


Abstract
242386
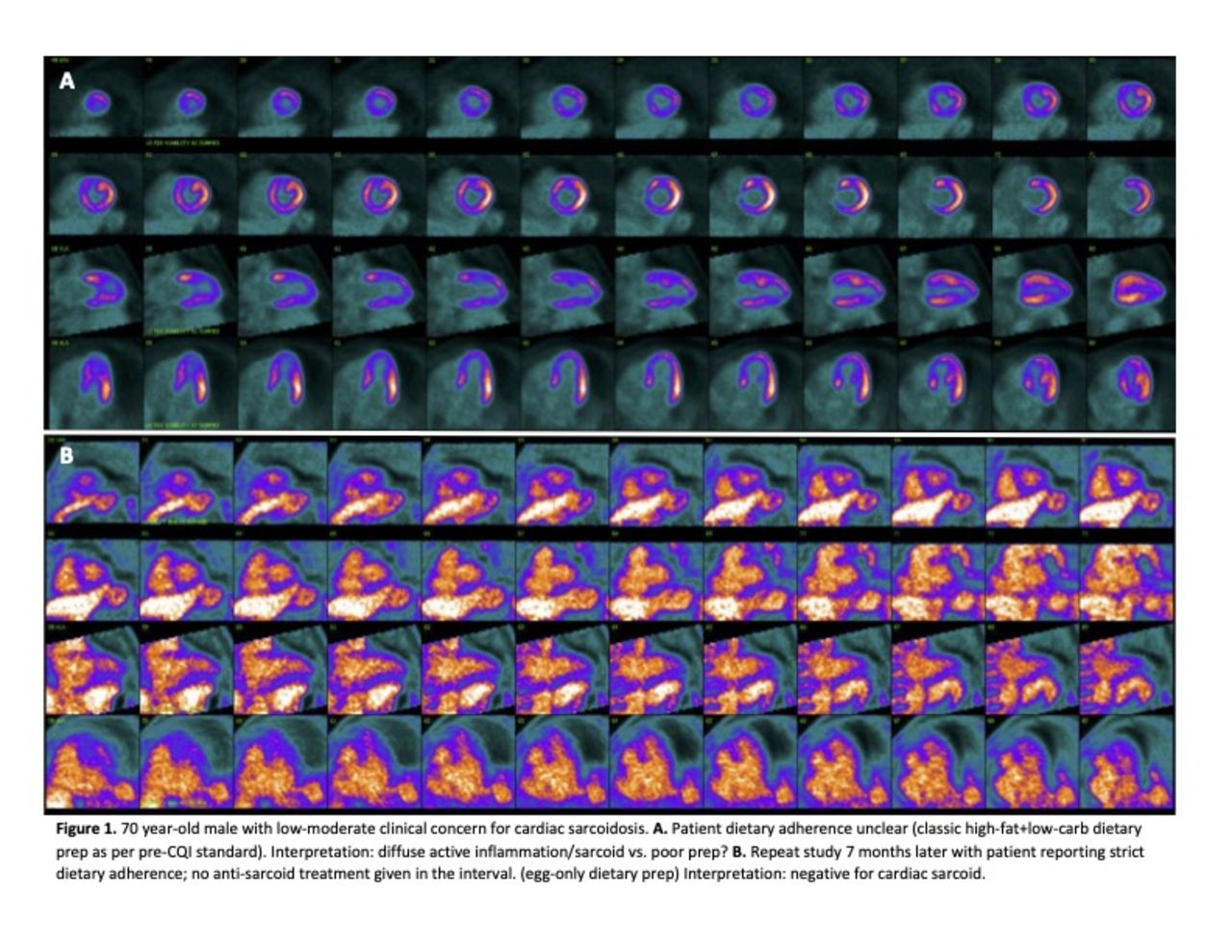
Introduction: Cardiac sarcoidosis is defined by non-caseating granulomatous inflammation of the myocardium which can cause heart failure, arrhythmias, or sudden death. 18F-FDG PET/CT has shown utility in diagnosis and monitoring as granulomas require glucose for fuel, leading to increased FDG uptake in inflamed areas. However, suppressing normal myocardial glucose uptake is required, necessitating ketosis. At our institution, the occurrence of nondiagnostic or equivocal studies was too high, often due to patient and referring clinician uncertainty related to the standard dietary prep and resulting in poor interpreter confidence. We implemented a QI initiative to improve the likelihood of obtaining quality diagnostic cardiac sarcoid PET/CT images through dietary prep modification and serum ketosis monitoring.
Methods: All patients referred for PET/CT for evaluation of known or suspected cardiac sarcoidosis as of October 1, 2023, were prepped utilizing the new protocol as described below. The new dietary protocol consisted of 3 days of eggs and cheese taken with water, black tea, or coffee only, without creamer, sugar, or sweeteners ("egg-only" diet"). This egg-only diet was followed by prolonged fasting starting at midnight in the evening prior to the imaging test. A 48-hour water-only fast was specified for patients with an egg allergy. Serum beta-hydroxybutyrate (BHB) was used as a biomarker for ketosis; all patients were asked to undergo BHB testing at least 1 day prior to the study ("D-1 BHB") and on the morning of the study ("D0 BHB"). Imaging of patients with D-1 BHB levels <0.5 mmol·L−1 was postponed at least 24 hrs, with additional dietary prep. For inpatients, a sarcoid diet order-set was developed for the EMR and training was provided to the nutritional services team.
No changes were made to the standard clinical protocol for cardiac sarcoid PET/CT imaging in our department. Imaging was acquired in 2D mode with ECG-gating over 25 minutes on a GE Discovery PET/CT scanner and consisted of a rest Rb-82 myocardial perfusion study followed by F-18 FDG metabolic imaging of the heart.
Results: Thus far, 25 patients (10 inpatients, 15 outpatients) have been imaged after being prepped with the new diet, the majority (23/25) via the egg-only diet. We were able to obtain D-1 BHB labs in 11/25 patients, which facilitated rescheduling of some patients to achieve better ketosis through prolonged dietary prep. Serum D-1 BHB was drawn in 17/25 and was used clinically to support reader confidence in interpretation. In addition, we have collaborated successfully to create a new order set for the diet in the EMR, and a script for schedulers to use with outpatients that includes information about the diet and labs. Lastly, referring and interpreting physicians have expressed high satisfaction with image quality and interpretability.
Conclusions: This QI project arose from a need to improve the dietary prep compliance and image quality in patients presenting for cardiac sarcoid assessment with PET/CT. A classic high fat-low carbohydrate diet had resulted in an unacceptably high frequency of poor or uncertain ketosis and frequent confusion on the part of patients and ordering clinicians. Our multidisciplinary team was able to institute a simple dietary prep which has, thus far, proven to be tolerated by most patients and straightforward for clinicians. The use of BHB testing has allowed us to provide an early assessment of patient ketosis in a timeframe that allows for rescheduling when needed and has helped interpreting physicians have more confidence in image interpretation. Many of our challenges with this new workflow were related to obtaining timely D-1 BHB results in outpatients and we recognize the need for a simple ketogenic alternative for patients with egg allergies or strong egg aversions who cannot tolerate a prolonged (48 hr) fast; these will likely be the focus of our near-term adjustments to this new protocol.


In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.