


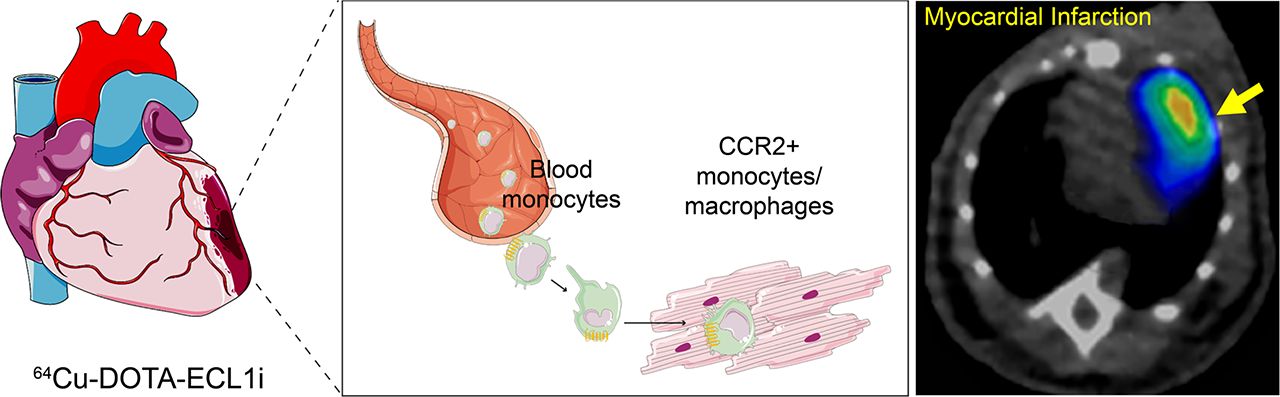
Visual Abstract
Abstract
Proinflammatory macrophages are important mediators of inflammation after myocardial infarction and of allograft injury after heart transplantation. The aim of this study was to image the recruitment of proinflammatory chemokine receptor 2–positive (CCR2+) cells in multiple heart injury models. Methods: 64Cu-DOTA-extracellular loop 1 inverso (ECL1i) PET was used to image CCR2+ monocytes and macrophages in a heart transplantation mouse model. Flow cytometry was performed to characterize CCR2+ cells. Autoradiography on a human heart specimen was conducted to confirm binding specificity. 64Cu- and 68Ga-DOTA-ECL1i were compared in an ischemia–reperfusion injury mouse model. Results: 64Cu-DOTA-ECL1i showed sensitive and specific detection of CCR2+ cells in all tested mouse models, with efficacy comparable to that of 68Ga-DOTA-ECL1i. Flow cytometry demonstrated specific expression of CCR2 on monocytes and macrophages. The tracer binds to human CCR2. Conclusion: This work establishes the utility of 64Cu-DOTA-ECL1i to image CCR2+ monocytes and macrophages in mouse models and provides the requisite preclinical information to translate the targeted clinical-grade CCR2 imaging probe for clinical investigation of heart diseases.
Within the heart, macrophages represent the most abundant immune cell type and have important roles in potentiating both inflammatory and reparative responses after cardiac injury. Recent studies have shown that chemokine receptor 2–positive (CCR2+) monocytes and macrophages, recruited to the site of myocardial injury, are important mediators of adverse remodeling in myocardial infarction (MI), heart failure pathogenesis, and inflammation after heart transplantation. Thus, CCR2+ cells represent a potential therapeutic target to improve outcomes in the above disease settings (1–3).
Though some PET tracers have been developed for MI imaging (4–6), these probes lack specificity in visualizing cell types important to the remodeling process. Molecular imaging of CCR2+ monocytes and macrophages provides not only a sensitive approach to determine a specific mechanism of myocardial inflammation that is therapeutically targetable but also a strategy to facilitate the selective delivery of immunomodulatory agents to cardiovascular patients who are most likely to benefit.
Previously, we reported the capacity of a targeted PET tracer to quantify the CCR2-specific inflammation burden in multiple animal models using extracellular loop 1 inverso (ECL1i) peptide through 64Cu or 68Ga radiolabel (7–9). The PET signal intensity in inflammatory tissues was corroborated by molecular characterization of CCR2 expression and correlated with disease progression and regression. Currently, 64Cu radiolabeled ECL1i (64Cu-DOTA-ECL1i) is approved by the Food and Drug Administration for clinical investigations to identify CCR2+ cells in humans (10). To explore its potential for imaging patients with heart injury, we assessed the sensitivity and specificity of 64Cu-DOTA-ECL1i CCR2+ monocyte and macrophage abundance in preclinical models of heart transplantation and MI and in comparison with 68Ga radiolabeled analog. These studies provided strong support to apply the CCR2 PET imaging strategy to human subjects.
MATERIALS AND METHODS
Mouse Heart Injury Models
For the heart transplantation mouse model, cardiac grafts harvested from wild-type (WT) C57BL/6 mice were transplanted into the right neck of C57BL/6 LysM-GFP or CCR2 knockout (CCR2−/−) recipient mice after 1 h of cold (4°C) ischemia as previously described (11). The ischemia–reperfusion injury mouse model was developed in 2- to 4-mo-old C57BL/6 mice by following a reported protocol (9).
Radiolabeling of DOTA-ECL1i with 64Cu and 68Ga
The synthesis of DOTA-ECL1i and radiolabeling with 64Cu and 68Ga were reported previously (9,12). The radiochemical purities for both tracers were more than 95% before administration to mice.
PET/CT Imaging and Biodistribution
All animal studies were performed in compliance with guidelines set forth by the National Institutes of Health Office of Laboratory Animal Welfare and approved by the Washington University institutional animal care and use committee. At 1–2 h after heart transplantation (2,13), PET/CT (Siemens; 40- to 60-min dynamic scan) with 64Cu-DOTA-ECL1i was performed after tail-vein injection. For mice with ischemia–reperfusion injury, PET/CT was done at day 3 after injury with 68Ga-DOTA-ECL1i and at day 4 with 64Cu-DOTA-ECL1i and quantified as previously reported (9,12). A post-PET biodistribution study in the heart transplant model was performed immediately after imaging (8).
Flow Cytometry
To characterize the expression of CCR2, saline-perfused cardiac tissue specimens were collected and processed as previously reported. Fluorescence-activated cell sorting analysis was performed on an LSR II platform (BD) (9).
Autoradiography
Human pathologic specimens were obtained under Institutional Review Board protocol 201305086, approved by the Washington University Human Research Protection Office. Fixed sections of human heart tissue were used to test the binding of 64Cu-DOTA-ECL1i to human CCR2. Competitive receptor blocking studies were also performed to verify the binding specificity, using previously reported methods (8,9).
Statistics
Data were analyzed using GraphPad Prism (version 6.07). Differences between groups were compared using paired parametric or unpaired nonparametric 2-tailed t tests. A P value of less than 0.05 was indicative of a statistically significant difference.
RESULTS
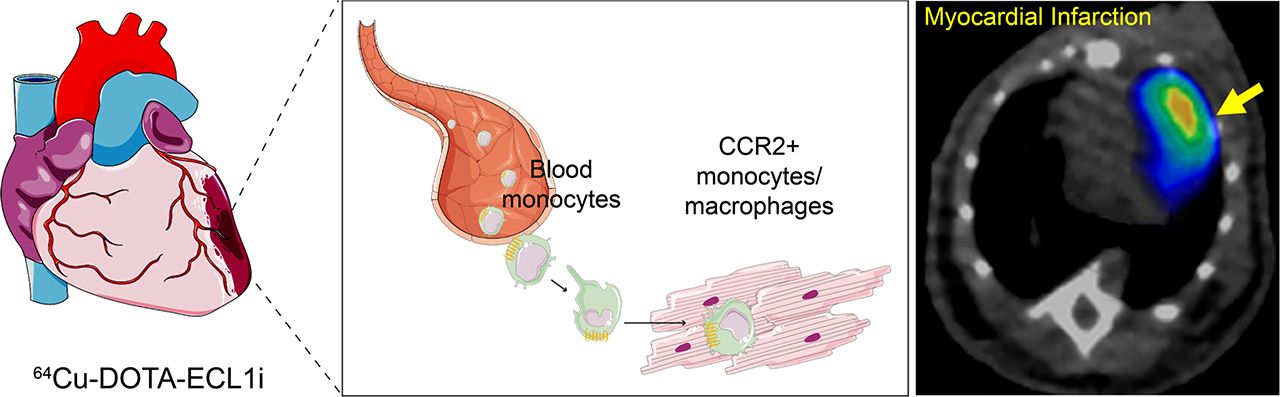
The sensitivity and specificity of 64Cu-DOTA-ECL1i to image CCR2+ cells were assessed in mouse syngeneic heterotopic heart transplant models. In this model, hearts from WT mice were harvested, placed on ice for 1 h, and subsequently transplanted in the cervical position of either a WT recipient mouse or a CCR2−/− mouse. As shown in Figure 1A, besides rapid renal clearance as previous reported (12), PET/CT imaging revealed intensive signal in the donor heart but minimal tracer retention in the native heart in the WT→WT mouse heart transplantation model. In the WT→CCR2−/− model (Fig. 1B), a similar profile was detected, with tracer uptake in the donor heart and marginal accumulation in the native heart. Quantitative uptake analysis showed that tracer accumulation in the donor heart (3.51 ± 0.19 percentage injected dose [%ID]/g, n = 4) was approximately 4 times higher than that in the native heart (0.72 ± 0.08 %ID/g, P < 0.0001, n = 4) in the WT→WT model (Fig. 1C). In the WT→CCR2−/− model (Fig. 1C), a 5-fold higher difference in tracer accumulation was determined in the donor heart (1.46 ± 0.16 %ID/g, n = 3) than in the native heart (0.25 ± 0.06 %ID/g, P < 0.0001, n = 3). Moreover, the donor heart tracer uptake in the WT→WT model was 1.4-fold (P < 0.0001, n = 3–4) higher than that in the WT→CCR2−/− model, whereas the difference was approximately 5-fold (P < 0.0001, n = 3–4) for the native hearts in the 2 models. This difference was likely a result of reduced infiltration of recipient CCR2+ cells from CCR2−/− recipients into the graft, as was reported in the ischemia–reperfusion injury model after lung transplantation (12). Of note, tracer uptake was evident within donor hearts transplanted into CCR2−/− recipients. This finding is likely due to the persistence of CCR2+ resident macrophages after transplantation, a population of cells that are activated after ischemia–reperfusion injury and orchestrate infiltration of peripheral monocytes and neutrophils (2,13).

64Cu-DOTA-ECL1i imaging of CCR2 in heart transplantation models. (A and B) 64Cu-DOTA-ECL1i PET/CT images (maximum-intensity projection) showing significant signal in transplanted heart (yellow arrow) and weak accumulation in native heart (white arrow) in WT→WT model (A) and WT→CCR2−/− model (B). (C) Quantitative uptake analysis of native and donor hearts of 2 models (WT→WT and WT→CCR2−/−). (D) Flow cytometry assay showing 3-fold more CCR2+ cells in transplanted heart than in native heart in WT→WT model. (E) Post-PET biodistribution showing 3-fold higher uptake in donor heart than in native heart in WT→WT model. (F) Autoradiographic images of 64Cu-DOTA-ECL1i on human MI specimens revealing heterogeneous tracer binding. Competitive blocking using excess nonradioactive ECL1i shows decreased tracer binding. ****P < 0.0001, assessed by 1-way ANOVA.
We have previously demonstrated that recipient CCR2+ monocytes and macrophages accumulated within the transplanted heart after transplantation (2). In agreement, flow cytometry analysis of the WT→WT model revealed abundant CCR2+ monocytes and macrophages in the transplanted donor heart as compared with the native heart 2 d after heterotopic heart transplantation (Fig. 1D). Furthermore, post-PET biodistribution showed that tracer uptake in the donor heart (2.82 ± 0.40 %ID/g) was 4 times that in the native heart (0.70 ± 0.19 %ID/g, P < 0.0001, n = 4) (Fig. 1E), supporting PET data. In contrast to the bone marrow uptake (0.57 ± 0.16 %ID/g, n = 4) in naïve mice (8), tracer localization in the marrow (2.33 ± 0.51 %ID/g) of the WT→WT model was also 3 times higher, indicating the increased production and accumulation of CCR2+ monocytes within the bone marrow compartment.
To further assess the potential of 64Cu-DOTA-ECL1i for human cardiac injury imaging, the binding of 64Cu-DOTA-ECL1i to human CCR2 was evaluated in human MI specimens, which are known to contain CCR2+ monocytes and macrophages, using autoradiography (9). A substantial and heterogeneous binding profile was observed in human MI tissues, which was blocked by excess nonradioactive ECL1i peptide (Fig. 1F), indicating the specificity of 64Cu-DOTA-ECL1i binding to human hearts.
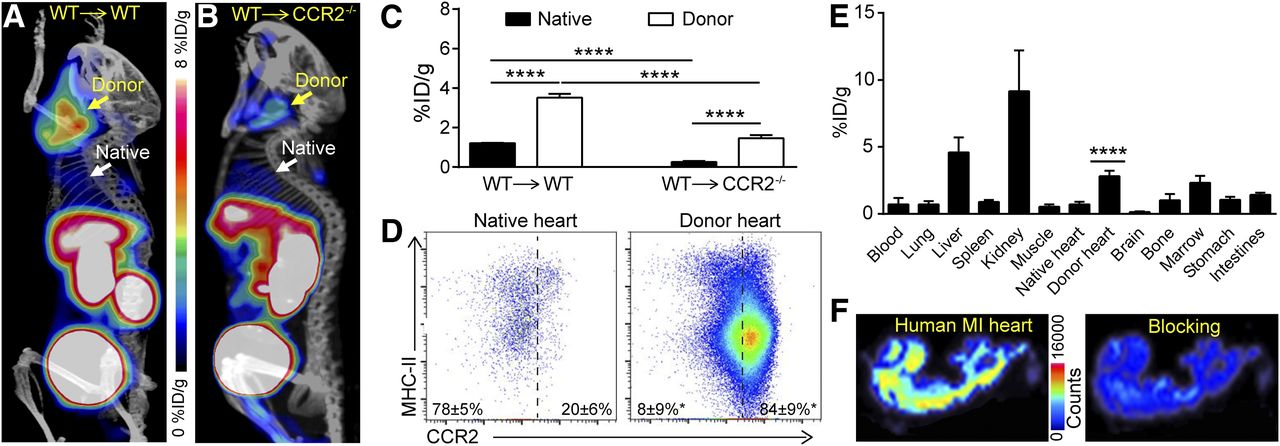
To further assess the suitability of 64Cu-DOTA-ECL1i for human cardiac injury imaging, we compared it with a 68Ga-radiolabeled analog in a previously established mouse MI model (9). 68Ga-DOTA-ECL1i and 64Cu-DOTA-ECL1i each showed significant radiotracer uptake within the infarct region 3–4 d after ischemia–reperfusion injury (Figs. 2A and 2B). Quantitative analysis in the same mouse showed that the uptake of 68Ga-DOTA-ECL1i within the heart at day 3 after injury (3.07 ± 0.33 %ID/g, n = 6) was comparable to that acquired a day later using 64Cu-DOTA-ECL1i (2.71 ± 0.28 %ID/g, n = 6). These data are also comparable to 68Ga-DOTA-ECL1i uptake at day 4 after MI (2.53 ± 0.52 %ID/g, n = 6) (9), indicating equivalent sensitivity of 64Cu-DOTA-ECL1i and 68Ga-DOTA-ECL1i for detecting CCR2+ cells within the infarcted heart.

64Cu-DOTA-ECL1i compared with 68Ga-DOTA-ECL1i–mediated imaging of CCR2 in injured heart. Representative PET/CT images (transverse plane) of 68Ga-DOTA-ECL1i acquired at day 3 (A) and 64Cu-DOTA-ECL1i acquired at day 4 (B) after MI in same mouse show comparable PET signals (C) in same infarcted region of heart.
DISCUSSION
Clinically, the identification of reliable biomarkers of inflammation is required to facilitate a timely diagnosis of heart transplant rejection and primary graft dysfunction, to identify heart failure patients at increased risk of disease progression, to elucidate pathways that contribute to the pathogenesis of these entities, and to allow for the development and appropriate use of immunomodulatory therapies. It is known that CCR2+ macrophages generate damaging inflammation by recruiting additional monocytes and neutrophils that release cytokines and oxidative products. Removal of CCR2+ macrophages is sufficient to reduce chemokine and cytokine production and monocyte and neutrophil recruitment and results in preservation of left ventricular function and suppression of pathologic remodeling after MI and heart transplantation. Thus, the precise imaging of CCR2+ macrophages has the potential to determine the severity of heart injury, provide guidance for targeted treatment, and monitor treatment response.
Herein, we report robust detection of CCR2+ monocytes and macrophages in mouse models of heart injury using a clinical-grade 64Cu-DOTA-ECL1i PET tracer. The imaging sensitivity and specificity were demonstrated using WT→WT and WT→CCR2−/− heart transplantation models. We demonstrated that the 64Cu-DOTA-ECL1i tracer provides imaging efficacy equivalent to that of our previously published 68Ga-DOTA-ECL1i tracer in a mouse MI model. We further demonstrated that the 64Cu-DOTA-ECL1i tracer binds inflamed human myocardial tissue.
Compared with 68Ga, the radioactive decay half-life of 64Cu is 10 times longer, providing an imaging agent that is ideal for multicenter translational studies. 64Cu-DOTA-ECL1i can be produced at a single center, and intact tracer can be shipped to collaborating institutions, avoiding the need for onsite 68Ge/68Ga generators or radiochemistry expertise necessary for local tracer production. More importantly, the 64Cu-DOTA-ECL1i tracer is currently approved by the U.S. Food and Drug Administration for clinical investigation under an exploratory investigational new drug application.
CONCLUSION
This study demonstrates the utility of 64Cu-DOTA-ECL1i to detect CCR2+ monocytes and macrophages in preclinical models and provides the requisite preclinical data to support translation of 64Cu-DOTA-ECL1i for clinical investigation of heart injuries.
DISCLOSURE
Yongjian Liu, Daniel Kreisel, Robert Gropler, Steven Brody, and Kory Lavine have a pending patent entitled “Compositions and Methods for Detecting CCR2 Receptors” (application 15/611,577). Daniel Kreisel serves on the Scientific Advisory Board of Compass Therapeutics. Yongjian Liu is supported by NIH R35 HL145212, R01 HL131908, and P41 EB025815. Kory Lavine is supported by NIH K08 HL123519, R01 HL138466, R01 HL139714, the Burroughs Welcome Fund (1014782), the Children’s Discovery Institute of Washington University and St. Louis Children’s Hospital (CHII-2015–462 and CH-II-2017–628), and the Foundation of Barnes–Jewish Hospital (8038-88). Daniel Kreisel is supported by 1P01AI116501, R01 HL094601, Veterans Administration Merit Review grant 1I01BX002730, and the Foundation for Barnes–Jewish Hospital. Steven Brody is supported by R01 HL131908 and is the Dorothy R. and Hubert C. Moog Professor of Pulmonary Medicine, awarded through the Barnes–Jewish Hospital Foundation. Robert Gropler is supported by P41 EB025815. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What is the feasibility of noninvasively imaging proinflammatory CCR2+ cells after heart injury?
PERTINENT FINDINGS: 64Cu-DOTA-ECL1i showed sensitive and specific detection of CCR2+ cells in mouse heart injury models, as was further confirmed by flow cytometry analysis. The tracer also binds to injured human heart specimens.
IMPLICATIONS FOR PATIENT CARE: This study provides the requisite preclinical data to support translation of 64Cu-DOTA-ECL1i for clinical investigation of heart injuries and may provide new insight into the role of inflammation during progression of human heart failure.
Acknowledgments
We thank the small-animal imaging facility and cyclotron facility at Washington University for assistance with this research.
Footnotes
↵* Contributed equally to this work.
Published online May 22, 2020.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication March 6, 2020.
- Accepted for publication April 16, 2020.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Interleukin-1{beta} Drives Disease Progression in Arrhythmogenic Cardiomyopathy
- Toward Quantitative Multisite Preclinical Imaging Studies in Acute Myocardial Infarction: Evaluation of the Immune-Fibrosis Axis
- Imaging Inflammation Past, Present, and Future: Focus on Cardioimmunology
- Radiotracers to Address Unmet Clinical Needs in Cardiovascular Imaging, Part 2: Inflammation, Fibrosis, Thrombosis, Calcification, and Amyloidosis Imaging
- The Latest Advances in Imaging Crosstalk Between the Immune System and Fibrosis in Cardiovascular Disease