


Visual Abstract
Abstract
We aimed to conduct a systematic review and metaanalysis of studies reporting the performance of radioactive iodine (131I) therapy in differentiated thyroid cancer (DTC) patients requiring a completion treatment after lobectomy. We also evaluated the response to 131I therapy according to 2015 American Thyroid Association guidelines and the adverse events. Methods: A specific search strategy was designed to find articles evaluating the use of 131I in patients with evidence of DTC after lobectomy. PubMed, Cochrane Central Register of Controlled Trials, Scopus, and Web of Science were searched. The search was updated until January 2020, without language restriction. Data were cross-checked and any discrepancy discussed. A proportion metaanalysis (with 95% confidence interval) was performed using the random-effects model. Metaregressions on 131I success were attempted. Results: The pooled success ablation rate was 69%, with better results in patients receiving a single administration of about 3.7 GBq; high heterogeneity was found (I2 test, 85%), and publication bias was absent (Egger test, P = 0.57). Incomplete structural responses were recorded in only 14 of 695 (2%) patients enrolled in our analysis. Incomplete biochemical responses were observed in 8%–24% of patients, with higher rates (24%) in patients receiving low radioiodine activities (∼1.1 GBq) and lower rates (8%–18%) in patients receiving higher activities of radioiodine (∼3.7 GBq). Neck pain due to thyroiditis was reported in up to 18% of patients, but in most cases, symptoms resolved after oral paracetamol or a short course of prednisone. Conclusion: Lobar ablation with 131I is effective, especially when high 131I activities are used. However, the rate of incomplete biochemical response to initial treatment appears to be slightly higher than in the classic scheme of initial treatment of DTC. Radioisotopic lobectomy should be considered for patients with low- to intermediate-risk DTC requiring completion treatment after lobectomy due to specific individual risk factors or patient preferences.
A more conservative approach to the clinical management of thyroid nodules and differentiated thyroid cancer (DTC) has recently been proposed by the 2015 American Thyroid Association guidelines (1). Indeed, fine-needle aspiration biopsy has been selectively proposed for nodules at higher risk on the basis of ultrasound features or dimensions. In addition, lobectomy, rather than thyroidectomy, has been proposed as the initial surgical procedure in most patients affected by low-risk DTC (1). Although lobectomy mostly avoids surgery-related complications (i.e., hypoparathyroidism and laryngeal nerve dysfunction), completion thyroidectomy may be required to provide complete resection of multicentric disease or in the case of unexpected extrathyroidal extension or lymph node involvement. The clinical outcome is similar in patients treated with total thyroidectomy and lobectomy followed by completion thyroidectomy (2). However, the risk of transient (9%) or persistent hypocalcemia (1.5%) and transient vocal cord paresis (5%) is not negligible, especially if the second thyroid surgery is performed within 90 d after lobectomy (3). In addition, this 2-stage thyroidectomy is not well accepted and is often refused by patients for whom total thyroidectomy should have been initially recommended. In addition, a second surgical operation may be clinically contraindicated in patients with comorbidities or with evidence of complications after lobectomy.
Radioactive remnant ablation (131I therapy) has traditionally been reserved for DTC patients who have undergone total thyroidectomy, and particularly in those at risk of disease persistence or relapse after surgery. However, in the case of an unexpected diagnosis of DTC after lobectomy, ablation of the remaining lobe by means of 131I has been proposed as an alternative to a second completion surgery (1). This noninvasive approach could be an attractive alternative to a second surgery. However, the available literature is limited, and the effectiveness and safety of radioisotopic lobectomy are uncertain. In view of this problem, we planned an updated systematic review and metaanalysis of studies reporting the performance of radioactive iodine (131I) therapy in DTC patients who require a completion treatment after lobectomy. We also evaluated the response to 131I therapy according to 2015 guidelines (1) and reported adverse events.
MATERIALS AND METHODS
The systematic review was performed in accordance with the guidelines of PRISMA (Preferred Reporting Items for a Systematic Review and Metaanalysis) (Fig. 1) (4).

PRISMA flow diagram.
Search Strategy
A 4-step search strategy was adopted. First, sentinel studies were sought in PubMed. Second, keywords and MeSH (Medical Subject Headings) terms were identified in PubMed. Third, PubMed, Cochrane Central Register of Controlled Trials, Scopus, and Web of Science were searched. Fourth, we sought studies evaluating the use of 131I therapy for residual lobe ablation in patients with evidence of DTC after lobectomy in online databases (i.e., PubMed/MEDLINE, Embase, Web of Science, and Scopus). The search was updated until January 31, 2020. No language restriction was used. To identify additional studies and expand our search, the references of the articles retrieved were also screened. Important overlapping data (>25%) between several studies were excluded.
Data Extraction
The following information was extracted independently and in duplicate by 2 investigators in a piloted form: general information on the study (author, year of publication, country, study type, number of patients, and final diagnosis), 131I activity administered, and rate of successful ablation. For the extraction of data, main papers and supplementary data were searched; if data were missing, the authors were contacted via e-mail. Data were cross-checked, and any discrepancy was discussed.
Study Quality Assessment
The risk of bias of the studies included was assessed independently by 2 reviewers with regard to the following aspects: study design, patient selection, reporting, and reference standard. Risk of bias and concerns about applicability were rated as low, high, or unclear.
Statistical Analysis
A proportion metaanalysis was performed by means of a random-effects model. Pooled data were presented with 95% confidence interval. Heterogeneity among studies was assessed by means of the I2 test, with 50% or higher being regarded as high. Publication bias was assessed by means of the Egger test. Metaregressions on 131I therapy success were attempted. All analyses were performed using Prometa 3.0 (Internovi) or StatsDirect software. A P value of less than 0.05 was regarded as significant.
RESULTS
Literature Search
In total, 11 papers were found, and their titles and abstracts were analyzed; 4 were excluded because they were case series or did not analyze or mention at least one of the following issues: successful ablation rate, response to initial therapy (i.e., thyroidectomy and 131I therapy) (1), and side effects. In addition, we excluded studies in which patients had been treated with more than a single 131I administration and those in which the number of patients treated once was not inferable. Therefore, 5 articles were selected and 695 patients were finally included (5–9). The papers were published between 2002 and 2013 and had sample sizes ranging from 50 to 364 patients treated with 131I therapy for lobe ablation following a conservative surgical approach (i.e., lobectomy) and with a histologic diagnosis of DTC.
Qualitative Analysis (Systematic Review)
Three studies were retrospective and 2 prospective. Two studies were performed in India, 1 in the United States, 1 in the United Kingdom, and 1 in Switzerland. In 3 of the 5 studies, 22 patients affected by Hürthle cell carcinomas were included. The characteristics of the studies and patients and the therapeutic protocols are summarized in Tables 1 and 2. When the 1-y outcome after 131I ablation was evaluated according to the 2015 American Thyroid Association guidelines, sufficient data were inferable from 4 of the 5 studies. The results are summarized in Table 3. Side effects were reported in 3 of the 5 studies. Specifically, Randolph et al. and Bal et al. reported neck pain in 18% and 15% of patients, respectively (5,7). Giovanella et al. reported moderate neck pain in 34 of their 67 patients (50.7%) treated with 1.1 GBq and in 46 of the 69 treated with 3.7 GBq (66%) (8).
Characteristics of Included Studies
Patient Characteristics, Therapeutic Protocol, and Ablation Criteria
One-Year Response to Initial Therapy (Surgery Plus 131I) According to 2015 American Thyroid Association Guidelines (1)
Quality Assessment of the Studies
Risk of bias was assessed on the basis of 4 study characteristics; these results are reported in Table 4. In general, the risk of bias seemed to be high. Specifically, in 4 of 5 studies the patient selection and the quality of the standard of reference seemed to be suboptimal. In addition, the data in at least 3 of the 5 studies were not well described and reported.
Quality Assessment of Studies and Risk of Bias for Each Study Considered
Quantitative Analysis (Metaanalysis)
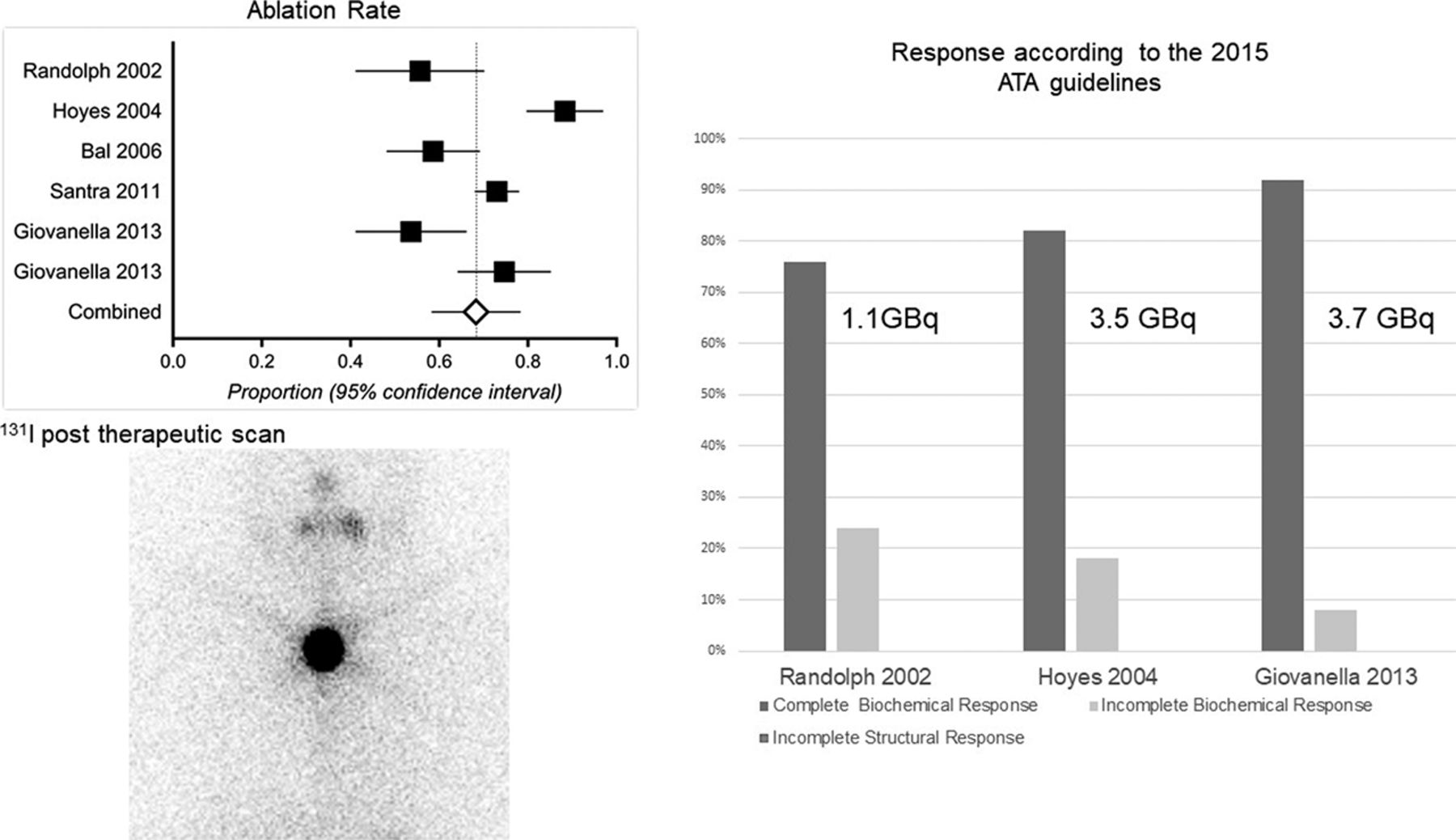
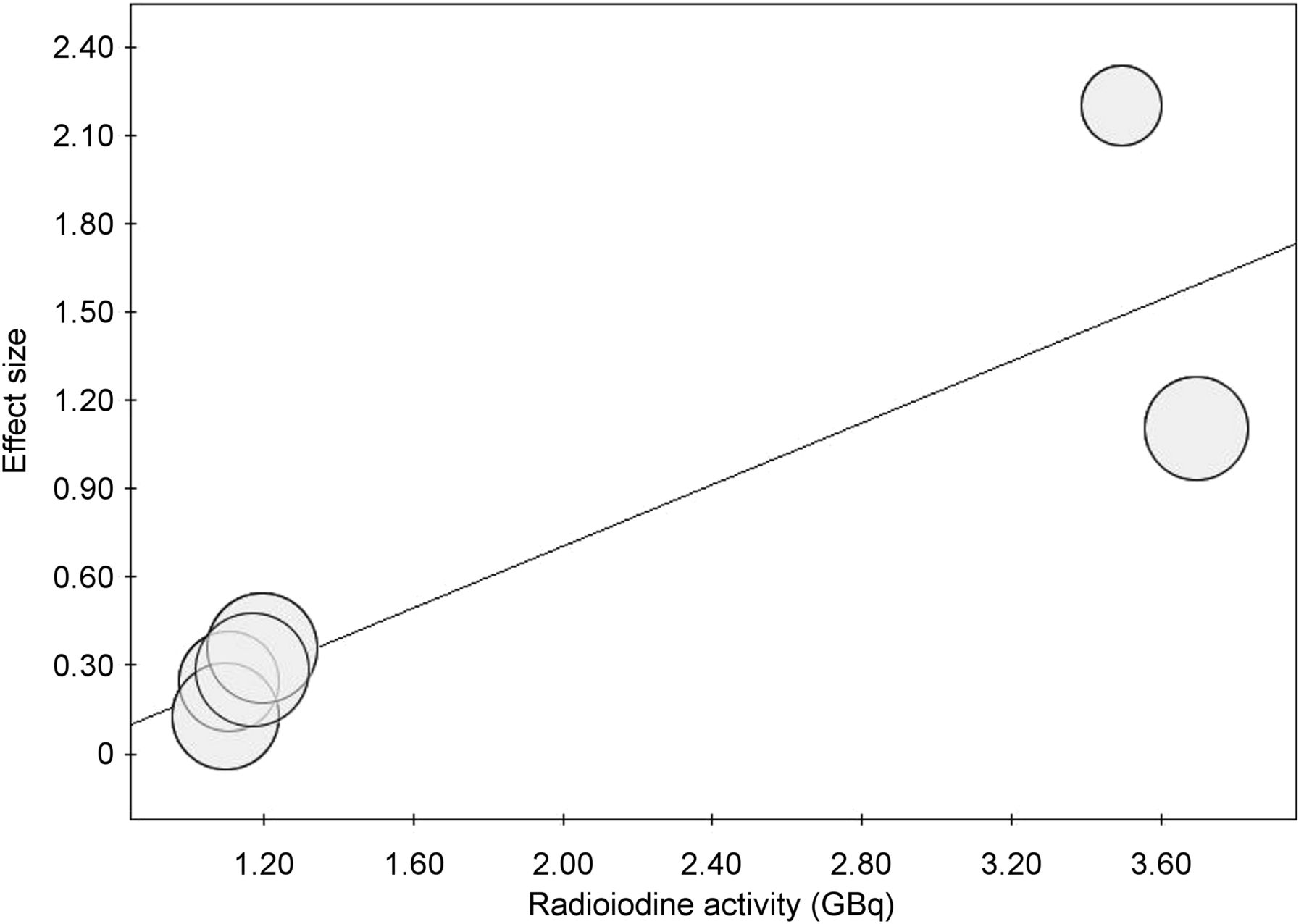
The pooled rate of successful ablation was 69% (Fig. 2); high heterogeneity was found (I2 test, 85%), and publication bias was absent (Egger test, P = 0.57). To investigate the heterogeneity found in the pooled rate of success of 131I therapy, a metaregression was performed to analyze the correlation between the 131I activity administered and the success of 131I therapy. As shown in Figure 3, the higher the 131I activity, the higher the rate of success (P = 0.02).

Proportion of rate ablation (with 95% confidence interval) of studies included in metaanalysis, with pooled result represented by diamond.

Metaregression scatterplot showing correlation between ablation rate (log) and radioiodine activity. Each circle represents study in metaanalysis, and size of circle is proportional to sample size.
DISCUSSION
The aim of this systematic review and metaanalysis was to produce evidence-based data on the reliability of 131I therapy as a noninvasive procedure to complete thyroid ablation after lobectomy in patients with DTC. Indeed, to our knowledge, this is the first high-level evidence study to focus specifically on this issue. An extensive database search was performed without time or language restrictions, and inclusion criteria were defined a priori.
Overall, 131I therapy was found to be an effective and safe strategy for completing thyroid ablation after lobectomy. As the main result, the pooled rate of successful ablation was 69%, with better results in patients receiving a single administration of about 3.7 GBq. Particularly, 131I thyroid lobe ablation, which was performed during thyroid hormone withdrawal, presented a very high rate of complete ablation, ranging from 75% to 90% when a relatively high activity of 131I (i.e., 3.5–3.7 GBq) was used. By contrast, less than 60% of patients treated with a single activity of about 1.1 GBq achieved lobe ablation.
When we applied to these studies the concept of response to initial therapy risk, as defined by the 2015 American Thyroid Association guidelines, incomplete structural responses were recorded in only 14 of 695 (2%) patients enrolled in our analysis; all of these come from a single series (8).
Incomplete biochemical responses were observed in 8%–24% of patients, with higher rates (24%) being recorded in patients receiving lower radioiodine activities (∼1.1 GBq) and lower rates (from 8%–18%) in patients receiving higher activities of radioiodine (∼3.7 GBq) (5,9); these latter rates are not far from rates reported following the conventional thyroid ablation strategy (i.e., total thyroidectomy followed by 131I ablation).
Finally, we systematically analyzed 131I therapy–related side effects on the basis of the 3 studies that reported reliable information. Overall, significant neck pain due to thyroiditis was reported in up to 18% of patients in 2 studies (2,7). Mild to moderate neck pain occurred in 50%–66% of patients in another study, depending on the activity administered: however, in most cases, symptoms resolved after oral paracetamol (500–1,000 mg) administration for a few days; in rare cases, a short course of prednisone (20–40 mg/d, tapered over 7–10 d) was needed (9). These data are encouraging, albeit limited; however, two of the studies analyzed were prospectively designed, which increased the reliability of our results.
In summary, 131I ablation after lobectomy is an effective alternative to completion thyroidectomy, especially when performed by administering activities of about 3.7 GBq, and has no or minor side effects.
Some limitations, however, should also be disclosed: first, the definition of thyroid ablation was not consistent among the studies, mostly because of the adoption of different thyroglobulin assays and cutoff points. On the other hand, applying a fixed quantitative criterion was debatable, as different assays were used, with associated differences in functional sensitivity and calibration (10). Notably, qualitative and quantitative radioiodine scanning remains the most reliable way to properly authenticate thyroid ablation, especially in the context of clinical research (11). We therefore opted for a composite qualitative criterion, adopting negative scan and thyroglobulin levels below the institutional cutoff point for a given center as the criterion for ablation.
Second, the high rate of excellent response could be related to the prevalence of low-risk DTC patients in these cases. On the other hand, a relatively high number of follicular and Hürthle cell thyroid cancers were also included.
Third, it was not possible to retrieve and analyze data on the long-term outcomes of patients. Interestingly, previously published large cohort studies found improved overall and disease-free survival after 131I lobar ablation. Using the National Cancer Database, Kiernan et al. (12) retrieved data on 32,119 of 170,330 (20%) DTC patients treated by thyroid lobectomy between 1998 and 2011. Their mean age on diagnosis was 48 y; 4% had extrathyroidal extension, 4% had positive lymph nodes, and less than 1% had distant metastases. 131I therapy was administered to 24% of patients in the thyroid lobectomy cohort and accounted for 10% of the overall 131I use. On multivariate analysis, 131I therapy use was associated with an age of less than 45 y (odds ratio, 1.51), community facilities (odds ratio, 1.26), tumors larger than 1 cm (odds ratio, 5.67), stage II or III (odds ratio, 1.54 and 2.05), positive lymph nodes (odds ratio, 1.78), and extrathyroidal extension (odds ratio, 1.36). On both univariate and multivariate analyses, 131I after lobectomy was associated with improved survival at both 5- and 10-y follow-up examinations (97% vs. 95% and 91% vs. 89%, respectively; hazard ratio, 0.53; confidence interval, 0.38–0.72 [P < 0.001]) (12).
Barbesino et al. (13) retrospectively compared 131I lobe ablation and completion thyroidectomy in a series of 134 patients affected by follicular thyroid carcinoma treated between 1983 and 2008. Thirty-seven (27.6%) had 131I lobe ablation with 1.1 GBq of 131I, 68 (50.7%) had completion thyroidectomy, and 29 (21.6%) had initial total thyroidectomy. The investigators proved that these approaches were equally effective in preparing patients for conventional 131I treatment, and whole-body scanning was associated with similar long-term outcomes (after 47–95 mo). In line with our results, Barbesino et al. found a higher rate of patients with detectable thyroglobulin (0.2–2.2 ng/mL) after 131I lobe ablation than after completion or total thyroidectomy (13).
One of the possible explanations for this difference in terms of thyroglobulin response may be related to thyroglobulin half-life, which is about 28 h (14) after total thyroidectomy, with a nadir reached in 3–4 wk (15). Vice versa, even if precise data on thyroglobulin half-life after radioiodine lobe ablation are not available, its concentration may slowly decline over the years (16).
Fourth, recommended thyroid-stimulating hormone cutoff levels to perform 131I therapy are not inferable from these studies, considering that the mean thyroid-stimulating hormone levels reported ranged from 11 to 76 μIU/mL. However, a clinical hypothyroidism related to adequate thyroid hormone withdrawal was the most frequent approach. This endogenous thyroid-stimulating hormone stimulation seems to be the most adequate preparation for 131I therapy.
Another limitation is the lack of information about the residual lobe before administering 131I. Indeed, the dimension of the lobe is an important issue, considering its influence on successful ablation. In addition, in patients with a large residual lobe, symptomatic 131I-related thyroiditis could be more frequent. One of the 5 studies evaluated the volume of residual lobe (9). Indeed, in the study by Giovanella et al. (9), one of the inclusion criteria to perform lobe ablation with 131I was a normal residual lobe (i.e., men < 12.5 cm3, women < 9 cm3) without nodules on ultrasound examination. From this point of view, we suggest careful neck ultrasonography to estimate the size of the lobe and to inform the 131I administration strategy (Fig. 4).
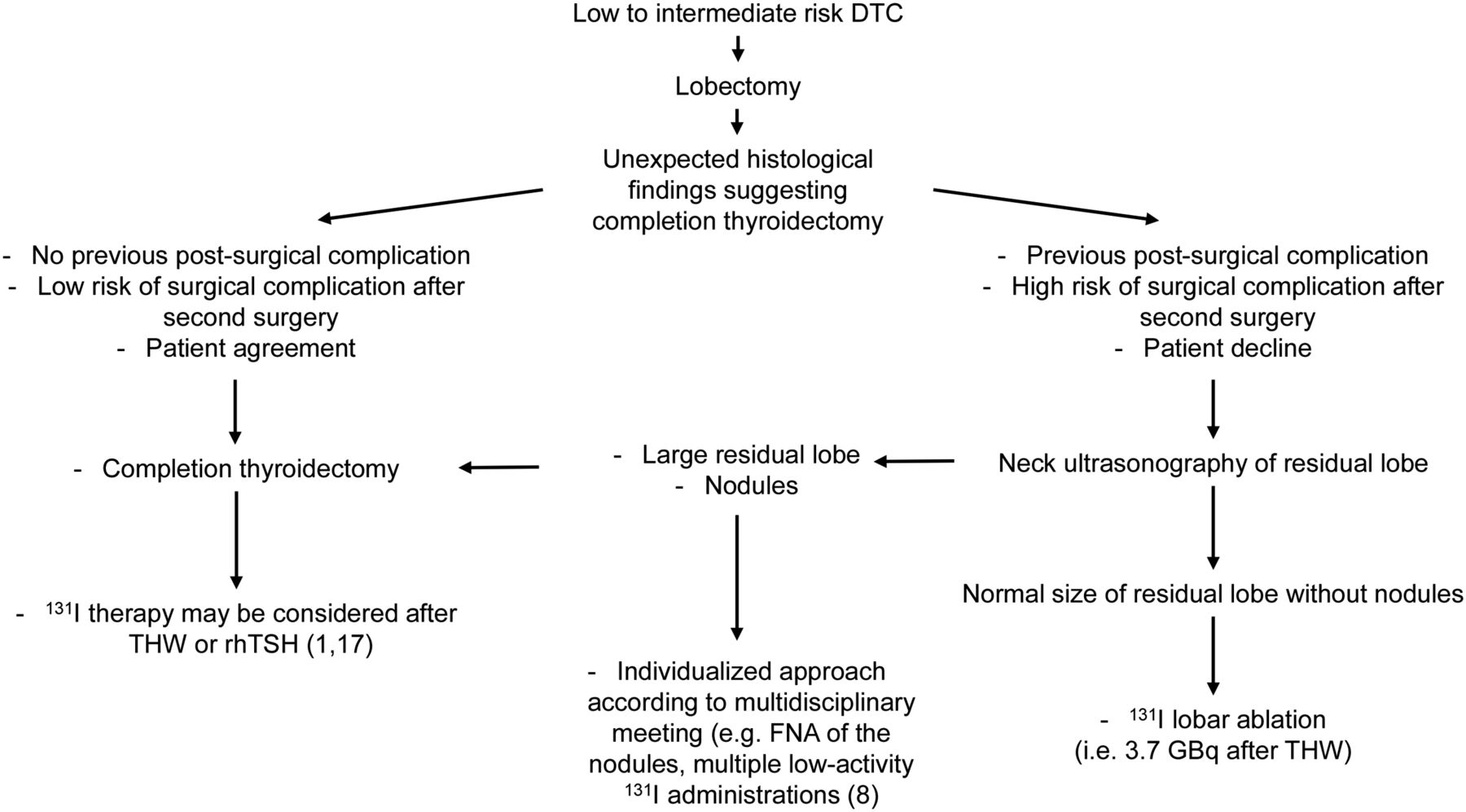
Proposed flowchart for 131I lobar ablation. FNA = fine-needle aspiration; rhTSH = recombinant human thyroid-stimulating hormone; THW = thyroid hormone withdrawal.
Finally, it is difficult to infer the clinical intent of radioisotopic lobectomy (i.e., ablation, to lower thyroglobulin levels, or adjuvant, to prevent recurrences) in the selected studies. In fact, the rigorous distinction between the ablative, adjuvant, and therapeutic aims of postoperative 131I administration was only recently introduced (1,17), making its retrospective application impossible. On the other hand, considering that an effective ablation is often associated with an excellent response to treatment and a good prognosis (1), the possibility of achieving undetectable or very low levels of thyroglobulin after 131I, even after lobectomy, could predict a good outcome identifying the patients at lower risk of disease relapse.
CONCLUSION
The need for completion thyroidectomy after lobectomy could increase in the near future because of new DTC guidelines. Thus, a noninvasive, feasible, and safe alternative to a second-step surgery is desirable. Lobar ablation with 131I is effective, especially when high 131I activities are used. However, the rate of incomplete biochemical response to initial treatment appears to be slightly higher than in the classic total thyroid ablation scheme, probably because of differences in the disappearance kinetics of thyroglobulin after 131I lobe ablation. Further prospective studies assessing the reliability of this procedure using standardized criteria for interpretation of thyroid tissue ablation are needed. Overall, radioisotopic lobectomy should be currently considered for patients with low- to intermediate-risk DTC requiring completion treatment after lobectomy due to specific individual features, risk factors, or patient preferences (1,17) who are not eligible for a second surgery or prefer to avoid an additional invasive procedure.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: is radioiodine lobectomy a feasible, effective, and safe procedure in patients with an unexpected diagnosis of intermediate- to high-risk DTC after lobectomy for an indeterminate thyroid nodule or in the case of unexpected extrathyroidal extension or lymph node metastases in patients with DTC considered, a priori, at low risk?
PERTINENT FINDINGS: Lobar ablation with 131I is effective, especially when high 131I activities are used. However, the rate of biochemical incomplete response to initial treatment seems to be slightly higher than in the classic scheme of total thyroid ablation, likely because of differences in disappearance kinetics of thyroglobulin after 131I lobar ablation.
IMPLICATIONS FOR PATIENT CARE: The need for completion thyroidectomy after lobectomy could increase in the near future because of new DTC guidelines. Then, a noninvasive, feasible, and safe alternative to a second-step surgery will be desirable.
Footnotes
↵* Contributed equally to this work.
Published online Apr. 24, 2020.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication February 29, 2020.
- Accepted for publication March 28, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.