


Abstract
The aim of this research study was to determine the role of 18F-sodium fluoride (18F-NaF) PET/CT imaging in the assessment of physiologic molecular calcification in the intracranial structures. We also examined the association of 18F-NaF accumulation with age as well as Hounsfield unit (HU) in certain anatomic sites that are known to calcify with normal aging. Methods: A total of 78 healthy subjects from the Cardiovascular Molecular Calcification Assessed by 18F-NaF PET/CT (CAMONA) clinical trial (38 women and 40 men) were included in this retrospective study. The mean age was 45.28 ± 14.15 y (age range, 21–75 y). SUVmean was used to measure 18F-NaF accumulation in the choroid plexus and epithalamus (pineal gland and habenula). Maximum HU was also measured for each region of interest. Correlation analysis was conducted to assess the association between parameters. Results: Mean SUVmean was 0.42 ± 0.26 in the right choroid plexus, 0.39 ± 25 in the left choroid plexus, and 0.23 ± 0.08 in the epithalamus. Significant positive correlations were present between 18F-NaF uptake and age in the right choroid plexus (r = 0.61, P < 0.0001), left choroid plexus (r = 0.63, P < 0.0001), and epithalamus (r = 0.36, P = 0.001). 18F-NaF uptake significantly correlated with HU in the right choroid plexus (r = 0.52, P < 0.0001), left choroid plexus (r = 0.57, P < 0.0001), and epithalamus (r = 0.25, P = 0.03). Conclusion: 18F-NaF could be used in the assessment of physiologic calcification in several intracranial structures. We report significant associations between 18F-NaF uptake and aging as well as HU in the calcified choroid plexus and epithalamus. Our findings further support the growing interest to use 18F-NaF for detecting extraosseous, molecular calcification, and this powerful probe has potential applications in the evaluation of various age-related, neurodegenerative brain processes.
Sodium fluoride labeled with 18F (18F-NaF) was first used as a molecular imaging probe in 1962 by Blau et al. (1) and was approved by the U.S Food and Drug Administration in 1972 for routine assessment of osseous disorders including metastasis from various malignancies. 18F-labeled NaF gained a great deal of popularity as an excellent bone-seeking agent due to its high skeletal uptake and rapid blood clearance from the circulation after its intravenous administration. However, due to lack of appropriate imaging instruments (PET), efforts were made to synthesize compounds that could be used with conventional nuclear medicine techniques. Therefore, routine use of 18F-NaF declined since conventional γ-cameras were unable to detect the high-energy positron annihilation after 18F decay. The introduction of modern PET scanners and the increased availability of 18F-NaF have resulted in a renewed interest in this tracer. Its sensitivity in detecting benign and malignant osseous disorders is significantly higher than that of 99mTc-labeled phosphates (2–4).
Extraosseous accumulation of 18F-NaF as a marker of soft-tissue calcification has been reported in many settings (5,6). 18F-NaF uptake in the arterial wall of arteries such as the aorta and carotid and coronary arteries indicates an active calcifying atherosclerotic plaque (7–9). 18F-NaF is also taken up in the extraosseous microscopic calcification, dystrophic calcification, and calcified metastatic lesions (10–13).
Intracranial calcification is a common neuroimaging finding in otherwise asymptomatic, normal individuals or in patients with a wide range of underlying maladies such as neurologic, metabolic, infectious, hemorrhagic, neoplastic, or other disorders (14). Choroid plexus calcification is very common finding, usually in the atrial portions of the lateral ventricles. Pineal region calcification is known to be present histologically from fetal life to adulthood. Idiopathic intracranial calcification is defined as the deposition of calcium within brain parenchyma in the absence of neurologic deficits or an apparent underlying pathologic cause (15). During the human life span, the choroid plexus, pineal gland, and habenula tend to accumulate physiologic calcifications.
The purpose of this study was to determine the use of 18F-NaF PET in the detection and characterization of active calcification in intracranial structures. We also investigated the possible association between 18F-NaF uptake and age as well as Hounsfield unit (HU) at the sites selected for this research project.
MATERIALS AND METHODS
18F-NaF PET/CT scans used in this retrospective study are part of the Cardiovascular Molecular Calcification Assessed by 18F-NaF PET/CT (CAMONA) protocol. CAMONA is a prospective trial and was approved by the Danish national committee on biomedical research ethics, registered at ClinicalTrials.gov (NCT01724749), and conducted from 2012 to 2016 in accordance with the Declaration of Helsinki. Details of the CAMONA study were previously published by Blomberg et al. (16).
Subject Selection
The CAMONA study included 89 healthy volunteers who were recruited from the general population by local advertisement or from the blood bank of Odense University Hospital, Denmark. Negative history of cardiovascular disease, oncologic disease, chronic inflammatory disease, autoimmune disease, immunodeficiency syndromes, alcohol abuse, illicit drug use, or any prescription medication were inclusion criteria for healthy volunteers. Active smokers and pregnant women were excluded. Adults were preselected by sex and age to ensure a balanced inclusion of men and women aged 20–29, 30–39, 40–49, 50–59, and 60 y or older.
The Framingham risk score was used to evaluate the modifiable cardiovascular risk factors, and only subjects with a score below the upper limits of the recommended levels were included: systolic blood pressure below 160 mm Hg and a diastolic blood pressure below 100 mm Hg, total serum cholesterol below 6.2 mmol/L, and glycated hemoglobin (HbA1c) below 48 mmol/L (17). Further detailed description of the healthy subjects of the CAMONA study were previously published by Blomberg et al. (18).
In the current study, 6 subjects were excluded as their scans were not available within our laboratory database. Another 5 subjects were excluded because of motion artifact that degraded image quality and prevented optimal images analysis. A total of 78 healthy subjects, 38 women and 40 men, were included; mean age was 45.28 ± 14.15 y (age range, 21–75 y) (Table 1). The Danish national committee on biomedical research ethics approved this study, and all subjects signed a written informed consent form.
Subject Demographics
Study Design
Study participants were evaluated by blood pressure measurements, blood chemistry testing, Framingham risk score, and 18F-NaF PET/CT imaging. Information regarding smoking habits, family history of cardiovascular diseases, and prescription medication were collected through questionnaires. Three blood pressure measurements were done for each patient, with an interval of 30 min while the patient rested supine. The average of last 2 systolic and diastolic measurements were recorded. Blood chemistry tests included fasting total cholesterol, serum low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, fasting serum glucose, HbA1c, serum creatinine, and the Modification Diet and Renal Disease–estimated glomerular filtration rate. SCORE percentage was calculated for each subject based on sex, age, total serum cholesterol, serum high-density lipoprotein cholesterol, systolic blood pressure, and smoking status.
18F-NaF PET/CT scans were obtained according to the previously published methodology by Blomberg et al. (19). In summary, 18F-NaF PET/CT imaging was performed on integrated PET/CT scanners (Discovery 690, VCT, RX, and STE; GE Healthcare) with comparable spatial resolutions. PET images were obtained 90 min after the intravenous administration of 2.2 MBq of 18F-NaF/kg of body weight. The acquisition time per bed position was 2.5 min. Total body PET images were acquired in 3-dimensional mode and reconstructed into coronal, transverse, and sagittal slices by an iterative reconstruction algorithm (VUE Point; GE Healthcare). Corrections were applied for attenuation, scatter, random coincidences, and scanner dead time. For attenuation correction and anatomic orientation, low-dose CT imaging (140 kV, 30–110 mA, noise index 25, 0.8 s per rotation, slice thickness 3.75 mm) was performed. Total body PET images were acquired in 3-dimensional mode and reconstructed into coronal, transverse, and sagittal planes by an iterative reconstruction algorithm (VUE Point; GE Healthcare).
Image Analysis
Osirix MD, version 9.0 (DICOM viewer and image-analysis program; Pixmeo SARL) was used for the analysis of fused PET/CT images. Three fixed-size spheric regions of interest (ROIs) (volume = 1.5 cm3, diameter = 1.42 cm) were drawn to encompass the calcified choroid plexus in the inferior horn of the lateral ventricle in each cerebral hemisphere and the epithalamus (including both the pineal gland and the habenula) (Fig. 1). SUVmean and maximum HU were measured for each ROI.
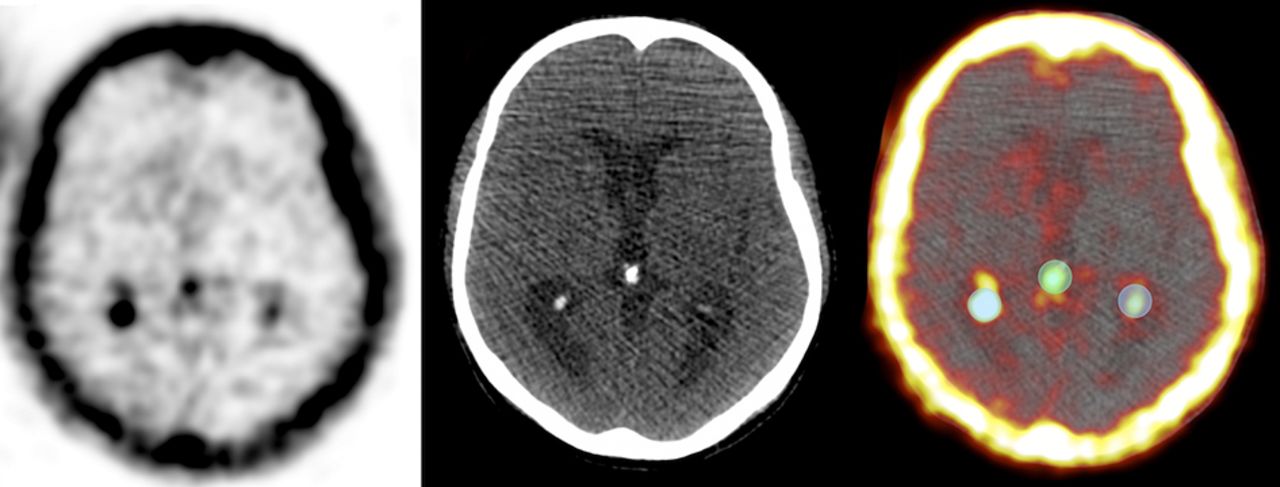
Axial PET, CT, and fused PET/CT brain images of a 59-y-old man illustrating ROIs set over calcified epithalamus and right and left choroid plexus. Mean 18F-NaF uptake and maximum HU were measured for each ROI.
Statistical Analysis
Correlation analysis by means of Pearson correlation coefficients and scatterplots was performed to investigate the relation of age with 18F-NaF uptake and maximum HU values. The association between 18F-NaF uptake and maximum HU was also investigated by correlation analysis. Exploratory multivariable linear regression was applied for all endpoints using all available demographic data (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org). Because of the limited sample size, the number of explanatory variables was reduced by application of variance inflation factor analysis first and backward variable selection (with pstay = 0.7) thereafter, but age and sex were maintained irrespectively of their P values. A 2-tailed P value below 0.05 was regarded as statistically significant. Statistical analysis was conducted using Stata/MP 15.0 (StataCorp.).
RESULTS
SUVmean was 0.42 ± 0.26 in the right choroid plexus, 0.39 ± 0.25 in the left choroid plexus, and 0.23 ± 0.08 in the epithalamus. The average of maximum HU was 148 ± 66.01 in the right choroid plexus, 141 ± 61.31 in the left choroid plexus, and 235 ± 130.69 in the epithalamus.
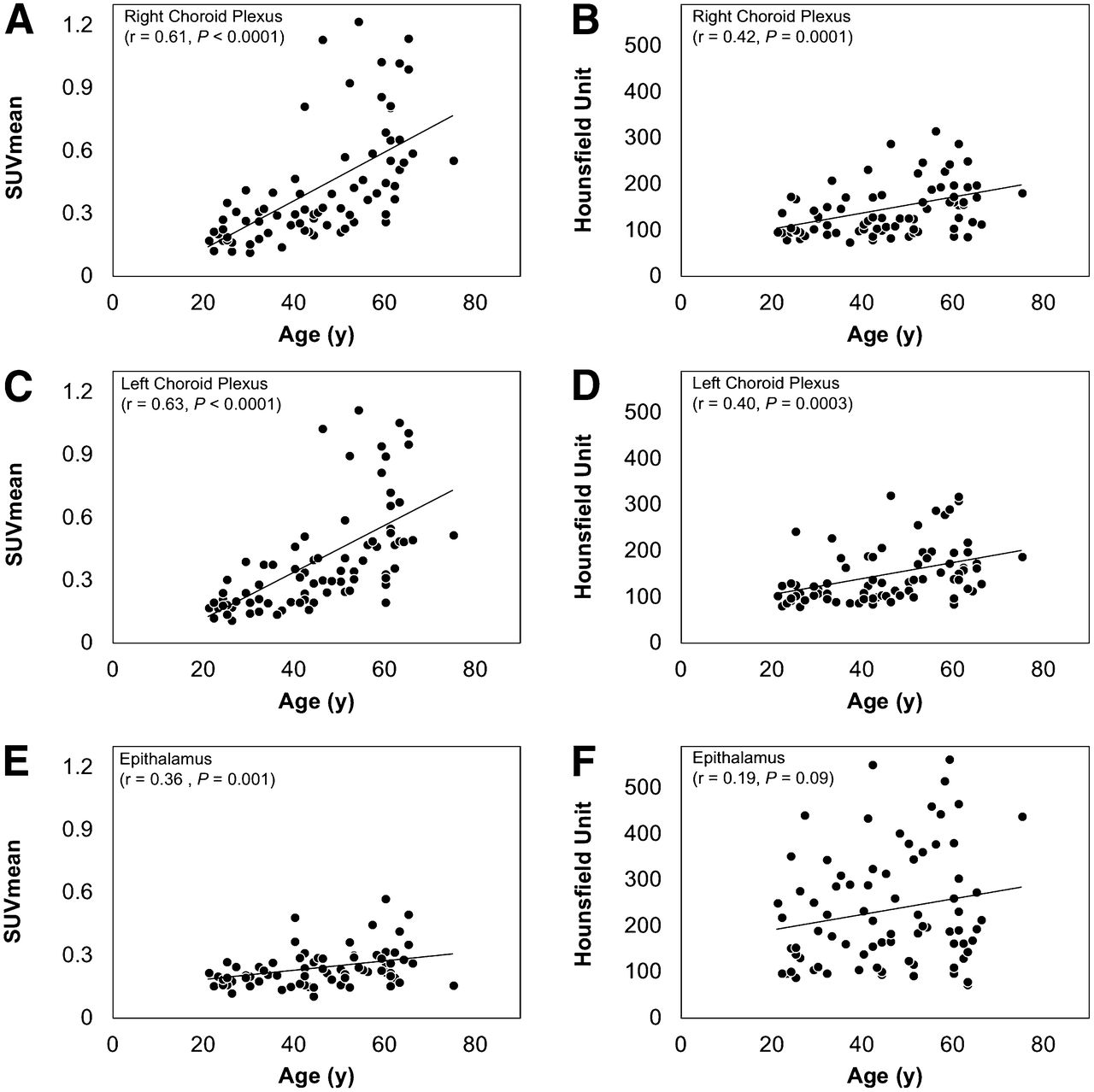
Significant positive correlations were present between 18F-NaF uptake and age in the right choroid plexus (r = 0.61, P < 0.0001), left choroid plexus (r = 0.63, P < 0.0001), and epithalamus (r = 0.36, P = 0.001). HU values also had a positive correlation with aging in both the right (r = 0.43, P = 0.0001) and the left (r = 0.40, P = 0.0003) choroid plexus, but not in the epithalamus (r = 0.19, P = 0.09) (Fig. 2). Exploratory multivariable linear regression supported the statistically significant influence of age on 18F-NaF uptake and HU values after adjustment for demographic variables (Supplemental Table 1).

Correlation of 18F-NaF uptake (A, C, E) and maximum HU (B, D, F) in choroid plexus and epithalamus with age. r = Pearson correlation coefficient.
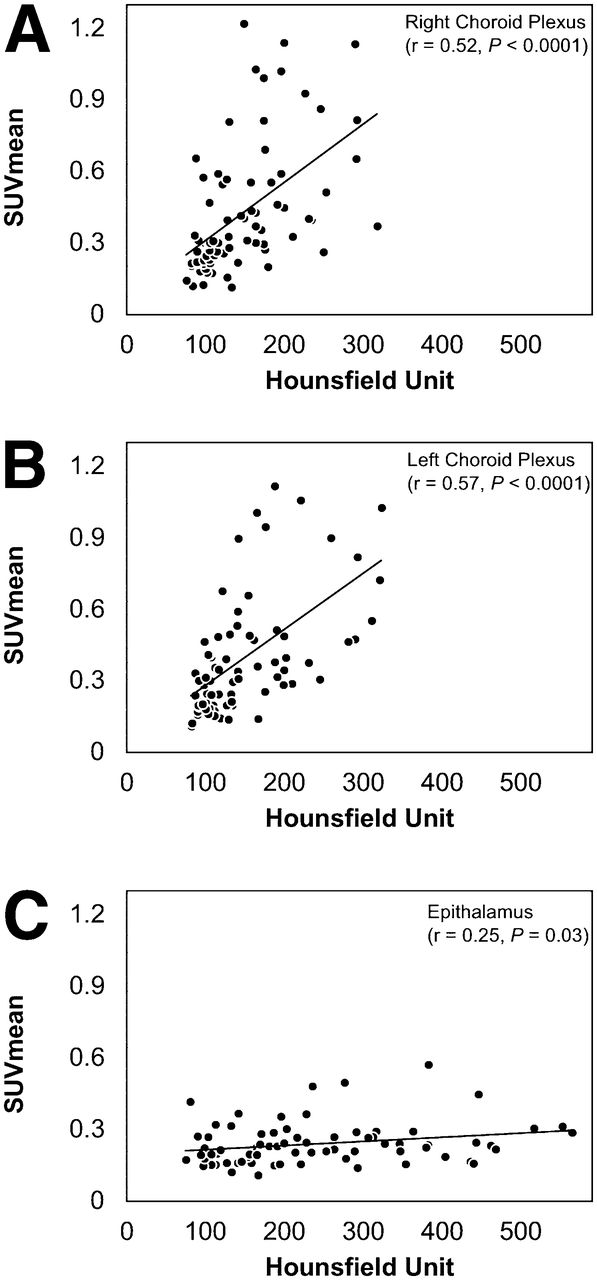
Significant positive correlations were observed between 18F-NaF uptake and HU in the right choroid plexus (r = 0.52, P < 0.0001), left choroid plexus (r = 0.57, P < 0.0001), and epithalamus (r = 0.25, P = 0.03) (Fig. 3).

Correlations of 18F-NaF uptake with HU values in right choroid plexus (A), left choroid plexus (B), and epithalamiums (C). r = Pearson correlation coefficient.
DISCUSSION
Idiopathic intracranial calcification is thought to be related to normal physiologic aging and neurodegenerative processes (20). It is most commonly found in the choroid plexus, pineal gland, habenula, and dura matter. It is present in 50%–70% of adults above the age of 30 y, and its incidence increases with age (21,22), but it is not uncommon to encounter these finding in young adolescents (23,24).
Hydroxyl-apatite (Ca10[PO4 ]6[OH]2) is a major component of calcified intracranial lesions (25,26). The 18F-fluorine ion of NaF exchanges with hydroxyl ions (OH−) on the surface of the hydroxyapatite matrix to form fluoro-apatite (27). The rate of 18F-NaF accumulation depends on the number of binding sites on the surface of hydroxyl-apatite available to react with 18F (28). Any anabolic or catabolic process that alters calcium metabolism affects the hydroxyl-apatite surface area, and thus, increases the degree of availability of binding sites, consequently resulting in higher 18F-NaF uptake (29–31).
Our results showed that 18F-NaF PET could detect and semiquantify calcium metabolism and its turnover in calcified choroid plexus and epithalamus. We also found significant positive associations between aging and 18F-NaF accumulation as well as HU values in the choroid plexus and epithalamus. 18F-NaF accumulation in the regions selected for this study had a significant positive correlation with HU values.
Kwak et al. retrospectively studied 2,877 cranial CT scans and noted a strong association between the calcification of choroid plexus and pineal gland with normal aging (32,33). Whitehead et al. examined head CT scans of 500 subjects in their first decade of life and reported a correlation between choroid plexus and pineal gland calcification with age (34).
In the population examined, calcification in the epithalamus had higher maximum HU values than those seen in the choroid plexus on CT images. However, the choroid plexus had higher 18F-NaF uptake on PET. This may indicate that calcium deposits in the pineal gland were more mature and less metabolically active than the calcification of the choroid plexus. This consolidates the role of PET as a functional imaging modality that reflects the metabolic activity of the investigated organ in contrast to other structural imaging modalities. Pathologic studies suggested that the architecture of pineal gland calcifications does not change with age (35).
Imaging studies are routinely used in the evaluation of brain calcifications and its associated disorders. Nonenhanced CT scanning is the most commonly used modality to image brain calcification; calcium deposits have a distinct hyperdense appearance on CT (36,37). Calcifications have variable signal intensity on T1-weighted and T2-weighted images. However, iron and calcium deposition in the basal ganglia both have a hypointense signal on T2-weighted images (38), making conventional MRI less reliable than CT in detecting calcifications (39). Susceptibility-weighted imaging has improved the ability of MRI in detecting brain calcification (40). The sensitivity of ultrasound for detecting intracranial calcification is highly comparable to that of CT in early childhood, but it is only feasible to perform in newborns before the closure of the fontanelles which occurs by the 18th month of age (41,42). Plain radiography is not a reliable modality to detect intracranial calcification, but extensive calcifications could be seen on radiographs as opaque lesions similar to that in the pineal gland or the falx.
Our study was limited by the imaging protocol; images were acquired 90 min after administration of 18F-NaF instead of the routine 60 min-protocol; however, these scans originate as stated from the CAMONA project, which deals with molecular arterial calcification, whereas the Society of Nuclear Medicine and Molecular Imaging guideline is for 18F-NaF PET/CT bone scans. Molecular imaging with PET to detect intracranial calcification is an important domain of research and may not replace the established methods in the near future. However, as the experience with this powerful approach becomes substantial, 18F-NaF PET may play a major role in the evaluation of the metabolic activity of calcified brain lesions.
CONCLUSION
On the basis of the scientific data that we have described in this article, 18F-NaF could be used in the assessment of physiologic calcification in several intracranial structures. We report a significant association between 18F-NaF uptake and aging as well as HU in the calcified choroid plexus and epithalamus. Our findings further support the growing interest to use 18F-NaF for detecting extraosseous, molecular calcification and this powerful probe has potential applications in the evaluation of various age-related, neurodegenerative brain calcifications.
DISCLOSURE
This study was funded by the Anna Marie and Christian Rasmussen’s Memorial Foundation, University of Southern Denmark, Odense, Denmark, and the Jørgen and Gisela Thrane’s Philanthropic Research Foundation, Broager, Denmark. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank the staff of the CAMONA study and the study participants for their valuable contributions.
Footnotes
Published online Jul. 12, 2018.
- © 2019 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication April 25, 2018.
- Accepted for publication June 18, 2018.





{kind=link}
{kind=link}
{kind=link}