


Abstract
In randomized clinical trials, no survival benefit has been observed for selective internal radiation therapy (SIRT) over sorafenib in patients with advanced hepatocellular carcinoma (HCC). This study aimed to assess, through a metaanalysis, whether overall survival (OS) with SIRT, as monotherapy or followed by sorafenib, is noninferior to sorafenib and to compare safety profiles for patients with advanced HCC. Methods: We searched MEDLINE, EMBASE, and the Cochrane Library up to February 2019 to identify randomized clinical trials comparing SIRT, as monotherapy or followed by sorafenib, with sorafenib monotherapy among patients with advanced HCC. The main outcomes were OS and frequency of treatment-related severe adverse events (≥grade 3). The per-protocol population was the primary analysis population. A noninferiority margin of 1.08 in terms of hazard ratio was prespecified for the upper boundary of 95% confidence interval for OS. Prespecified subgroup analyses were performed. Results: Three randomized clinical trials, involving 1,243 patients, comparing sorafenib with SIRT (SIRveNIB and SARAH) or SIRT followed by sorafenib (SORAMIC), were included. After randomization, 411 of 635 (64.7%) patients allocated to SIRT and 522 of 608 (85.8%) allocated to sorafenib completed the studies without major protocol deviations. Median OS with SIRT, whether or not followed by sorafenib, was noninferior to sorafenib (10.2 and 9.2 mo [hazard ratio, 0.91; 95% confidence interval, 0.78–1.05]). Treatment-related severe adverse events were reported in 149 of 515 patients (28.9%) who received SIRT and 249 of 575 (43.3%) who received sorafenib only (P < 0.01). Conclusion: SIRT as initial therapy for advanced HCC is noninferior to sorafenib in terms of OS and offers a better safety profile.
For patients with hepatocellular carcinoma (HCC) that is not amenable to curative therapy, transarterial chemoembolization is the recommended choice when HCC is intermediate-stage, liver-confined, and inoperable (1–6). The standard of care for patients with HCC with preserved liver function in advanced disease stages, including those with portal vein invasion, lymph node or distant metastases, or altered performance status (Barcelona Clinic Liver Cancer stage C) is systemic therapy with sorafenib (1,7). In the subset of patients with advanced HCC but no invasion at the main portal vein, lenvatinib has been shown to be noninferior to sorafenib (1,7,8).
Case series and small-scale cohort studies (9–13) suggested that the median overall survival (OS) for HCC patients receiving selective internal radiation therapy (SIRT) using 90Y microspheres was similar to the OS achieved with sorafenib (7,8). On the basis of these findings, multicenter randomized clinical trials were undertaken in Asia Pacific populations (SIRveNIB) (14) and European populations (SARAH) (15) receiving SIRT using 90Y-resin microspheres (SIR-Spheres; Sirtex) compared with sorafenib, 400 mg twice daily. In these studies, SIRT with 90Y-resin microspheres showed similar efficacy to sorafenib, with better tolerability (14,15). A further randomized trial, SORAMIC, showed no difference in OS between patients who received SIRT followed by sorafenib and those who received sorafenib monotherapy (16). However, whereas these studies did not demonstrate the superiority of SIRT (with or without subsequent sorafenib treatment) to sorafenib with respect to OS, noninferiority was not tested.
The aim of this study was to assess, through a metaanalysis of randomized clinical trials, whether SIRT with 90Y microspheres, as monotherapy or followed by sorafenib, is noninferior to sorafenib in OS of patients with advanced HCC and to compare the safety of both treatment strategies. Randomized clinical trials of SIRT followed by sorafenib, compared with sorafenib alone, were included if SIRT was the initial treatment and sorafenib therapy was given sequentially, not simultaneously.
MATERIALS AND METHODS
This metaanalysis was performed according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. The protocol for this metaanalysis is available in PROSPERO (CRD42019124372).
Data Sources and Search Strategy
Searches were conducted in 3 databases (MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials) and in the abstract books from 4 congresses (the European Society for the Study of the Liver Congress, the International Liver Congress, the American Society of Clinical Oncology Annual Congress and Gastrointestinal Symposium, and the 2018 European Society for Medical Oncology Congress) with an end date of February 14, 2019. The filter “clinical trials” was applied to the searches. No other limits were entered for the searches. The following search terms were used (search strategy for PubMed): “yttrium” (all fields) AND “sorafenib” (all fields) AND “hepatocellular carcinoma” (all fields). The Boolean operator “AND” was used to narrow the search results. In addition, we searched the clinical trial registry ClinicalTrials.gov for unpublished completed trials.
Eligibility Criteria
For inclusion in the metaanalysis, a study had to meet the following criteria: participants aged at least 18 y with histologically or radiologically diagnosed advanced HCC (imaging or biopsy); interventional arm, SIRT with 90Y-resin microspheres either as a monotherapy or followed by sorafenib; and comparator arm, sorafenib as monotherapy. The studies had to be randomized clinical trials with full information and final study results published or confirmed by the principal investigator and had to include analyses of both intention-to-treat (ITT) and per-protocol (PP) populations.
The main outcomes assessed were OS and the frequency of adverse events (AEs). An additional outcome was tumor response assessments (assessed by the Response Evaluation Criteria in Solid Tumors [RECIST 1.1]) (17).
Screening and Selection Criteria
Identified papers and congress abstracts were initially screened by title to remove duplicates and papers not fulfilling inclusion criteria and then were screened in duplicate by 2 researchers using the abstracts retrieved from congress websites and PubMed. The 2 researchers then reviewed each other’s selection. Full versions of relevant papers from the initial screening were obtained and reviewed in detail for inclusion.
Exclusions
Papers were excluded if they were reviews, did not include outcome data, were case reports or case series, or were an opinion piece or a letter. Congress abstracts were excluded if they did not add information to that obtained in the main randomized clinical trial publications, reported studies that subsequently appeared as published papers, were encore abstracts, or had insufficient information to provide useful data.
Assessment of Risk Bias in Included Studies
The 2 independent reviewers separately assessed the risk of bias of each included trial according to the recommendations from the Cochrane Handbook for Systematic Reviews of Interventions (18). Risk was assessed for allocation sequence generation; allocation concealment; masking of participants, personnel, and outcome assessors; incomplete outcome data; selective outcome reporting; for-profit bias; and other biases (Supplemental Section 1; supplemental materials are available at http://jnm.snmjournals.org (19–24)).
Trials assessed as having “low risk of bias” in all the specified individual domains were considered trials with low risk of bias. Trials assessed as having “uncertain risk of bias” or “high risk of bias” in one or more of the specified individual domains were considered as trials with high risk of bias. Disagreements were discussed, and the authors of the study were contacted, until consensus was reached. Further details of the risk of bias assessment are given in Supplemental Section 1.
Data Extraction
Using a predefined metaanalysis form, 2 reviewers, working independently, extracted data from each study. The information collected included the names of the authors, title of the study, journal in which the study was published or congress at which the study was presented, country and year of the study, treatment regimen, dosage, duration of treatment, testing sample size (with sex differentiation if applicable), number of patients receiving each regimen, and number of patients reporting treatment-related AEs. After completing the data extraction, the 2 independent reviewers compared the results. Any differences in data extraction were resolved by consensus with a third review author, referring back to the original article. The corresponding authors of the studies were contacted and agreed to contribute to the metaanalysis with individual-participant data for protocol-relevant analyses.
Data Synthesis and Analysis
Three data sets were used. The safety analysis set included all patients who received a study treatment. The PP set excluded patients with major protocol deviations, such as no or incomplete study treatment. The PP set is regarded as the preferred set for investigating noninferiority (25) and was therefore used for the primary efficacy analysis, the secondary efficacy analyses, and the subgroup analyses. However, regulatory agencies recommend analysis of both the PP and the ITT populations, and therefore, the ITT set was used in a sensitivity analysis of OS. The ITT set comprised all patients for whom data were available, and the patients were analyzed according to their randomization group. The SIRT arm comprised patients randomized to receive SIRT, whether or not followed by sorafenib, and the sorafenib arm comprised patients randomized to sorafenib treatment. The proportion of patients in each baseline characteristics category was compared between the treatment arms by a z test.
The primary endpoint of OS was tested for noninferiority. The noninferiority margin was set at 1.08 (corresponding to 60% retention of sorafenib effect vs. placebo, a value recommended in the European Society for the Study of the Liver guidelines and based on previous phase III trials of sorafenib) (7,8,26). The primary outcome of the individual trials was compared between the 2 groups using an approach that applies a fixed-effect, inverse-variance weighted log hazard ratio (HR) metaanalysis of individual-participant data.
If the 1-sided upper 95% confidence interval (CI) for this HR did not cross the noninferiority boundary of 1.08, then this result was interpreted as supporting evidence that the SIRT or the SIRT followed by sorafenib was not appreciably worse than sorafenib.
To assess whether the variation in the effects of treatment across trials was greater than might be expected, a statistical evaluation of heterogeneity by χ2 test was used. Heterogeneity was considered to be present if the χ2 test delivered a P value of less than 0.05. An I2 statistic was used to quantify the proportion of variation in the treatment effect in the study that is due to heterogeneity rather than chance. All computations and plots were performed with Stata 14.0 (StataCorp) with Leandro’s book metanalysis software (27).
Prespecified subgroup analysis included demographic characteristics, age and sex, Eastern Cooperative Oncology Group status, presence of liver cirrhosis, etiology of liver disease (hepatitis B, hepatitis C, alcohol), Child–Pugh score, Barcelona Clinic Liver Cancer stage, presence of portal vein invasion, and the absence of distant metastases.
RESULTS
Study Selection
The literature search identified 33 papers and congress abstracts, of which the reports of 3 trials—SIRveNIB (14), SARAH (15), and SORAMIC (16,28)—fulfilled the eligibility criteria and were included in the metaanalysis (Fig. 1). At the time of the literature search, 2 of the 3 eligible studies—SIRveNIB (14) and SARAH (15)—were fully published, and 1 study (SORAMIC) was presented at a congress (European Association for the Study of the Liver, in March 2018) (28). For the SORAMIC trial, the presenting author provided the preliminary proof of the article along with the raw data to allow this metaanalysis. Accordingly, the full publication of SORAMIC is cited in this paper.
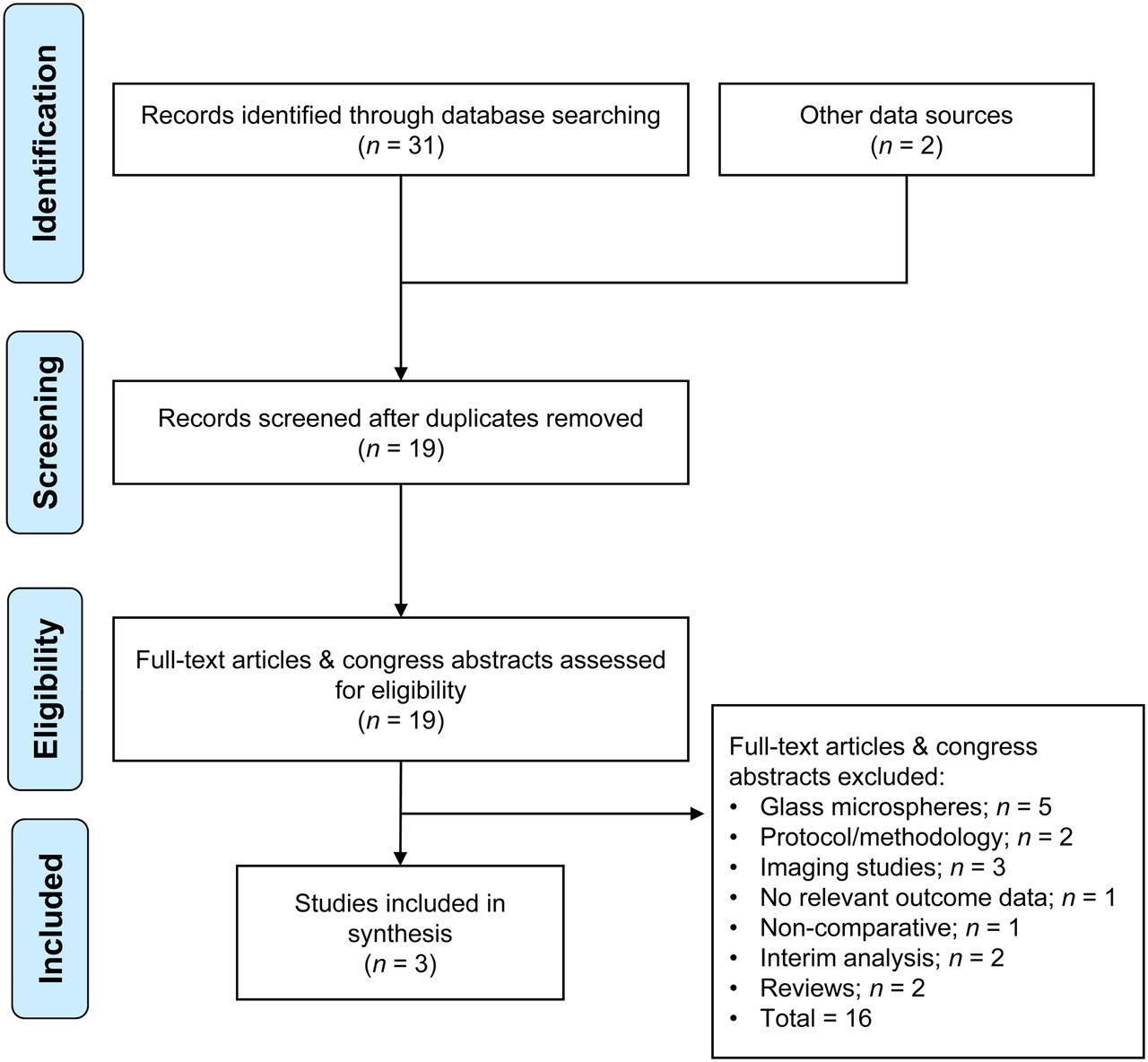
PRISMA flow diagram.
Study Characteristics
Supplemental Table 1 shows the year of study publication, study location, therapy regimens, and characteristics of each study. The trials included a total of 1,243 patients with advanced HCC, and the PP population included 933 patients (Supplemental Table 2). There were no significant differences between the studies in the proportions of patients in each category (z test for proportions).
Patient Allocation
After randomization, 23.3% and 7.1% of patients in the SIRT and sorafenib arms, respectively, did not receive the allocated treatment. The risk of not receiving the allocated treatment was higher in the SIRT arm than in the sorafenib arm (odds ratio [OR], 3.3; 95% CI, 2.5–4.4; relative risk, 1.7; 95% CI, 1.5–1.8). Reasons for not receiving the allocated treatment after randomization are shown in Supplemental Table 3.
Results of Individual Studies
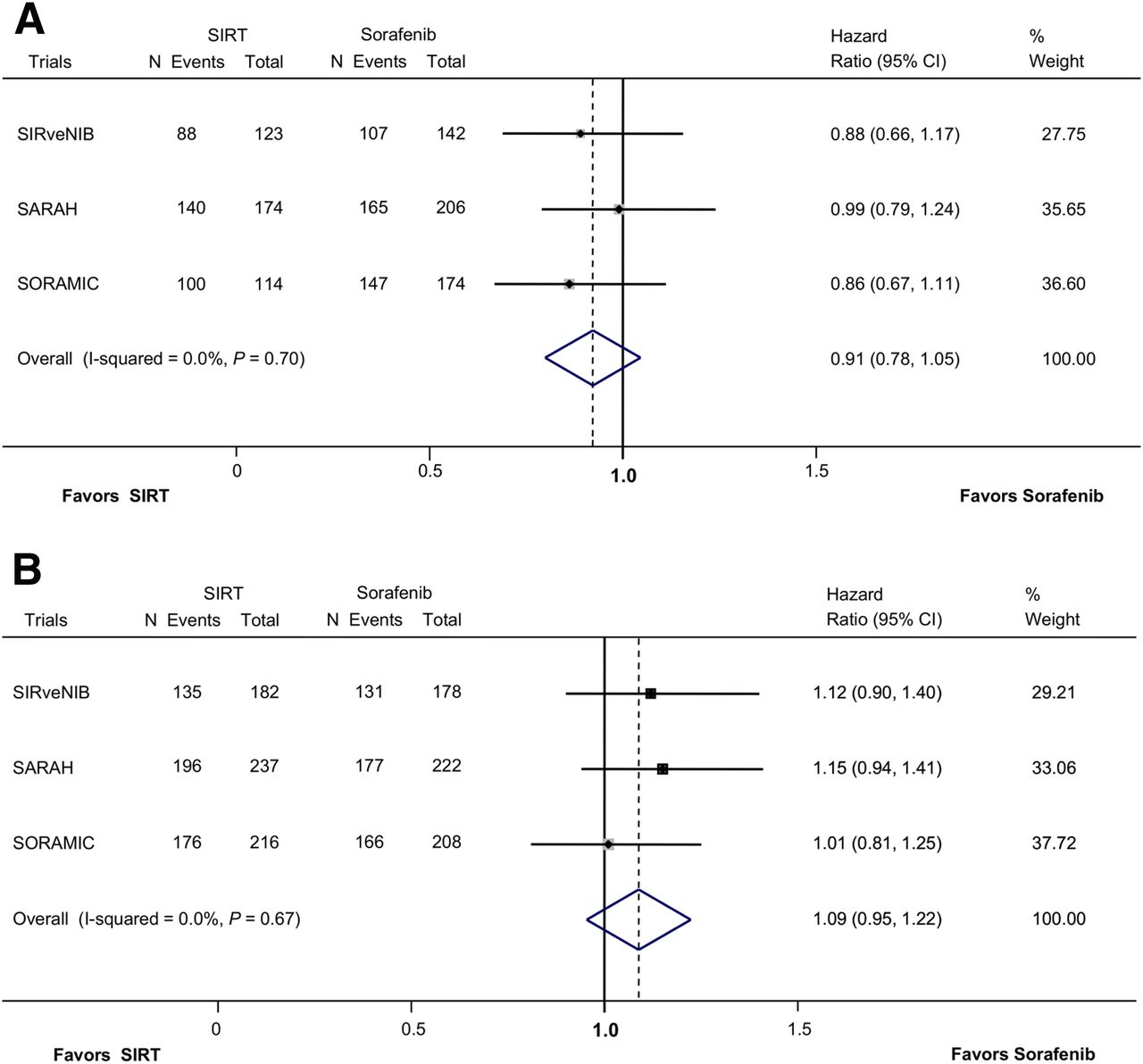
OS for the PP and ITT populations in the individual studies are shown in Figure 2. In the PP population, OS was 11.0, 9.9, and 14.0 mo in the SIRT arm versus 10.0, 9.9, and 11.1 mo in the sorafenib arm, for SIRveNIB, SARAH, and SORAMIC, respectively.

OS for SIRT vs. sorafenib in patients with HCC in individual trials and in metaanalysis of SIRveNIB, SARAH, and SORAMIC: PP population (A) and ITT population (B). Dotted line indicates overall, pooled, estimate. Size of shaded gray boxes indicates relative weight of study.
Risk of Bias Within Studies
We considered all included trials to be at a low risk of bias. A detailed analysis of the risk of bias within the studies is reported in Supplemental Section 2.
Data Synthesis
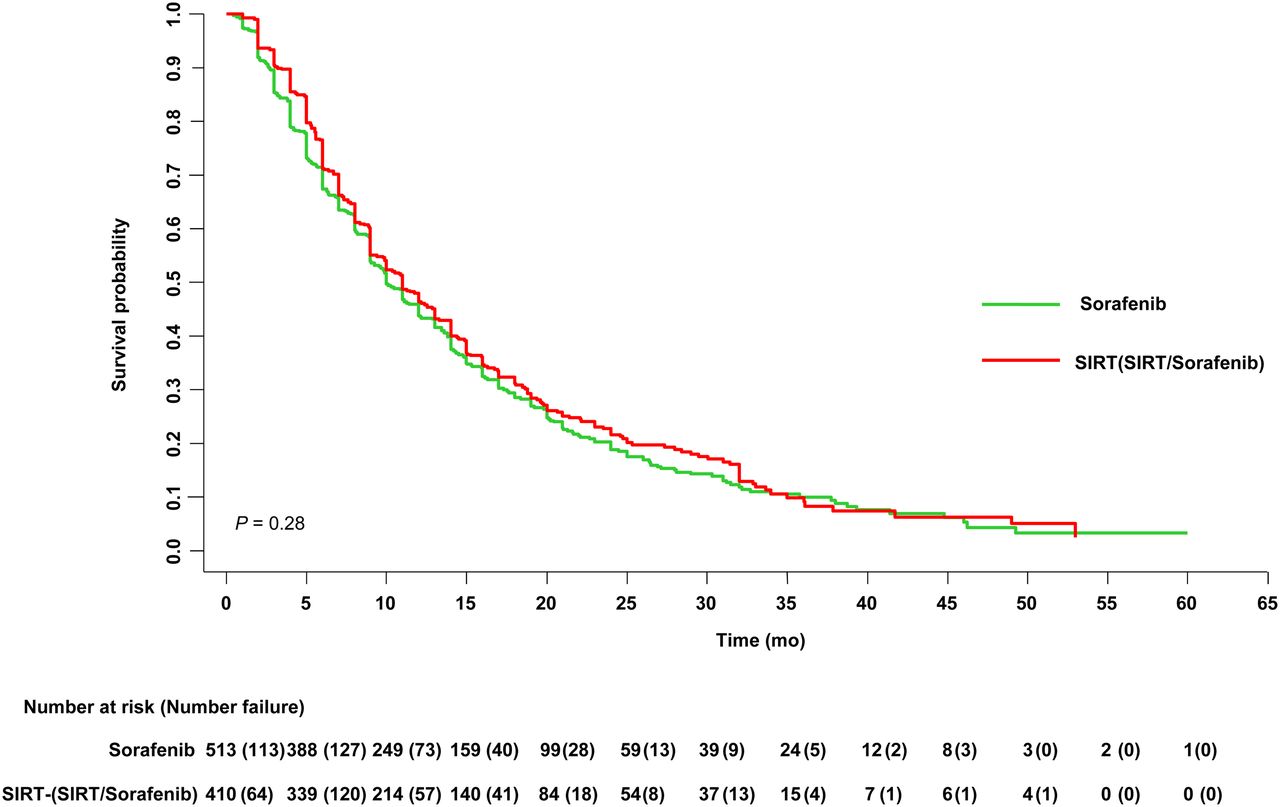
In the metaanalysis, median OS in the PP population was 10.2 mo in the SIRT arm and 9.2 mo in the sorafenib arm (pooled HR, 0.91; 95% CI, 0.78–1.05; Figs. 2 and 3). There was a high degree of similarity (nonheterogeneity) between the study populations (χ2 test for heterogeneity, 0.88; P = 0.666). The I2 statistic (variation in HR due to heterogeneity) was 0%. Analysis of OS in the ITT population also showed no significant difference between treatments (Fig. 2).
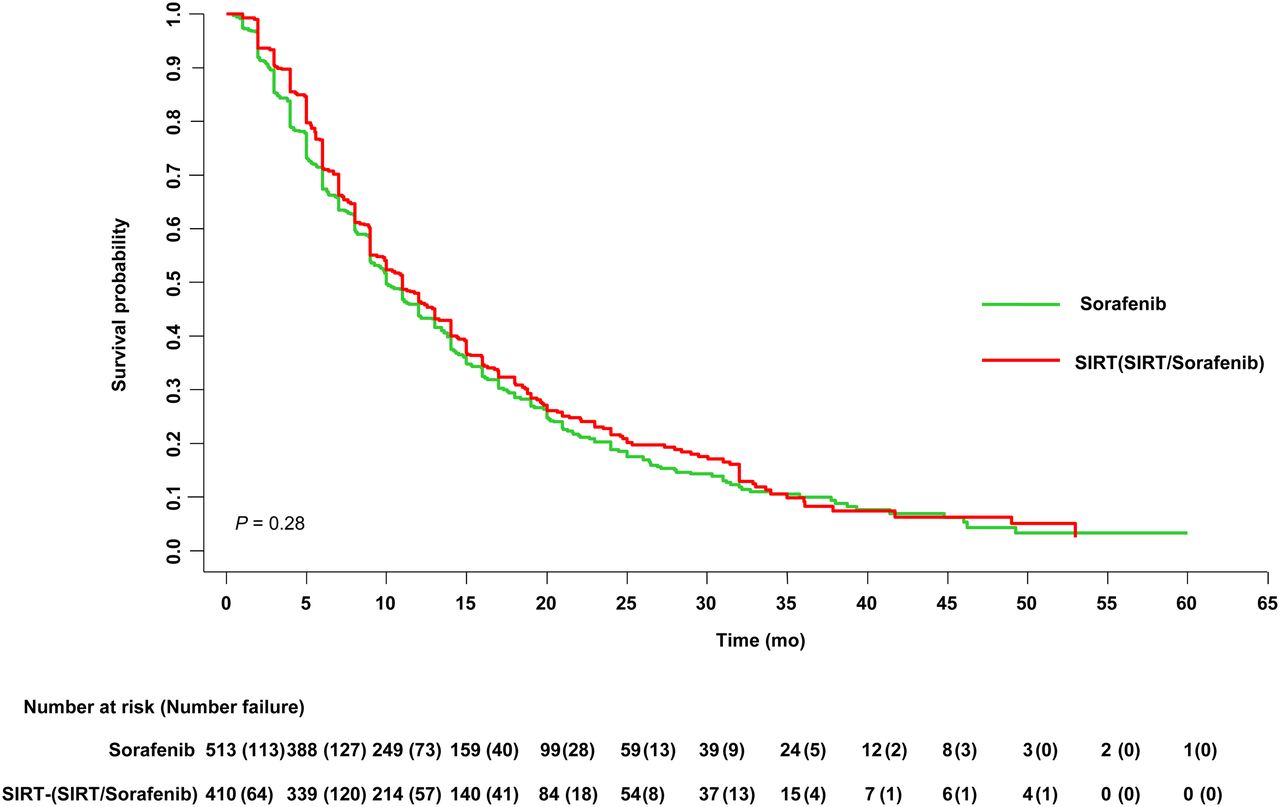
Kaplan–Meier plot of OS for SIRT, followed or not by sorafenib, vs. sorafenib monotherapy in PP population of patients with HCC.
The results of the subgroup analyses for the PP population are shown in Figure 4 and Supplemental Table 4. In all subgroups, the HR for OS was no more than 1.0 and noninferiority of SIRT to sorafenib was demonstrated in most subgroups. Superiority of SIRT to sorafenib was found in noncirrhotic patients and patients with hepatitis B (Fig. 4; Supplemental Table 4). Patients included in SIRveNIB were younger and more likely to have an Eastern Cooperative Oncology Group status of 0 and hepatitis B.

Subgroup analyses of OS for SIRT, followed or not by sorafenib, vs. sorafenib monotherapy in PP population of patients with HCC (n = 933). Dotted line indicates overall, pooled, estimate. Size of shaded gray boxes indicates relative weight of analysis. Cirrhosis data are available only for SARAH and SORAMIC. BCLC = Barcelona Clinic Liver Cancer stage; ECOG = Eastern Cooperative Oncology Group status.
Tumor response data by RECIST were not available from SORAMIC, and the combined analysis of SIRveNIB and SARAH is shown in Table 1.
Comparison of Tumor Responses (RECIST 1.1) in PP Population of SIRveNIB and SARAH Trials
The safety population included 1,090 patients with advanced HCC; 515 received SIRT and 575 received sorafenib as monotherapy (Table 2). In the SIRveNIB and SARAH trials, AEs and SAEs were more numerous in the sorafenib arms than the SIRT arms, and in SORAMIC, the addition of SIRT to sorafenib did not increase the AE rate (Table 2). The incidence of treatment-related AEs that were at least grade 3 in the SIRveNIB and SARAH trials was lower for SIRT than for sorafenib (30.6% vs. 52.1%, respectively; P = 0.0002). In SORAMIC, the incidence of treatment-related AEs that were at least grade 3 was slightly higher for SIRT, followed by sorafenib, compared with sorafenib monotherapy, without reaching statistical significance.
Treatment-Related ARs in Safety Population of SIRveNIB, SARAH, and SORAMIC Trials
DISCUSSION
Our metaanalysis included the results of 3 randomized clinical trials comparing SIRT, as monotherapy (SIRveNIB and SARAH) or followed by sorafenib (SORAMIC), with sorafenib alone. The findings indicate that initial SIRT, whether or not followed by sorafenib, is noninferior to sorafenib in terms of OS (HR, 0.91; 95% CI, 0.78–1.05) for patients in whom SIRT proved feasible. Furthermore, the safety profile of SIRT is significantly better than that of sorafenib. The better safety profile of SIRT was confirmed by the pooled analysis of the individual studies, even with the inclusion of the SORAMIC data.
Although the study design of SIRveNIB had more similarities to that of SARAH than to SORAMIC, the HR and 95% CIs for OS reported in SIRveNIB differed from those in SARAH but nearly overlapped with those in SORAMIC. The higher total bilirubin levels that were allowed for inclusion in SARAH (≤50 μmol/L), compared with SIRveNIB and SORAMIC (≤32 μmol/L), is a likely explanation for these differences.
Subgroup analyses suggested that noninferiority of SIRT, whether or not followed by sorafenib, compared with sorafenib alone was consistent across subgroups. Notably, SIRT was superior to sorafenib in terms of OS among patients with HCC etiologically linked to hepatitis B infection and those without liver cirrhosis. These populations may partially overlap because HCC arising in the absence of liver cirrhosis is mostly etiologically linked to hepatitis B infection, hepatitis C infection, or nonalcoholic fatty liver disease (29). The benefit derived from sorafenib therapy appears to be lower in patients with chronic hepatitis B virus–related HCC than in patients with HCC of other etiologies; however, no plausible causal explanation has been given for this clinically relevant observation (30,31). Unlike patients with HCC and liver cirrhosis, in which both diseases have prognostic relevance, in noncirrhotic patients the sole life-threatening disease is HCC. In the latter patient cohort, the intact liver function may allow consecutive tumor-specific systemic therapies, even in cases of rapid progression after SIRT, and this factor may account for the better OS in our analysis.
In the pooled analysis of SIRveNIB and SARAH, SIRT leads to a statistically significantly higher percentage of partial responses, whereas there was a higher percentage of stable disease in the sorafenib arm. Consequently, disease control rates did not differ between the 2 comparison groups. With respect to sorafenib, our data are in line with the results of the SHARP trial, in which it was the percentage of stable disease that mainly accounted for disease control rates whereas partial responses were exceptional and no complete responses were observed in patients receiving sorafenib.
According to current recommendations for the design, reporting, and interpretation of noninferiority trials, the data set for the full analysis, based on the ITT principle, and the data set for the PP analysis should have equal importance, and for a robust interpretation their use should lead to similar conclusions. However, in some instances a PP analysis that excludes patients who did not receive the randomized PP assignment may be preferable in a noninferiority trial (25). In the present metaanalysis, noninferiority was clearly demonstrated in the PP population but was not confirmed in the ITT population. The designs and protocols of the 3 studies included in this analysis, with the unusual comparison of a locoregional therapy with a systemic therapy, are the main reasons for this discrepancy. For example, the interval between randomization and SIRT in the included trials was 4–5 wk, as could be predicted from the study protocols, whereas patients allocated to sorafenib received the drug within 1 wk. During the 4–5 wk between randomization and SIRT, deterioration of the patient’s general condition, worsening liver function, or progression of HCC precluded a substantial proportion of patients from receiving the allocated SIRT. Furthermore, 11.5% of patients allocated to SIRT had liver-to-lung shunting or were ineligible for SIRT for technical reasons. Thus, for future trials, key prerequisites for more consistent results in the ITT and PP analyses are ascertainment of SIRT eligibility before randomization and earlier delivery of SIRT. Notably, the increased sites of production for SIR-Spheres microspheres have reduced the shipment times, resulting in earlier delivery of SIRT.
A possible drawback of a PP analysis is the low number of participants, as was the case in each of the 3 trials included in this metaanalysis. To overcome this drawback, we pooled the individual-patient data of the 3 trials to test the noninferiority of SIRT to sorafenib. However, heterogeneity between the study populations can make the results difficult to interpret. When the PP populations in the present study were combined, heterogeneity tests indicated a high degree of similarity (nonheterogeneity) among the 3 studies. In addition, a PP analysis that includes fewer participants may introduce postrandomization bias, since baseline characteristics may no longer be balanced among treatment groups. However, such was not the case in our metaanalysis, as no significant differences in baseline characteristics were found among the treatment groups of the PP population.
A limitation of this metaanalysis is that only 3 studies met the selection criteria. A strength of our metaanalysis is the inclusion of individual-patient data.
CONCLUSION
Our findings indicate that, whenever feasible, SIRT as initial therapy for advanced HCC is noninferior to sorafenib in OS and offers a better safety profile.
According to our analysis, SIRT may prove not feasible in roughly 10% of patients with advanced HCC. In these patients, systemic therapy is the standard of care. Early-phase trials exploring the efficacy and safety of combining SIRT with check-point inhibitors, modern tyrosine kinase inhibitors, and antibodies inhibiting angiogenesis are ongoing or being designed.
DISCLOSURE
Marino Venerito has received honoraria from Nordic Pharma, Merck Serono, Bayer Vital, Lilly, and Sirtex and has an advisory role with Ipsen, Lilly, Nordic Pharma, BMS, MSD, Eisai, and Amgen. Gilles Chatellier has received research funding from Sirtex. Helena Pereira has received research funding from Sirtex. Mihir Gandhi has received research funding from Sirtex Medical (Inst). Pierce Chow has received honoraria from Sirtex Medical, QuintilesIMS, Guerbet, and Merck Serono; is on the speakers’ bureau or has an advisory or consulting role with Sirtex Medical, Ipsen, Oncosil Medical, Bristol-Myers Squibb, and MSD; has received research funding from Sirtex Medical (Inst), New B Innovation (Inst), and QuintilesIMS (Inst); and has received travel or accommodation expenses from Roche. Valérie Vilgrain has received honoraria from Sirtex. Peter Malfertheiner is on the speakers’ bureau or performs consulting for Biocodex, Biohit, Danone, and Mayoly-Spindler. Jens Ricke has received research funding from, and is on the speaker’s bureau for, Bayer and Sirtex. Editorial support was received from Martin Gilmour and Tim Latham of ESP Bioscience Crowthorne, funded by Sirtex Medical. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is SIRT, as monotherapy or followed by sorafenib, noninferior to sorafenib in OS in patients with advanced HCC?
PERTINENT FINDINGS: In a noninferiority, individual-patient metaanalysis of SIRT with 90Y resin microspheres versus sorafenib in advanced HCC, we found that SIRT as initial therapy for advanced HCC was noninferior to sorafenib in terms of OS and offered a better safety profile.
IMPLICATIONS FOR PATIENT CARE: Patients eligible for first-line sorafenib treatment for advanced HCC could be offered SIRT as an effective, safer option.
Footnotes
Published online May 1, 2020.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication February 3, 2020.
- Accepted for publication March 28, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}