10%) any visceral involvement (M1c), and 91 (87%) bone involvement without visceral metastases. Table 1 summarizes changes for CT versus PSMA PET tumor extent on a lesion basis. When compared with CT findings, more lesions were found in 65 of 105 patients (62%), resulting in upstaging in 42 of 105 (40%). Overall, 25 of 105 patients (24%) had unifocal disease on PSMA PET, 39 of 105 (37%) had oligometastatic disease, and 41 of 105 (39%) had multifocal disease. Supplemental Table 2 gives an overview of TNM stage migration.
mHSPC Disease Extent by CT Versus PSMA PET
When formally applying the CHAARTED criteria to PET, we found that PSMA PET led to hypothetical migration to CHAARTED HVD in 16 of 85 (19%) patients due to the detection of additional bone metastases (14/85, 16.5%) or visceral metastases (2/85, 2%). To optimize alignment of CT-based CHAARTED versus PET-based volume-of-disease classification, PET volume was assessed.
PET Volume and PET HVD Versus LVD Classification
Mean PET volume was significantly higher in CT-based CHAARTED HVD than in LVD patients (320.9 cm3 vs. 21.2 cm3; P < 0.001). ROC analysis showed an area under the curve of 0.86 for the PET volume–based classification of disease volume with 38.8 cm3 (termed ∼40 cm3 in the following) as the optimal cutoff. An optimal cutoff was applied to define a PET volume-of-disease classification with the lowest reasonably achievable misalignment (13%) with CT-based CHAARTED criteria: PET LVD (any unifocal; oligometastatic or disseminated < ∼40 cm3) versus PET HVD (oligometastatic or disseminated ≥ ∼40 cm3; any visceral) (Fig. 1). An additional ROC analysis of only those patients who had undergone 68Ga-PSMA PET showed an area under the curve of 0.84 and confirmed the optimal cutoff to be 38.8 cm3. Comparison of both ROC curves did not show statistically significant differences (P = 0.96).
PET versus CT-based volume-of-disease misalignment is detailed in Supplemental Table 3.
DISCUSSION
In this study with similar inclusion criteria to CHAARTED, PSMA PET when compared with CT detected additional lesions in almost two thirds of mHSPC patients, leading to hypothetical CHAARTED LVD-to-HVD migration in about one fifth of patients. PSMA PET offers improvement by semiautomatic disease volume measurement. An approximately 40-cm3 PET volume cutoff for patients with oligo- to disseminated metastatic disease was implemented in newly proposed PET volume-of-disease criteria with additional groups for unifocal and low-volume oligometastatic disease. PET volume-of-disease criteria were aligned with current CT-based CHAARTED disease volume groups (13% difference).
This study demonstrated high agreement between PSMA PET and CT for the involved TNM regions in mHSPC patients. However, PSMA PET detected significantly more lesions with a quantifiable tumor volume (3–6). High accuracy enables visualization of unifocal or oligometastatic disease extent. PSMA PET may aid in target volume delineation for metastasis-directed treatment, thus potentially delaying the need for systemic treatment, as previously assessed in the ORIOLE, STOMP, and SABR/COMET studies (7,10,11). On the other hand, PSMA PET detected disseminated disease in 1 of 5 patients with uni- or oligometastatic disease on conventional imaging. Upstaging aids in accurate identification of candidates for systemic treatment and prevents standalone metastasis-directed treatment when the clinical benefit is questionable.
In addition, semiautomatic assessment of tumor volume on PSMA PET allows for reproducible classification of PET HVD versus LVD. Using an optimized approximately 40-cm3 cutoff PET volume-of-disease classification was largely compatible with the CT-based CHAARTED criteria. The higher accuracy and rapidly growing availability of PSMA PET necessitates revised disease volume definitions. However, novel PET criteria need to align with current evidence on prognostic groups within the CHAARTED and STAMPEDE trials. Proposed PET criteria may allow for more accurate patient stratification in future clinical trials. PET subdivides LVD patients into those potentially eligible for metastasis-directed treatment (unifocal or oligometastatic disease) versus those with low-volume nontargetable disseminated disease (Fig. 1).
Shortcomings of the study are the lack of correlational bone scans and missing long-term survival follow-up due to the recent introduction of PSMA PET. When compared with the CHAARTED trial, our study included a larger proportion of patients with recurrent prostate cancer after initial therapy and lower PSA values. This difference affects the comparability of results.
qPSMA tumor volume measurement has been validated using 68Ga-PSMA datasets. Therefore, caution is warranted when expanding this framework to patients staged with 18F-labeled PSMA ligands; however, inclusion of 18F-PSMA did not significantly impact the optimal PET volume cutoff in our study.
CONCLUSION
Here, we propose novel PET volume-of-disease criteria: PET LVD (any unifocal; oligometastatic or disseminated < ∼40 cm3) versus PET HVD (oligometastatic or disseminated ≥ ∼40 cm3; any visceral). Novel PET criteria demonstrate acceptable alignment with the CHAARTED and STAMPEDE groups but need to be validated in larger patient cohorts with survival follow-up.
DISCLOSURE
Wolfgang P. Fendler is a consultant for Endocyte and BTG and received personal fees from RadioMedix outside the submitted work. Ken Herrmann reports personal fees from Bayer SIRTEX, Adacap, Curium, Endocyte, IPSEN, Siemens Healthineers, GE Healthcare, Amgen, Novartis, and ymabs; personal fees and other from Sofie Biosciences; nonfinancial support from ABX; and grants and personal fees from BTG outside the submitted work. Kambiz Rahbar has received consultant fees from Bayer and ABX; lectureship fees from Janssen Cilag, Amgen, AAA, and SIRTEX; and travel expenses as an unpaid member of the steering committee of the VISION trial. Boris Hadaschik reports advisory roles for ABX, Bayer, Lightpoint Medical, Inc., Janssen R&D, Bristol-Myers-Squibb, and Astellas; research funding from German Research Foundation, Janssen R&D, Bristol-Myers-Squibb, and Astellas; and travel support from AstraZeneca, Janssen R&D, and Astellas. Matthias Eiber reports an advisory role for Blue Earth Diagnostics, Point Biopharma, Telix, and Janssen and a patent application for rhPSMA. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Does PSMA PET hold potential for improved tumor volume assessment over CT in patients with mHSPC?
PERTINENT FINDINGS: PSMA PET detects additional lesions in 62% of patients with mHSPC. Classification by virtue of quantified tumor volume and lesion number yields comparable results to conventional LVD versus HVD frameworks while providing a more accurate portrayal of true disease extent.
IMPLICATIONS FOR PATIENT CARE: The unparalleled accuracy of PSMA PET allows for improved tumor volume assessment in mHSPC and may facilitate the implementation of metastasis-directed treatment.
Footnotes
Published online May 14, 2021.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication February 11, 2021.
- Revision received March 19, 2021.





{kind=link}
{kind=link}