


Abstract
161Tb has decay properties similar to those of 177Lu but, additionally, emits a substantial number of conversion and Auger electrons. The aim of this study was to apply 161Tb in a clinical setting and to investigate the feasibility of visualizing the physiologic and tumor biodistributions of 161Tb-DOTATOC. Methods: 161Tb was shipped from Paul Scherrer Institute, Villigen-PSI, Switzerland, to Zentralklinik Bad Berka, Bad Berka, Germany, where it was used for the radiolabeling of DOTATOC. In 2 separate studies, 596 and 1,300 MBq of 161Tb-DOTATOC were administered to a 35-y-old male patient with a metastatic, well-differentiated, nonfunctional malignant paraganglioma and a 70-y-old male patient with a metastatic, functional neuroendocrine neoplasm of the pancreatic tail, respectively. Whole-body planar γ-scintigraphy images were acquired over a period of several days for dosimetry calculations. SPECT/CT images were reconstructed using a recently established protocol and visually analyzed. Patients were observed for adverse events after the application of 161Tb-DOTATOC. Results: The radiolabeling of DOTATOC with 161Tb was readily achieved with a high radiochemical purity suitable for patient application. Planar images and dosimetry provided the expected time-dependent biodistribution of 161Tb-DOTATOC in the liver, kidneys, spleen, and urinary bladder. SPECT/CT images were of high quality and visualized even small metastases in bones and liver. The application of 161Tb-DOTATOC was well tolerated, and no related adverse events were reported. Conclusion: This study demonstrated the feasibility of imaging even small metastases after the injection of relatively low activities of 161Tb-DOTATOC using γ-scintigraphy and SPECT/CT. On the basis of this essential first step in translating 161Tb to clinics, further efforts will be directed toward the application of 161Tb for therapeutic purposes.
Terbium comprises 4 medically interesting radioisotopes (149Tb, 152Tb, 155Tb, 161Tb) that are potentially useful for various applications in nuclear medicine using chemically identical radiopharmaceuticals (1). Several years ago, the production and a preliminary preclinical application of all 4 Tb radioisotopes were demonstrated at Paul Scherrer Institute in Villigen, Switzerland (2). Since then, additional studies have been performed with the aims of improving production methods (3) and investigating the potential of these radioisotopes for nuclear imaging (152Tb, 155Tb) (4,5) and targeted radionuclide therapy (149Tb, 161Tb) (6–10) in more detail. In terms of clinical translation, 152Tb was the only terbium radioisotope that was applied to patients in 2 independent proof-of-concept studies (11,12). 152Tb-DOTATOC, a somatostatin receptor agonist, was administered to a patient with a metastatic neuroendocrine neoplasm (NEN) of the ileum at Zentralklinik Bad Berka, Bad Berka, Germany (11). The PET images were convincing and, because of the relatively long half-life of 152Tb (17.5 h), image acquisition over an extended time period was feasible and enabled the visualization of the metastases (11).
161Tb is, nevertheless, at the most advanced stage of all Tb radioisotopes in terms of production and preclinical investigations. This radionuclide is of particular interest for targeted radionuclide therapy because its decay properties are similar to those of 177Lu (half-life of 161Tb: 6.95 d (13); half-life of 177Lu: 6.65 d) and because of the emission of medium-energy β¯-particles (154 keV for 161Tb; 134 keV for 177Lu). Importantly, 161Tb emits a substantial number of conversion and Auger electrons, which are believed to make 161Tb therapeutically more effective than 177Lu (14). Several theoretic dosimetry studies consistently predicted the high potential of this radionuclide for nuclear oncology purposes (15–20). Preclinically, it was consistently shown that 161Tb-labeled tumor-targeting agents delayed tumor growth in mice more effectively than their 177Lu-labeled counterparts (7,9,21). It was also demonstrated in preclinical studies as well as in clinical phantom studies that 161Tb can be visualized using SPECT because of the emission of γ-radiation and, thus, potentially can be used for dosimetry purposes and monitoring of the activity distribution in patients (7,9,22).
Lehenberger et al. demonstrated the concept of 161Tb production using the 160Gd(n,γ)161Gd → 161Tb nuclear reaction in analogy to the production of no-carrier-added 177Lu (14). More recently, this production route was stepwise optimized at Paul Scherrer Institute, enabling the preparation of 161Tb at a high activity and in a quality comparable to that of commercially available 177Lu (3).
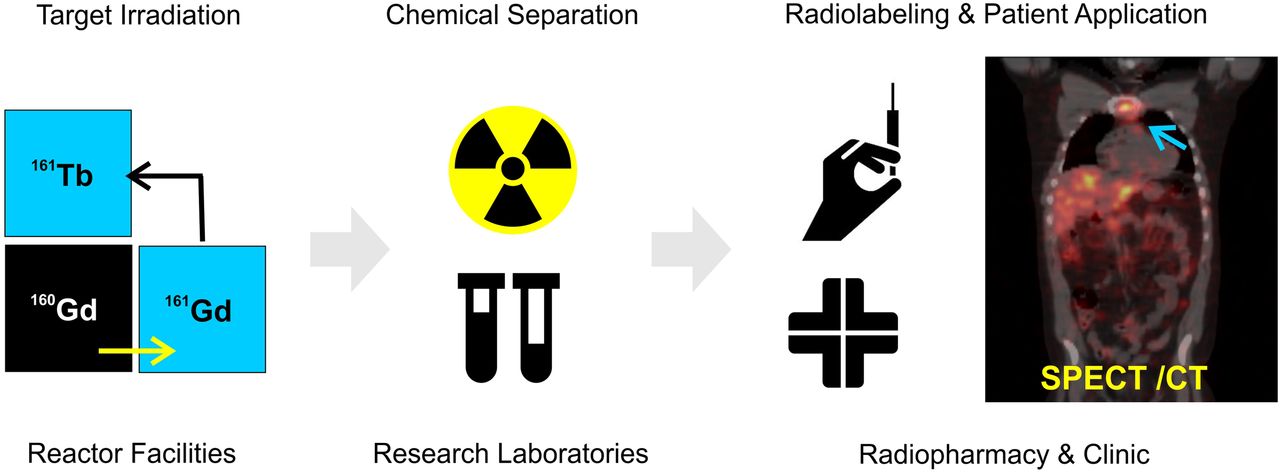
In the present study, we aimed to demonstrate first-in-humans application of 161Tb-DOTATOC. After irradiation of gadolinium targets at a high-flux reactor to obtain 161Tb, the ampoules were shipped to Paul Scherrer Institute, where 161Tb was chemically separated from its target material. The product was transported to Zentralklinik Bad Berka, where it was directly used for the radiolabeling of DOTATOC. 161Tb-DOTATOC was administered to 2 patients with NENs for whole-body planar γ-scintigraphy as well as for SPECT/CT imaging.
MATERIALS AND METHODS
Production of 161Tb
161Tb was produced using the 160Gd(n,γ)161Gd → 161Tb nuclear reaction as previously reported (3,14). In brief, enriched 160Gd targets were irradiated at the high-flux reactor at Institut Laue Langevin, Grenoble, France, or at the SAFARI-1 reactor at the South African Nuclear Energy Corp., Pelindaba, South Africa. 161Tb was chemically separated from the gadolinium target material and other impurities as previously reported (3).
Radiosynthesis of 161Tb-DOTATOC for Patient Application
The 161Tb product was used to radiolabel DOTATOC (JPT Peptide Technologies GmbH) at Zentralklinik Bad Berka. In brief, a solution of DOTATOC (60 μg and 250 μg, for Patient 1 and Patient 2, respectively) in sodium acetate buffer (500 μL, 1 M, pH 5.5) was added to a solution of 161TbCl3 in 0.05 M HCl (629 and 1,740 MBq for Patient 1 and Patient 2, respectively; 100 μL). The reaction mixture was incubated at 95°C for 30 min. Quality control was performed using an analytic high-pressure liquid chromatography system (Jasco PU-1580 system) equipped with a radiometric detector and a reversed-phase column (Jupiter Proteo; Phenomenex). The reaction solution was diluted with 5 mL of sterile saline and filtered using a 0.2-μm sterile filter. Samples were taken for sterility and endotoxin testing using an Endosafe-PTS cartridge (Charles River Endosafe MS, Germany). The pH of the final product was approximately 5.
Ethical and Regulatory Issues for Patient Application
161Tb-DOTATOC was applied to patients in compliance with the German Medicinal Products Act (section 13, subsection 2b) and the 1964 Declaration of Helsinki (including subsequent amendments). The study was approved by an institutional review board, and the patients signed written informed consent forms before the investigation, which was performed in accordance with the regulations of the German Federal Agency for Radiation Protection (23). Written informed consent was obtained from the patients for collection and storage of their data in the institutional electronic data bank and for publication of the data.
Patient Selection and Characteristics
Patient 1
A 35-y-old male patient with a well-differentiated, nonfunctional malignant right glomus caroticum tumor (paraganglioma; Ki-67, 5%) and lymph node, pulmonary, hepatic, and osseous metastases was selected for this study (Table 1; Supplemental Table 1 [supplemental materials are available at http://jnm.snmjournals.org]). On diagnosis in 2011, he underwent right neck dissection, with partial excision of the primary tumor and locoregional lymphadenectomy followed by radiochemotherapy. Further partial excision of the residual tumor with lymphadenectomy was performed in early 2017. From April to July 2017, the patient received 2 cycles of intravenously applied peptide receptor radionuclide therapy using 177Lu-DOTATOC. However, 68Ga-DOTATOC PET/CT demonstrated progressive disease in July 2017. At the time of 161Tb-DOTATOC application, the patient’s Karnofsky Performance Score was 90%.
Characteristics of Patients in This Study
Patient 2
A 70-y-old male patient with a functional NEN of the pancreatic tail (G2) and lymph node, hepatic, pulmonary, osseous, and peritoneal metastases was selected for the (Supplemental Table 1). After initial diagnosis in 1996, partial left pancreatectomy and splenectomy followed. In 2016, he was treated with everolimus; however, this treatment was stopped because of severe stomatitis. In early 2017, the patient underwent surgical debulking of the tumor, including right hemihepatectomy, excision of hepatic segment 3, extirpation of lymph nodes in the hepatoduodenal ligament area, and tumor excision from teres as well as falciform ligaments, peritoneal adhesiolysis, and cholecystectomy. From 2005 to 2017, the patient received a total of 9 cycles of peptide receptor radionuclide therapy using either an intraarterial injection of 90Y-DOTATATE or an intravenous injection of 177Lu-DOTATATE or 177Lu-DOTA-LM3, a somatostatin receptor antagonist. Despite these extensive treatments, the patient experienced disease progression, as demonstrated by somatostatin receptor antagonist (68Ga-NODAGA-LM3)–based PET/CT. At the time of 161Tb-DOTATOC application, the patient’s Karnofsky Performance Score was 80%.
SPECT/CT Imaging of 161Tb
SPECT/CT imaging was performed using a Siemens Symbia T camera system (Siemens Healthcare GmbH) with the following settings: low-energy high-resolution collimator, peak at 75 keV (energy window: 67.1–89.5 keV; 6% upper and lower scatter windows), 128 × 128 matrix, projections acquired with 30 s per step, step and shoot, and body contour. The numbers of projections for patients 1 and 2 were 64 and 120, respectively. The following γ-camera settings were used for planar whole-body imaging: MEDISO spirit DH-V dual-head γ-camera (Medical Imaging Systems), low-energy high-resolution collimator, peak at 49 keV (20% energy window) and peak at 77 keV (15% energy window), and scan speed of 15 cm/min. SPECT images were reconstructed with a Monte Carlo–based ordered-subset expectation maximization model using the Sahlgrenska Academy reconstruction code (22,24). The Sahlgrenska Academy reconstruction code simulates photon attenuation, scattering, and the collimator–detector resolution in the forward projection. The backprojection applies narrow-beam attenuation (without scattering). Six iterations and 4 subsets were used for all reconstructions.
Imaging of Patients After Application of 161Tb-DOTATOC
Patient 1
161Tb-DOTATOC (596 MBq) was administered via a dedicated radionuclide therapy application system into a peripheral arm vein (Table 2). Ondansetron and dexamethasone were administered intravenously as premedication to prevent possible adverse effects. For nephroprotection, an amino acid solution (consisting of 1,100 mL of 5% lysine HCl, 250 mL of 10% l-arginine HCl, and 250 mL of 0.9% NaCl; pH 7.4; 400 mOsm/L) was infused intravenously over a period of 4 h, along with forced diuresis using furosemide as an intravenous bolus. After the application of 161Tb-DOTATOC, 5 sets of whole-body planar (anterior and posterior) images were acquired at early time points (30 min and 3.0 h after injection), at the standard acquisition time point (24 h after injection), and at late time points (49.5 and 71 h after injection). SPECT/CT images of the thorax and of the abdomen and pelvis were acquired at 46 and 46.5 h after injection, respectively.
Application of 161Tb-DOTATOC, Premedication, and Scan Times
Patient 2
161Tb-DOTATOC (1,300 MBq) was administered using the same premedication as that described for patient 1 (Table 2). As a nephroprotective measure, diuresis was forced by the administration of furosemide, followed by adequate hydration with a balanced electrolyte solution Deltajonin (Deltamedica GmbH, Germany; 1,000 mL). After the application of 161Tb-DOTATOC, 5 sets of whole-body planar (anterior and posterior) images were acquired at early time points (30 min and 2.5 h after injection), at the standard acquisition time point after 1 d (20 h after injection), and at late time points (93 and 113 h after injection). SPECT/CT of the liver and upper abdomen was performed at 19 h after injection.
The 161Tb-DOTATOC SPECT/CT images were interpreted independently by 2 experienced physicians (2 board-certified nuclear medicine physicians, each with over 10 y of experience).
Dosimetry Estimation
Dosimetry was performed using planar image data from patients 1 and 2 in accordance with a previously described protocol (25). Time-dependent activity in the whole body and kidneys and, for patient 1, also in the liver and spleen was determined by drawing regions of interest on serial whole-body scans after the administration of 161Tb-DOTATOC. The time–activity curves of source regions were fitted to exponential functions of the first or second order to determine the time-integrated activity coefficient. The mean absorbed doses were estimated with OLINDA 2.0 software.
Clinical Safety of 161Tb-DOTATOC
The patients were monitored for adverse events, such as nausea, emesis, rash, erythema, pruritus, or fever, and potential changes in vital parameters, including blood pressure, pulse rate, and temperature, immediately after the 161Tb-DOTATOC administration and at the follow-up review. Laboratory values, such as blood cell and relevant blood plasma parameters, were measured. The estimated glomerular filtration rate, the C-reactive protein level, and relevant tumor markers were also assessed (Supplemental Table 2).
RESULTS
Production of 161Tb and Preparation of 161Tb-DOTATOC
161Tb was produced with product data specifications as previously defined by Gracheva et al. (3). The radiolabeling of DOTATOC with 161Tb was performed for patient application at Zentralklinik Bad Berka to obtain 161Tb-DOTATOC at a molar activity of 9.9–14.9 GBq/μmol. After incubation of the reaction mixture for 30 min at 95°C, 161Tb was coordinated, and no “free” (uncoordinated) 161Tb was detected by high-pressure liquid chromatography–based quality control. No microbial growth was detected in the final product when tested for sterility. The content of bacterial endotoxins in the final product was determined to be less than 10 endotoxin units/mL, in accordance with the European Pharmacopoeia (26).
First-in-Humans Application
Physiologic Biodistribution in Patient 1
Whole-body images acquired at early time points demonstrated the biodistribution of 161Tb-DOTATOC within the background soft tissue, liver, spleen, and both kidneys (Figs. 1A and 1B). Accumulation of activity in the urinary bladder was due to renal excretion of 161Tb-DOTATOC. At the standard image acquisition time point (24 h after injection), a moderate intensity of physiologically accumulated 161Tb-DOTATOC was observed in the liver, spleen, intestines, and both kidneys, with residual activity in the bladder (Fig. 1C). Delayed images acquired 3 d after application (71 h after injection) demonstrated that 161Tb-DOTATOC was continuously cleared from the normal organs and tissues (Fig. 1D). At this late time point, the spleen visually demonstrated a comparatively high accumulation of 161Tb-DOTATOC (Fig. 1D). The SPECT/CT images of the thorax, abdomen, and pelvis acquired 2 d after injection demonstrated physiologic uptake of 161Tb-DOTATOC in the liver, spleen, and both kidneys (Fig. 2).

Whole-body images of patient 1 at 0.5 h after injection (A), 3 h after injection (B), 24 h after injection (C), and 3 d (71 h) (D) after injection of 161Tb-DOTATOC. Images demonstrated physiologic biodistribution of 161Tb-DOTATOC in liver (Li), spleen (Sp), intestines (Int), and kidneys (Ki) and excretion into urinary bladder (Bl). In addition, accumulation in known osseous metastases (sternal manubrium [blue arrows] and orbital part of frontal bone on left [red arrow]) was visualized. p.i. = after injection.

Fused coronal SPECT/CT images of patient 1 obtained on the second day after injection of 161Tb-DOTATOC. Images showed pathologic uptake of 161Tb-DOTATOC in osseous metastasis (sternal manubrium [red arrow]) (A) and physiologic uptake of 161Tb-DOTATOC in kidneys (Ki), liver (Li), and spleen (Sp) (B).
Pathologic Uptake in Patient 1
Images acquired at different time points after the injection of 161Tb-DOTATOC demonstrated uptake of the radiopeptide within some of the known skeletal lesions, such as the sternum and the left frontal bone, as well as in some liver lesions. The comparatively larger sternal metastasis was evident from the images obtained 3 h after injection and onward and was persistently visualized on delayed images up to 71 h after injection. The whole-body planar images acquired at 24 h after injection demonstrated distinct uptake of 161Tb-DOTATOC in the relatively smaller lesion in the left orbital part of the frontal bone (Fig. 1C).
Fused SPECT/CT images of the thorax (46 h after injection) and of the abdomen and pelvis acquired 2 d after application demonstrated uptake of 161Tb-DOTATOC in the osseous sternal manubrium metastasis as well as heterogeneously distributed physiologic uptake in the liver and spleen (Fig. 2).
Physiologic Biodistribution in Patient 2
Images obtained at early time points (0.5 and 2.5 h) after the injection of 161Tb-DOTATOC demonstrated normal blood-pool activity, including the heart and blood vessels. Distribution of the radiopeptide was also seen in the soft tissues, liver, both kidneys, and urinary bladder (Figs. 3A and 3B). The accumulation of 161Tb-DOTATOC in the kidneys and intestinal tract was observed on images obtained at 20 h after injection (Fig. 3C). The uptake of activity in the kidneys and urinary bladder was ascribed to renal excretion of 161Tb-DOTATOC, as is commonly also the case for 177Lu-DOTATOC. 161Tb-DOTATOC was effectively cleared from normal tissues over time, as demonstrated by the reduced activity seen on images acquired at delayed time points (Fig. 3D). SPECT/CT images acquired at 19 h after injection demonstrated physiologic distribution of 161Tb-DOTATOC in both kidneys as well as normal liver tissue (Fig. 4).

Whole-body images of patient 2 at 0.5 h after injection (A), 2.5 h after injection (B), 20 h after injection (C), and 113 h after injection (D) of 161Tb-DOTATOC. Early blood-pool activity was noted in heart (H) and blood vessels (BV) up to 2.5 h after injection. Physiologic uptake of radiopeptide was observed in soft tissues, liver (Li), kidneys (Ki), intestines (Int) and urinary bladder (Bl). Pathologic accumulation of 161Tb-DOTATOC was demonstrated in bilobar liver (blue arrows) and multifocal osseous metastases (red arrows). p.i. = after injection.

SPECT/CT images of patient 2 at 19 h after injection of 161Tb-DOTATOC. (A) Coronal section. (B) Sagittal section. (C) Transverse section. Images showed uptake of 161Tb-DOTATOC in bilobar hepatic metastases (yellow arrows) as well as multiple osteoblastic skeletal metastases in vertebral column and pelvis (red arrows). Physiologic uptake of 161Tb-DOTATOC was seen in both kidneys (Ki) as well as in liver (Li).
Pathologic Uptake in Patient 2
Whole-body planar images obtained at multiple time points demonstrated that the accumulation of 161Tb-DOTATOC in bilobar hepatic metastases as early as 0.5 h after injection was still seen on images acquired at late time points (113 h after injection). Multiple skeletal metastases demonstrated faint uptake of the radiopeptide on (early) images at 2.5 h after injection of 161Tb-DOTATOC, with further significant accumulation visible on images acquired at 113 h after injection (Fig. 3). SPECT/CT of the liver and upper abdomen acquired at 19 h after injection demonstrated significant accumulation of 161Tb-DOTATOC in the hepatic metastases as well as moderate uptake in the multiple osseous lesions of the thoracolumbar vertebrae and the pelvis (Fig. 4).
Dosimetry Estimation
Dosimetry data from patient 1 were in a range similar to that expected when using 177Lu-DOTATOC (Supplemental Table 3). Patient 2 showed slower renal clearance of 161Tb-DOTATOC and, hence, higher absorbed kidney and whole-body doses (1.5 and 0.07 Gy/GBq, respectively) than patient 1 (0.8 and 0.04 Gy/GBq, respectively).
Clinical Safety of 161Tb-DOTATOC
The administration of 161Tb-DOTATOC and postapplication imaging procedures were well tolerated by both patients. No adverse events were reported by the patients and no significant changes in vital parameters were observed or reported by the patients during, immediately after, or at follow-up review after the administration of 161Tb-DOTATOC. According to the Common Terminology Criteria for Adverse Events (CTCAE v5.0) (27), there were no clinically significant changes in relevant laboratory values (hematologic, renal, and hepatic panels) at the subsequent follow-up of the patients after the administration of 161Tb-DOTATOC (Supplemental Table 2).
DISCUSSION
161Tb was suggested for clinical translation because of its favorable physical decay properties (16,18–20). Importantly, 161Tb can be stably coordinated with a DOTA chelator because of its chemical similarity to 177Lu. Therefore, it can be applied with, potentially, any tumor-targeting agent that comprises a DOTA chelator, as demonstrated in several preclinical studies (5,7,9,11).
The feasibility of using the emitted γ-radiation of 161Tb for clinical SPECT was recently demonstrated with human phantoms (22). Low-energy high-resolution collimators were revealed to be most suited to obtaining high-resolution images, and SPECT/CT-based dosimetry was predicted to be feasible for 161Tb-labeled radiopharmaceuticals (22). To our knowledge, the data presented in this article are the first results for 161Tb clinical imaging in patients.
Two patients with somatostatin receptor–expressing malignancies received 161Tb-DOTATOC to analyze the distribution of the radiopeptide visualized on postapplication whole-body planar and SPECT/CT imaging. The resultant images showed a distribution profile for 161Tb-DOTATOC similar to that expected for 177Lu-DOTATOC. Considering that high interpatient as well as high intrapatient variations in dosimetry data are expected (25), the dosimetry results for the 2 patients who received 161Tb-DOTATOC are of minor informative value. They confirmed, however, the expected tissue distribution of 161Tb-DOTATOC. The comparatively higher absorbed kidney and whole-body doses in patient 2 can be ascribed to the slower renal clearance of 161Tb-DOTATOC in this patient; the slower clearance was due to the reduced renal function demonstrated by elevated renal plasma parameters (Supplemental Table 2) (28).
In patient 1, despite the low administered activity of 161Tb-DOTATOC, the resultant images visualized previously known osseous metastases, in agreement with visualization of the lesions on the PET/CT scan performed the previous week using 68Ga-DOTATOC (Fig. 5). It is not surprising that not all of the pathologic lesions observed on 68Ga-DOTATOC PET/CT images were visualized on SPECT images, which generally have lower sensitivity than high-resolution, state-of-the-art diagnostic PET/CT images. In agreement with diagnostic PET/CT images, high accumulation of 161Tb-DOTATOC was found in the spleen; this was a peptide-specific feature (29). Patient 2 had undergone a splenectomy; consequently, the accumulation of activity in the spleen was not observed in this patient and, therefore, dosimetry data were not available.

PET/CT sagittal section of patient 1 at 60 min after injection of 68Ga-DOTATOC. Pathologic uptake was seen in multiple skeletal metastases (sternal manubrium, left orbital part of frontal bone, occipital bone, and multiple vertebrae [red arrows]). Comparatively higher physiologic uptake of 68Ga-DOTATOC was observed in spleen (Sp). Accumulation of activity in urinary bladder (Bl) was seen because of renal excretion of radiopeptide.
Images acquired after the application of 161Tb-DOTATOC in patient 2 demonstrated significant radiopeptide uptake in bilobar hepatic as well as multifocal osseous metastases, with visually excellent target-to-background ratios (Fig. 4). The somewhat better image quality and detection of more pathologic lesions for patient 2 were ascribed to the fact that about twice as much activity was applied in this case. Because of multiple heterogeneously distributed and difficult to delineate liver metastases in this patient, dosimetry data for the liver could not be determined.
In both patients, 161Tb-DOTATOC was well tolerated, without any signs of adverse events during or after the procedure, indicating that the application of 161Tb-DOTATOC is safe.
There is no doubt that 161Tb holds promise as an alternative to 177Lu for peptide receptor radionuclide therapy; however, it may be important to use a targeting agent that will fully exploit the short-range electron emission.
CONCLUSION
The patient images obtained with 161Tb in the present study confirmed that the emitted γ-radiation of 161Tb can be used for whole-body planar as well as SPECT/CT imaging of even low activities of injected 161Tb. The results of the present study will serve as a basis for further investigations in patients with 161Tb-based radiopharmaceuticals and a stepwise escalation of the 161Tb activity applied, thereby achieving therapeutic efficacy.
DISCLOSURE
Roger Schibli, Nicholas P. van der Meulen, Cristina Müller, and Richard P. Baum received the Neuroendocrine Tumor Research Foundation (NETRF) Peterson Investigator Award 2018 (United States), which was a major contribution to the funding of this project. Peter Bernhardt and Tobias Rydén were supported by the Swedish Cancer Society, Swedish Radiation Safety Authority, King Gustav V. Jubilee Clinic Cancer Research Foundation, Swedish Research Council, and Swedish State under an agreement between the Swedish government and the county councils (the ALF agreement). No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is it feasible to visualize metastases in patients with NENs after injection of 161Tb-DOTATOC?
PERTINENT FINDINGS: This first-in-humans application of 161Tb demonstrated the feasibility of imaging metastases of NENs after the injection of relatively low activities of 161Tb-DOTATOC using γ-scintigraphy and SPECT.
IMPLICATIONS FOR PATIENT CARE: The feasibility of imaging 161Tb in patients is an essential finding in view of 161Tb-based radionuclide therapy in future clinical trials.
ACKNOWLEDGMENTS
We thank Lebogang Sepini at Necsa for arrangements with the shipment of irradiated targets from South Africa to Switzerland. We also thank the people responsible for radiation safety, transport of radioactive materials, and technical assistance at Paul Scherrer Institute. Furthermore, we thank the nursing staff as well as the nuclear medicine technologists for patient management at Zentralklinik Bad Berka.
Footnotes
↵* Contributed equally to this work.
Published online February 5, 2021.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication October 16, 2020.
- Accepted for publication January 19, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.