


Abstract
1357
Purpose: Fluorine-18 fluorodeoxyglucose (FDG) positron emission tomography/computed tomography (PET/CT) is an useful imaging modality in lung cancer patients, but it is not yet recommended as routine study for treatment assessment in the NCCN guidelines. Positron Emission Tomography Response Criteria in Solid Tumors (PERCIST), the response assessment criteria, suggests measurement from 1 and up-to-5 lesions, but the optimal number of lesions to measure from each time point is not validated for lung cancer. We compared 1 and up-to-5 lesion measurements for response assessment in lung cancer patients using PERCIST.
Methods: Lung cancer patients with pre- and post-treatment FDG PET/CT from 2015 to 2017 were retrospectively reviewed. The standard uptake value corrected for lean body mass (SULpeak) of up-to-5 hottest target lesions were measured at each time point. The percent changes of SULpeak (Δ%SULpeak) of the single hottest lesion (1-lesion-analysis) and the sum of up-to-5 hottest lesions (5-lesion-analysis) were computed. Response category was designated according to PERCIST: complete metabolic response (CMR) when no lesion with perceptible FDG uptake remained; partial metabolic response (PMR), stable metabolic disease (SMD), or progressive metabolic disease (PMD) determined using threshold of 30% and 0.8 unit change in SULpeak; unequivocal new lesion meant PMD. Pearson correlation coefficient was measured to evaluate the strength of association between percent changes of SULpeak. The concordance for response categorization was assessed by kappa statistics.
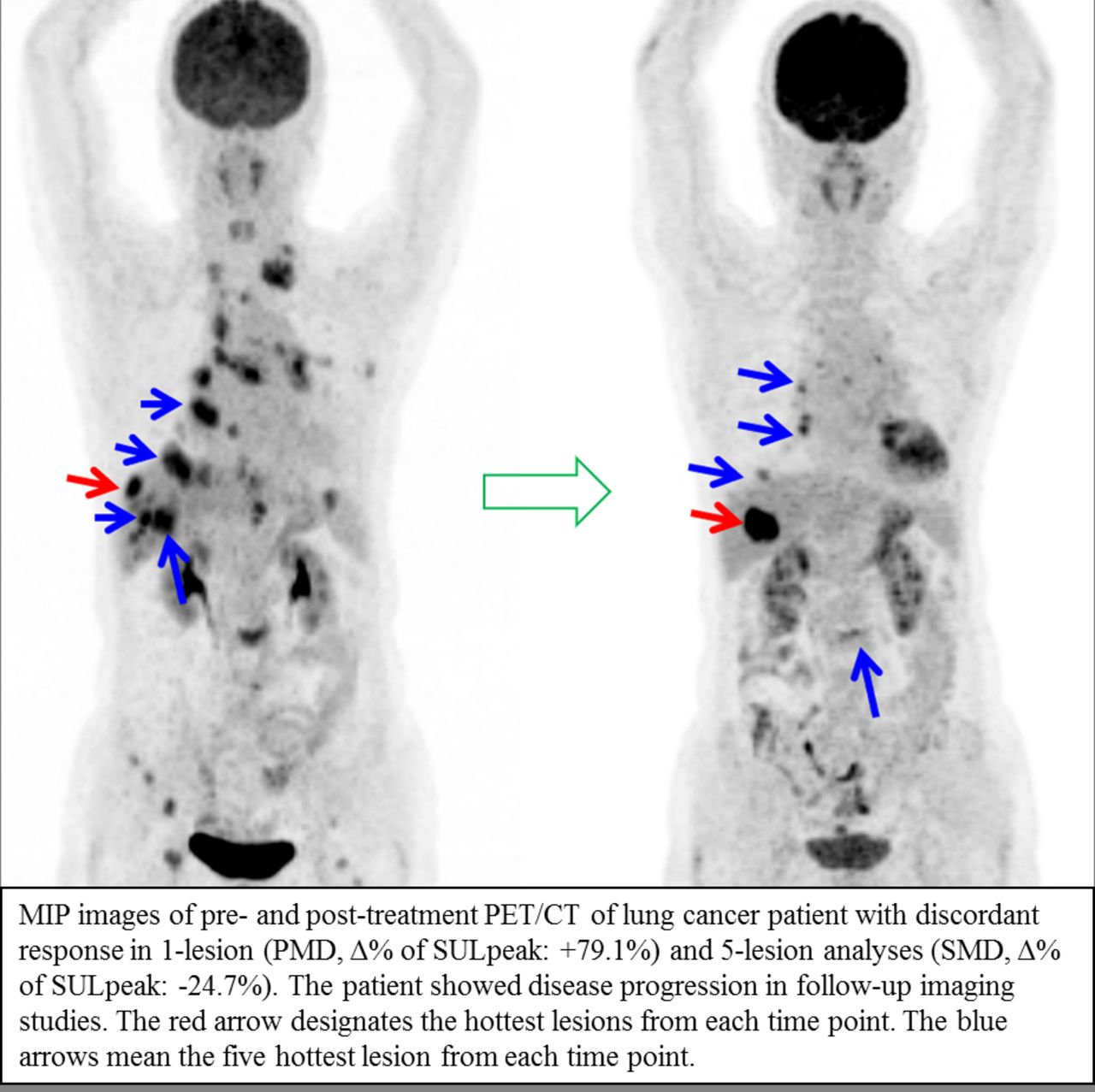
Results: Total 40 patients (25 non-small cell lung cancer; 15 small cell lung cancer) were analyzed and all patients had FDG-avid lung cancer. The median interval between pre- and post-treatment PET/CT was 30.8 weeks (12.6-60.9 weeks). Average of 3.0 target lesions were measured for 5-lesion-analysis in both pre-treatment and post-treatment PET/CTs. Pearson’s r was 0.77 (p<0.001) for all 40 patients and increased to 0.96 (p<0.001) when two outliers were excluded. One of the outliers was categorized PMD due to new lesions despite different Δ%SULpeak in 1-lesion and 5-lesion analysis (13.7% and 298.9%). The other outlier was sorted as PMD in 1-lesion analysis (Δ%SULpeak: 79.1%) and SMD in 5-lesion analysis (Δ%SULpeak: -24.7%). Response categorization with 1-lesion-analysis and 5-lesion-analysis was discordant in 3 patients (7.5%, weighted kappa=0.89). Most of the patients with PMD was attributable to new lesions (90.9% in 1-lesion analysis and 100% in 5-lesion analysis), without achieving SULpeak change criterion for PMD. Patients with CMR demonstrated Δ%SULpeak in range of -39.8% to -80.3%.
Conclusions: Analyzing 1 and up-to-5 hottest lesions at each time point for response assessment by PERCIST showed high concordance rate in patients with lung cancer patients.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.