


Abstract
The diagnosis and subsequent therapy of neuroendocrine neoplasms (NENs) have long relied on somatostatin receptor (SSTR) expression. The field of theranostics now uses newer SSTR-based PET imaging with 68Ga-DOTATATE or 68Ga-DOTATOC as a prerequisite for the administration of peptide receptor radionuclide therapy (PRRT). In the United States, Food and Drug Administration approval of 177Lu-DOTATATE, a form of PRRT, in 2018 for use in gastroenteropancreatic NENs was obtained on the basis of prolonged progression-free survival versus high-dose octreotide long-acting release in a phase III clinical trial of well-differentiated midgut NENs. Well-differentiated grade 1 and grade 2 NENs have a low proliferation index (Ki-67 < 20%) and longer overall survival (>10 y), whereas higher-grade (grade 3 [G3]) NENs have a high Ki-67 (>20%) and shorter overall survival (<1 y). Here, we present a review on the role of SSTR-based imaging and PRRT in G3 NENs, including a discussion of well-differentiated G3 NENs, the newest histologic classification. Some studies suggest that G3 NENs are less likely to be positive on SSTR-based imaging (but more likely on 18F-FDG PET) than are well-differentiated NENs, but these data are limited. We found only 13 studies mentioning the use of PRRT in G3 NENs and a total of only 151 patients across these studies in whom radiologic response was measured. Of these 151 patients, 99 (66%) demonstrated at least stable disease or a partial response, indicating that some G3 NENs can be responsive to PRRT. We suggest that patients with G3 NENs should receive both 18F-FDG PET and SSTR-based imaging to aid in both diagnosis and treatment selection, as positivity on SSTR-based imaging helps with patient identification for PRRT and discordance may suggest important clues to tumor biology and prognosis. However, prospective studies are needed to fully understand the role of PRRT in G3 NENs, especially in well- versus poorly differentiated G3 disease.
NOTEWORTHY
The 2017 World Health Organization classification of pancreatic NENs now distinguishes between well- and poorly differentiated G3 NENs, which acknowledges biologic differences between these subgroups.
SSTR-based imaging is considered most effective in low-grade or well-differentiated NENs, and 18F-FDG PET is more likely to demonstrate disease in G3 or poorly differentiated NENs. However, for the new WHO category of well-differentiated G3 NENs, the role of SSTR-based imaging is evolving.
There is a paucity of data on PRRT in G3 NENs. In our review of the literature, we found 151 patients with G3 NENs who received PRRT and were followed to determine disease response; of these, 66% had either a partial response or stable disease.
SSTR-based imaging is a prerequisite for PRRT; we therefore recommend that patients with well-differentiated G3 NENs get both SSTR-based imaging and 18F-FDG PET.
Neuroendocrine neoplasms (NENs) are characterized by their high level of somatostatin receptor (SSTR) expression. As early as 30 y ago, imaging modalities used this special characteristic to better delineate disease burden with radiolabeled compounds bound to the SSTR analogs (1). Once SSTR expression is confirmed by SSTR-based imaging, the same SSTR analog attached to a therapeutic radioisotope can also be used to deliver molecularly targeted therapy, known as peptide receptor radionuclide therapy (PRRT) (2). Taken together, this use of therapy based on specific diagnostic imaging is known as theranostics.
Diagnostic technology has evolved for NENs from the use of 111In-octreotide to the superior 68Ga-DOTATATE or 68Ga-DOTATOC, which uses 68Ga and PET for imaging (3). The use of PRRT has also become more widespread, especially after the recent, promising results of the international phase 3 NETTER-1 clinical trial, which tested 177Lu-DOTATATE versus high-dose octreotide long-acting release in well-differentiated midgut NENs with a Ki-67 of less than 20% (4). The Food and Drug Administration recently approved 177Lu-DOTATATE PRRT in SSTR-positive gastroenteropancreatic NENs (5); however, there is a paucity of formal data regarding the role of PRRT in patients with poorly differentiated or grade 3 (G3) disease. Consequently, the effectiveness of SSTR imaging and PRRT for G3 NENs is not yet well characterized despite its Food and Drug Administration–approved indication for gastroenteropancreatic NENs of all grades. We therefore present a review of SSTR theranostics in G3 NENs, especially as it relates to histologic classification.
METHODS
We conducted separate literature reviews for SSTR imaging and PRRT. Studies for the SSTR imaging review were identified via extensive searches of 2 bibliographic databases: PubMed (includes MEDLINE) and Google Scholar. Search terms included words and phrases synonymous with neuroendocrine tumors, somatostatin, imaging, dotatate, gallium, and further searches including differentiation and grade. The searches were restricted to English-language articles only. These articles were reviewed for studies that commented on the efficacy of SSTR imaging in G3 or poorly differentiated neoplasms.
A separate search for PRRT was performed on PubMed and Google Scholar using search terms including PRRT, radionuclide therapy, neuroendocrine tumors, and grade. Searches were again restricted to English-language articles only. One hundred seventeen articles were found, of which 53 mentioned using PRRT in neuroendocrine tumor (NET) patients. Of these 53 reviewed articles, most included grade 1 (G1) and grade 2 (G2) patients or did not mention grade or tumor differentiation at all, so were not included. Thirteen total studies were included after review that documented use of PRRT in G3 patients.
HISTOLOGIC CLASSIFICATION
The nomenclature for NENs has evolved considerably since the first World Health Organization (WHO) classification in 1980 and, over time, has included classifications based on embryologic origin, cell type, and hormone secreted. In 2010, WHO released an updated grading system for gastroenteropancreatic NENs based on grade as determined by mitotic rate and Ki-67 proliferative index (6). This separates NENs into 2 broad categories depending on tumor primary site: well-differentiated NENs including G1 and G2 tumors and poorly differentiated NENs including G3 carcinomas with a Ki-67 of at least 20% (Table 1). Recent studies, however, have suggested that not all G3 NENs are the same and that these may be better classified as well-differentiated G3 NENs versus poorly differentiated G3 NENs (7,8).
2010 WHO Grading System for NENs
The 2017 WHO guidelines for pancreatic NENs formally incorporate degree of differentiation into the classification and separate G3 disease into well-differentiated G3 neuroendocrine tumors and poorly differentiated G3 neuroendocrine carcinomas (Table 2) (9). This nomenclature in the literature is sometimes abbreviated as pancreatic “NET” versus pancreatic “NEC.” This new classification was proposed for NENs outside the pancreas by a recent WHO expert consensus panel (10); however, this system is not yet formally adopted. This distinction is significant because poorly differentiated NENs carry epidemiologic, histologic and prognostic features distinct from those of well-differentiated NENs. For example, well-differentiated G1 NENs carry a median overall survival (OS) of 16.2 y, compared with only 10 mo for G3 or undifferentiated NENs (11). Even among G3 NENs, well-differentiated tumors can have significantly longer OS than poorly differentiated tumors (52.2 vs. 10.1 mo) and worse response rates to platinum-based chemotherapy (10% vs. 37%) (12). The NORDIC study found that G3 NEN patients with a Ki-67 of no more than 55% did not respond as well to platinum–etoposide and survived longer than patients with a Ki-67 of more than 55% (13). Similarly, poorly differentiated disease seems to have less expression of the SSTR, leading to less expression on SSTR-based imaging (14) and consequently less response to PRRT. There are also important differences in somatic mutational patterns between well- and poorly differentiated NENs (15).
2017 WHO Grading System for Pancreatic NENs
DIAGNOSTICS
SSTR-based PET imaging with 68Ga-DOTATATE or 68Ga-DOTATOC has demonstrated superiority to 111In-octreotide scanning (16), and its routine use has been recommended by the most recent European guidelines on G1 NENs (17) and in a recent review and publication of appropriate use criteria (18). Many studies have shown higher accuracy for SSTR PET imaging, with most reporting sensitivities between 80% and 95% (17,19–21). These recommendations focus on well- or moderately differentiated G1 and G2 NENs.
Early studies looking at SSTR imaging by tumor histology and Ki-67 have had some conflicting results, but most of these studies are limited to 111In-octreotide for imaging and include very few G3 NENs (Table 3). For example, a small study of 17 patients by Belhocine et al. (22) concluded that there was no correlation between histologic grade and 18F-FDG PET versus SSTR SPECT tracer uptake, but only 1 of 17 patients had a Ki-67 grade of more than 10% (22). Studies by Kayani et al. (19), Adams et al. (23), and Pasquali et al. (24) all suggest that SSTR imaging works well for low-grade NENs but has limited uptake in high-grade, G3, NENs compared with 18F-FDG PET. These studies, however, only had 6, 16, and 8 patients, respectively, with G3 NENs. The latter 2 studies were also conducted before the advent of SSTR PET imaging and used the older 111In-octreotide scan. 18F-FDG PET has low sensitivity in detecting G1 disease with a Ki-67 of 2% or less and, when measured, SSTR imaging demonstrates higher uptake than 18F-FDG PET consistently. There is variable uptake of SSTR imaging when Ki-67 is more than 20%, and in some studies, such as those of Adams et al. (23) and Pasquali et al. (24), Ki-67 was not explicitly mentioned.
Select Studies Reporting SSTR and 18F-FDG PET Imaging by Ki-67
Newer studies retrospectively addressing this question, like that of Binderup et al. (25), showed that 18F-FDG PET was more likely to be positive in G3 disease (13/14 patients, or 93%) versus G1 (19/47 patients, or 40%), but they did not include any SSTR-based imaging. The authors found that 18F-FDG PET had an overall sensitivity of 58% in all grades, and uptake was associated with worse OS. This use of 18F-FDG PET as an independent prognostic marker in NETs is also increasingly being studied as an adjunct to tumor grade, with additional studies showing that 18F-FDG PET positivity is a poor prognostic sign (26,27). In patients with heterogeneous metastatic lesions of different grades, high 18F-FDG PET uptake may more accurately portray specific metabolic information about every independent metastatic site than is possible with pathology from a single biopsy site, including sample error.
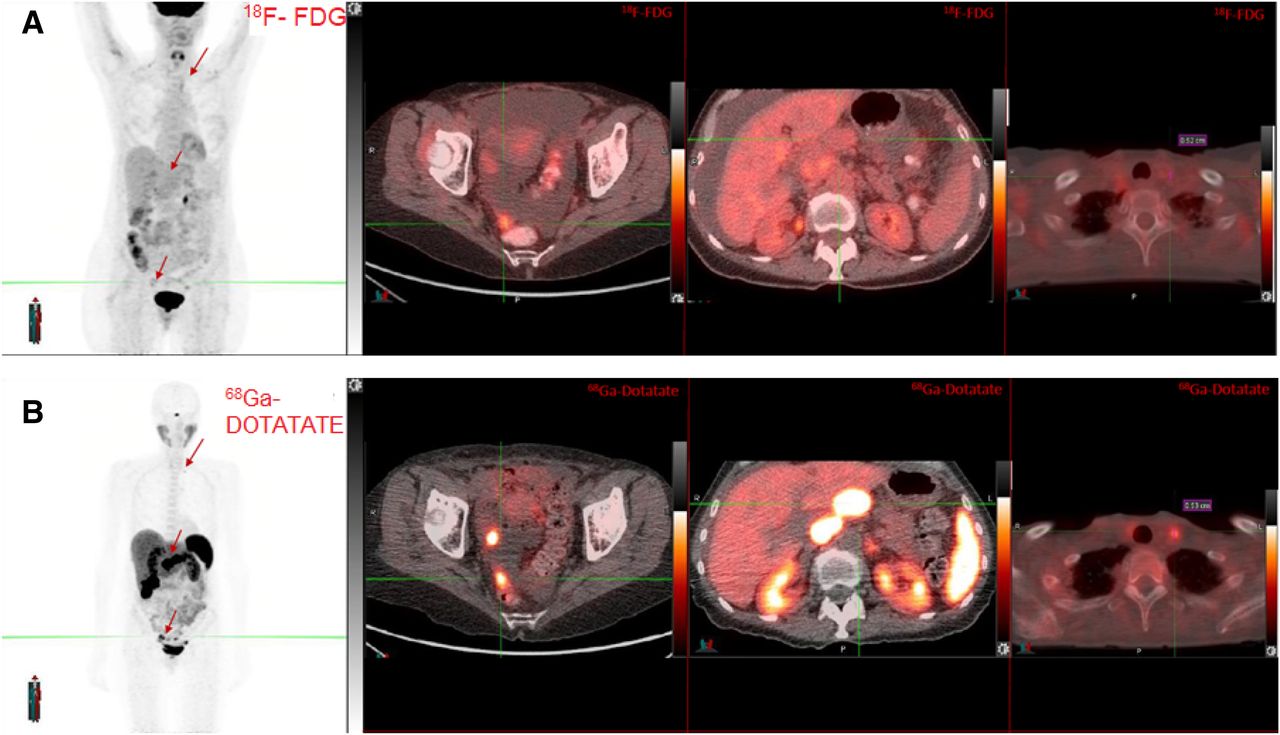
The only prospective study addressing the question of SSTR imaging versus 18F-FDG PET had 27 patients with histopathologically confirmed gastropancreatic NENs, but only 2 patients with a Ki-67 of more than 20% (28). Their results showed SSTR PET to have higher sensitivity than 18F-FDG PET regardless of tumor grade, with increased sensitivity for SSTR PET in detecting liver, bone, lymph node, and primary lesions across all grades. The concurrent use of 18F-FDG PET, however, altered therapy choices in 59% of patients in their cohort—for example, using or withholding chemotherapy or PRRT in a particular patient. Included in Figure 1 are examples of 18F-FDG PET and 68Ga-DOTATATE scans in a patient with biopsy-proven poorly differentiated, WHO G3, small cell neuroendocrine carcinoma with a mitotic index of 12 per 10 high-power fields (2 mm2) and a Ki-67 of up to 52%. The 68Ga-DOTATATE demonstrated more metastatic sites and showed more uptake in all commonly seen lesions. This patient was referred for PRRT given the positivity on the 68Ga-DOTATATE scan, with a partial response after 2 cycles before eventually having dose-limiting cytopenias and progressive disease.
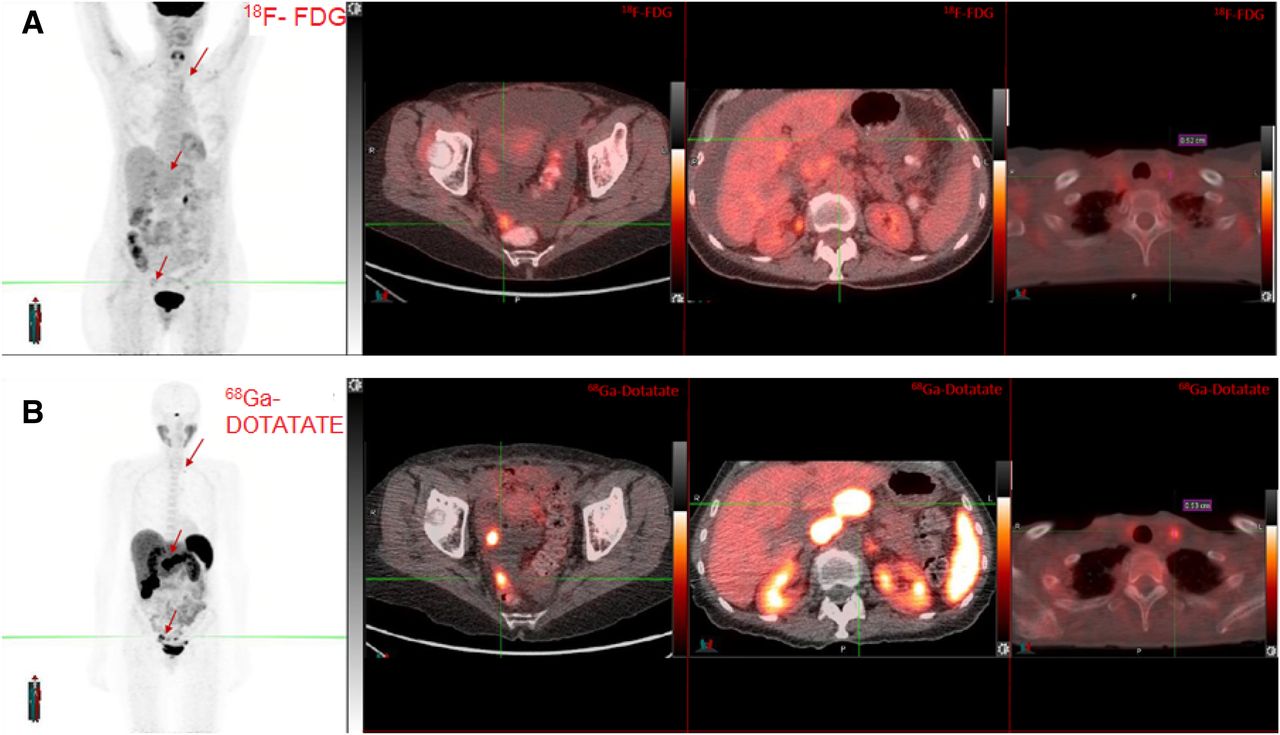
18F-FDG PET/CT (A) and 68Ga-DOTATATE PET/CT (B) in patient with G3 NEN with corresponding cross-sectional imaging.
To our knowledge, there are no large-scale retrospective or prospective studies that fully characterize the utility of SSTR PET imaging in G3 NENs. Such studies will have important therapeutic implications because positivity on SSTR imaging is a prerequisite for using PRRT.
THERAPEUTICS
Thirteen total retrospective studies were found that included any G3 or poorly differentiated NEN patients who received PRRT (Tables 4–6). Taken together, there are 183 patients overall with G3 NENs who received PRRT. No prospective trials were found.
Select Studies Reporting Survival in G3 NENs After Treatment with PRRT, 2011 and 2015
Select Studies Reporting Survival in G3 NENs After Treatment with PRRT, 2016 and 2018
Select Studies Reporting Survival in G3 NENs After Treatment with PRRT, 2017
Six of the 13 studies included in Tables 4–6 do not include outcomes of the G3 patients, and only 4 commented on the degree of differentiation. Of the 7 (7/13) studies (29–35) that directly measured the outcome of the G3 patients, there were a total of 151 patients in whom imaging studies could be tracked over time after receiving PRRT. Of these 151 patients, 99 (66%) demonstrated either stable disease, partial response, or complete response. The remaining 52 (34%) either progressed or died as best response. The results come from 7 studies with different types of PRRT, different dosages, and different times for median follow-up of CT scans. They nonetheless show that about two thirds of the pooled G3 patients have the potential to respond to PRRT.
Within these 7 studies, there is a varying level of response to the PRRT administered in a relatively small number of patients (Fig. 2). Considering the heterogeneity of the data, it is difficult to identify any specific characteristics that may predict response to PRRT in G3 NENs, given that the tumors were located in many different primary sites and the PRRT included a mix of 177Lu and 90Y in different dosages and numbers of cycles. The most successful reported studies were those by Zhang et al. (29), Nicolini et al. (30), and Thang et al. (31), in which, respectively, 49 of 69 (71%), 23 of 33 (70%), and 17 of 23 (74%) patients had either a partial response or stable disease. The study by Zhang et al. (29) reported significantly better outcomes in patients with a Ki-67 of no more than 55%, similar to the NORDIC study. The data from the study by Nicolini et al. (30) include 5 patients with a Ki-67 of between 15% and 20% and 8 patients with a Ki-67 of 20%, but the data do not track disease response from these patients apart from the other 20 patients with a Ki-67 of more than 20%. This factor may explain why the patients reported in their study had an overall better response than in some of the others in Tables 4–6. In the study by Thang et al. (31), the patients received radiosensitizing chemotherapy in cycles 2–4, which may have augmented their response. These 3 studies also seemed to have a higher median cumulative dose of 177Lu than those reported by the other studies included in Figure 2. There is unfortunately no full data reported in the study by Armaghany et al. (32), as it is only a presented abstract. The studies by Thapa et al. (33), Ezziddin et al. (34), and Yalchin et al. (35) are larger studies focused mainly on low-grade disease and included only 5, 7, and 2 patients, respectively, with a Ki-67 of more than 20%, thus making it difficult to draw any conclusions.

Comparison of responses reported in 7 studies of patients with G3 NENs treated with PRRT. PR = partial response; PD = progressive disease.
We also examined survival in the same 7 studies that measured the outcomes of G3 patients and found it to be quite varied. Zhang et al. (29), Thang et al. (31), and Armaghany et al. (32) showed median overall progression-free survival (PFS) of around 9 mo, whereas most of the other studies did not comment on PFS. Nicolini et al. (30) showed an overall median PFS of 23 mo, but as above had 13 of 33 patients with a Ki-67 of 20% or less. Katona et al. (36) did not directly report individual outcomes but showed a median PFS of only 5 mo. Zhang et al. (29), Nicolini et al. (30), and Thang et al. (31) reported median OS of 19.9, 59.9, and 19 mo, respectively. The large SEER-based study by Dasari et al. reported a median OS of 10 mo (11). In these studies, the median OS for G3 patients was even longer when stratified by Ki-67: a Ki-67 of 55% or less in Zhang et al. (29) and Thang et al. (31) had a median OS of 22 and 46 mo, respectively, and a Ki-67 of 35% or less in Nicolini et al. (30) had a median OS of 59.9 mo. This again suggests G3 NENs to be quite heterogeneous.
In the study by van Vliet et al. (37), PRRT was administered as neoadjuvant therapy before surgery, allowing for surgeries in 9 otherwise unresectable tumors, 2 of which were G3 neoplasms. Kong et al. (38), in addition to the aforementioned Thang et al. (31) study, administered PRRT in conjunction with radiosensitizing chemotherapy, with the choice of regimen based on primary site (pancreatic vs. nonpancreatic NET) (31,38). These studies show how PRRT can be used in combination therapy and perioperatively in patients with G3 NENs. However, it is premature to draw conclusions given the low numbers and lack of prospective data.
DISCUSSION
Patients with G3 NENs who are positive on SSTR-based imaging present a theranostic dilemma. Numerous studies have demonstrated the effectiveness of PRRT in well-differentiated disease where the Ki-67 is less than 20%, but it is unclear how patients with a Ki-67 of more than 20% (either well- or poorly differentiated G3 disease) would respond. It is our opinion that clinicians should perform both SSTR imaging and 18F-FDG PET when imaging G3 NENs, as this indicates which G3 patients could receive PRRT. In the future, highly detectable disease on SSTR-based imaging for G3 NENs could impact first-line therapeutic decisions as these patients should respond more favorably to PRRT. Additionally, having both studies would elucidate whether there is concordance between lesions seen on 18F-FDG PET and on SSTR-based imaging or whether there are metabolically active lesions on 18F-FDG PET that do no express the SSTR. High levels of discordance or a discordant level of progression on 18F-FDG PET again suggests a worse response to PRRT and would necessitate a switch to chemotherapy, as was shown in 5 patients in the Thang et al. study (31). The retrospective data we present regarding PRRT in G3 NENs suggest that PRRT can be effective in select patients; however, without data on tumor biology and radiographic information, it is difficult to tell which of these patients derive the most benefit. We acknowledge the lack of high-quality data for both SSTR-based imaging and PRRT in G3 NENs.
There is a need for further, large-scale prospective trials in G3 NENs receiving PRRT with respect to not only tumor grade but also degree of differentiation. As outlined in the new WHO diagnostic classifications in pancreatic NENs, degree of differentiation may be a more reliable method of understanding tumor biology and prognosis. We hypothesize that response to PRRT in G3 NENs will also hinge on degree of differentiation, with well-differentiated G3 NENs showing favorable responses, similar to lower-grade tumors.
Strong 18F-FDG PET uptake may also be used in conjunction with degree of differentiation as a predictor of response to PRRT and as a prognostic factor. High uptake seems to correlate with a poorly differentiated tumor that presumably would not respond as well to PRRT as to chemotherapy. In these cases, however, there may be a role for a combination of PRRT and radiosensitizing chemotherapy as demonstrated in the retrospective review by Thang et al. (31). Additionally, further studies can identify which radiopharmaceuticals and doses of PRRT could be effective in G3 disease, as well as identify if there are any differences based on tumor primary site.
CONCLUSION
PRRT is an important new therapeutic option, and 68Ga-DOTATATE and 68Ga-DOTATOC are important new diagnostic advances for patients with NENs that take advantage of an SSTR, the perfect target. In the field of NEN theranostics, careful consideration of SSTR-based imaging and development of prospective clinical trials will help define the role of PRRT for patients with G3 NENs.
DISCLOSURE
Carina Mari Aparici is on the Advisory Board for Ipsen. Pamela Kunz is on the Advisory Boards for Advanced Accelerator Applications, Ipsen, Lexicon, and Novartis. Research funding to the institution was received from Advanced Accelerator Applications, Genentech, Incyte, Lexicon, Merck, and Xencor. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Mar. 8, 2019.
- © 2019 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication October 29, 2018.
- Accepted for publication March 4, 2019.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.