


Abstract
The purpose of this study was to compare the diagnostic performance of 18F-DCFBC PET/CT, a first-generation 18F-labeled prostate-specific membrane antigen (PSMA)–targeted agent, and 18F-NaF PET/CT, a sensitive marker of osteoblastic activity, in a prospective cohort of patients with metastatic prostate cancer. Methods: Twenty-eight prostate cancer patients with metastatic disease on conventional imaging prospectively received up to 4 PET/CT scans. All patients completed baseline 18F-DCFBC PET/CT and 18F-NaF PET/CT scans, and 23 patients completed follow-up imaging, with a median follow-up interval of 5.7 mo (range, 4.2–12.6 mo). Lesion detection was compared across the 2 PET/CT agents at each time point. Detection and SUV characteristics of each PET/CT agent were compared with serum prostate-specific antigen (PSA) levels and treatment status at the time of baseline imaging using nonparametric statistical testing (Spearman correlation, Wilcoxon rank). Results: Twenty-six patients had metastatic disease detected on 18F-NaF or 18F-DCFBC at baseline, and 2 patients were negative on both scans. Three patients demonstrated soft tissue–only disease. Of 241 lesions detected at baseline, 56 were soft-tissue lesions identified by 18F-DCFBC only and 185 bone lesions detected on 18F-NaF or 18F-DCFBC. 18F-NaF detected significantly more bone lesions than 18F-DCFBC (P < 0.001). Correlation of PSA with patient-level SUV metrics was strong in 18F-DCFBC (ρ > 0.5, P < 0.01) and poor in 18F-NaF (ρ < 0.3, P > 0.1). When PSA levels were combined with treatment status, patients with below-median levels of PSA (<2 ng/mL) on androgen deprivation therapy (n = 11) demonstrated more lesions on 18F-NaF than 18F-DCFBC (P = 0.02). In PSA greater than 2 ng/mL, patients on androgen deprivation therapy (n = 8) showed equal to or more lesions on 18F-DCFBC than on 18F-NaF. Conclusion: The utility of PSMA-targeting imaging in metastatic prostate cancer appears to depend on patient disease course and treatment status. Compared with 18F-NaF PET/CT, 18F-DCFBC PET/CT detected significantly fewer bone lesions in the setting of early or metastatic castrate-sensitive disease on treatment. However, in advanced metastatic castrate-resistant prostate cancer, 18F-DCFBC PET/CT shows good concordance with NaF PET/CT.
Despite the promising decline in overall prostate cancer mortality rates in recent decades, disease-specific survival has not improved in men with metastatic prostate cancer (1). Clinical trial design is limited by the lack of predictive biomarkers, including imaging-based biomarkers, in this setting. Conventional imaging modalities such as CT, MRI, and 99mTc-methylene diphosphonate bone scintigraphy (bone scan) have shown modest, yet incomplete, prediction of treatment success (2,3).
Several molecular targets have shown promise in assessing disease burden. 18F-labeled sodium fluoride (18F-NaF) is a highly sensitive PET agent targeting bone turnover for detection of skeletal metastases (4,5). 18F-NaF PET/CT has a sensitivity superior to conventional planar bone scans, although its specificity is limited by false-positive benign bone pathologies (6). Gaining recent attention are newer radioligands targeting prostate-specific membrane antigen (PSMA), a transmembrane protein highly expressed in prostate cancer cells, which is thought to correlate with disease aggressiveness (7,8). PSMA-targeting PET agents have shown promising clinical utility in biochemically recurrent disease (9–11). Initial studies in metastatic prostate cancer show superior sensitivity compared with conventional imaging modalities and there is great hope that PSMA-targeted imaging can serve as an accurate imaging biomarker of disease burden in metastatic prostate cancer (12–14).
There are limited data on the comparative performance of PSMA-targeted imaging with 18F-NaF PET/CT, though initial case reports in advanced metastatic castrate-resistance (CRPC) suggest a diagnostic advantage of PSMA-targeted PET/CT (15,16). Here, we present a prospective pilot study comparing the detection performance of PSMA-targeted PET/CT using 18F-DCFBC, a first-generation 18F-labeled small molecule targeting the external binding domain of PSMA (12,17), with 18F-NaF PET/CT in metastatic prostate cancer patients.
MATERIALS AND METHODS
Patient Population
This single-institution prospective study was approved by the Institutional Review Board and was Health Insurance Portability and Accountability Act–compliant (NCT02190279). All patients enrolled after written informed consent was obtained. The primary objective of the multiarm study was to assess 18F-DCFBC in localized, recurrent and metastatic prostate cancer. We report findings from the metastatic population, with secondary endpoint to compare uptake of 18F-DCFBC in bone with 18F-NaF PET/CT. Eligibility required histopathologically confirmed prostate cancer and identifiable metastatic disease on conventional imaging (CT, MRI, or bone scan). All patients underwent baseline 18F-DCFBC PET/CT and 18F-NaF PET/CT scans (median interval, 7 d). Follow-up scans were obtained at a median 5.7 mo (range, 4.2–12.6 mo) after baseline imaging. There was no exclusion criteria regarding prior or ongoing therapies. Castration status, all prior treatment history, diagnostic history, and current treatments were established on the basis of clinical review of patient medical records. Prostate-specific antigen (PSA) levels were obtained at baseline and at the time of follow-up imaging. Interval treatments occurring between baseline and follow-up imaging time points were documented. Change in PSA during treatment was evaluated by PSA fold change, defined as the ratio of follow-up PSA to baseline PSA.
PET/CT Acquisition
18F-DCFBC was produced on a FASTlab synthesizer according to good-manufacturing-practice procedures, as described previously (17,18). Patients received 18F-DCFBC administered as an intravenous bolus (range, 277–296 MBq) followed by static whole-body PET/CT performed at 60 min (range, 52–66 min) and 120 min (range, 107–141 min) after injection. 18F-NaF was commercially obtained (Cardinal Health). A single, static whole-body 18F-NaF PET/CT scan was obtained 60 min (range, 50–81 min) after intravenous bolus of radiotracer (range, 99–137 MBq). All imaging was performed on a Gemini TF system (Philips Healthcare). Low-dose CT transmission scans were obtained (120 kVp, 60 mAs, 0.75-s rotation time, 1.438 pitch, axial slice thickness of 5 mm) for attenuation correction and localization. Emission PET images were obtained at 2 min/bed position with 22 slices in bed overlap. The PET images were reconstructed using the Gemini TF’s (19) default reconstruction algorithm (BLOB-OS-TF, a 3-dimensional ordered subset iterative time-of-flight reconstruction technique using 3 iterations, 33 subsets, and a voxel size of 4 × 4 × 4 mm). SUVs were calculated as the ratio of measured activity to injected dose per kilogram of patient’s body weight.
PET/CT Analysis
Imaging review and analysis was performed using commercial software (MIM). Three nuclear medicine physicians independently reviewed 18F-DCFBC PET/CT and 18F-NaF PET/CT images for identification of regions suggestive of metastatic disease. Only lesions that were determined to be highly suggestive of metastatic disease by reader consensus were included in this study. This process was repeated for follow-up imaging. SUVmax was reported for each lesion identified. Within each patient, the SUVmax and SUVmean uptake were calculated from all reported lesions. The total uptake burden, SUVtotal, was calculated as the sum of lesion-SUVtotal (SUVmean × volume) derived from threshold containing 80% of SUVmax from all reported lesions. Response was calculated as the percentage change from baseline to follow-up imaging.
Statistical Analysis
18F-DCFBC and 18F-NaF characteristics (number of lesions, SUV statistics) were correlated to PSA values using Spearman rank correlation. Differences in imaging characteristics across patient status characteristics, such as treatment status and castration status, were evaluated using the Wilcoxon rank-sum or signed-rank tests, when appropriate. The number of detected bone lesions by 18F-NaF PET/CT and 18F-DCFBC PET/CT was compared by the sign test. Correlation of lesion-level statistics across tracers was performed by Spearman correlation estimation for clustered data (20). Lesions were categorized as concordant or discordant across tracers, and uptake characteristics were compared using Wilcoxon rank-sum test for clustered data (21). All tests were 2-sided, and P values of less than 0.05 were considered statistically significant.
RESULTS
Patient demographics are listed in Table 1. At baseline, 9 patients were not on treatment, 16 were on androgen deprivation therapy (ADT) and 3 patients were on ADT + chemotherapy. In total, 26 of 28 patients had metastatic disease detected on 18F-NaF (n = 22) or 18F-DCFBC (n = 15) at baseline, and 21 of 23 had findings on 18F-NaF (n = 19) or 18F-DCFBC (n = 13) at follow-up. As determined by imaging in this study, 3 patients had soft tissue–only metastases, 14 had bone-only disease, and 9 had both soft-tissue and bone disease. The study summary is provided in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org).
Study Demographics
Lesion Detection
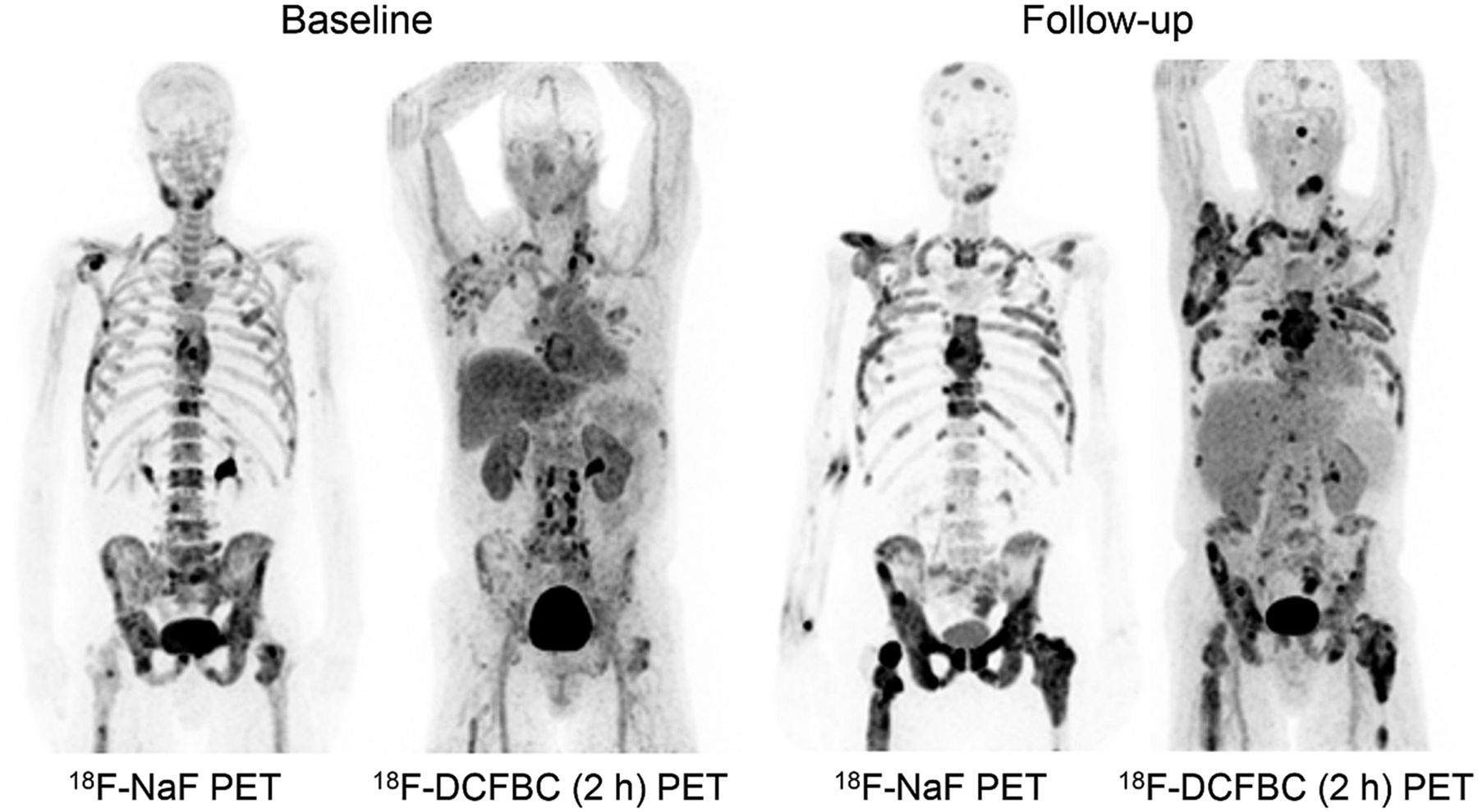
In total, 241 lesions were detected, with 56 soft-tissue lesions identified by 18F-DCFBC only and 185 bone lesions detected on 18F-NaF or 18F-DCFBC. Table 2 summarizes bone lesion detection by tracer at each time point. At baseline, 18F-NaF detected 182 of 185 (98.4%) of bone lesions, significantly higher than 18F-DCFBC at 1 h (45.4%, P < 0.001) and 18F-DCFBC at 2 h (45.9%, P < 0.001). These differences were maintained at follow-up imaging. 18F-DCFBC identified 3 bone lesions that did not have focal uptake on 18F-NaF at baseline and 25 lesions that were not seen on 18F-NaF images at follow-up, all within a single patient with advanced CRPC (Fig. 1). No differences in lesion detection were noted across 18F-DCFBC after injection time points so the 2-h time point was considered only for the remainder of the analysis.
DCFBC Bone Lesion Detection for 1- and 2-Hour Time Points at Baseline and Follow-up Imaging
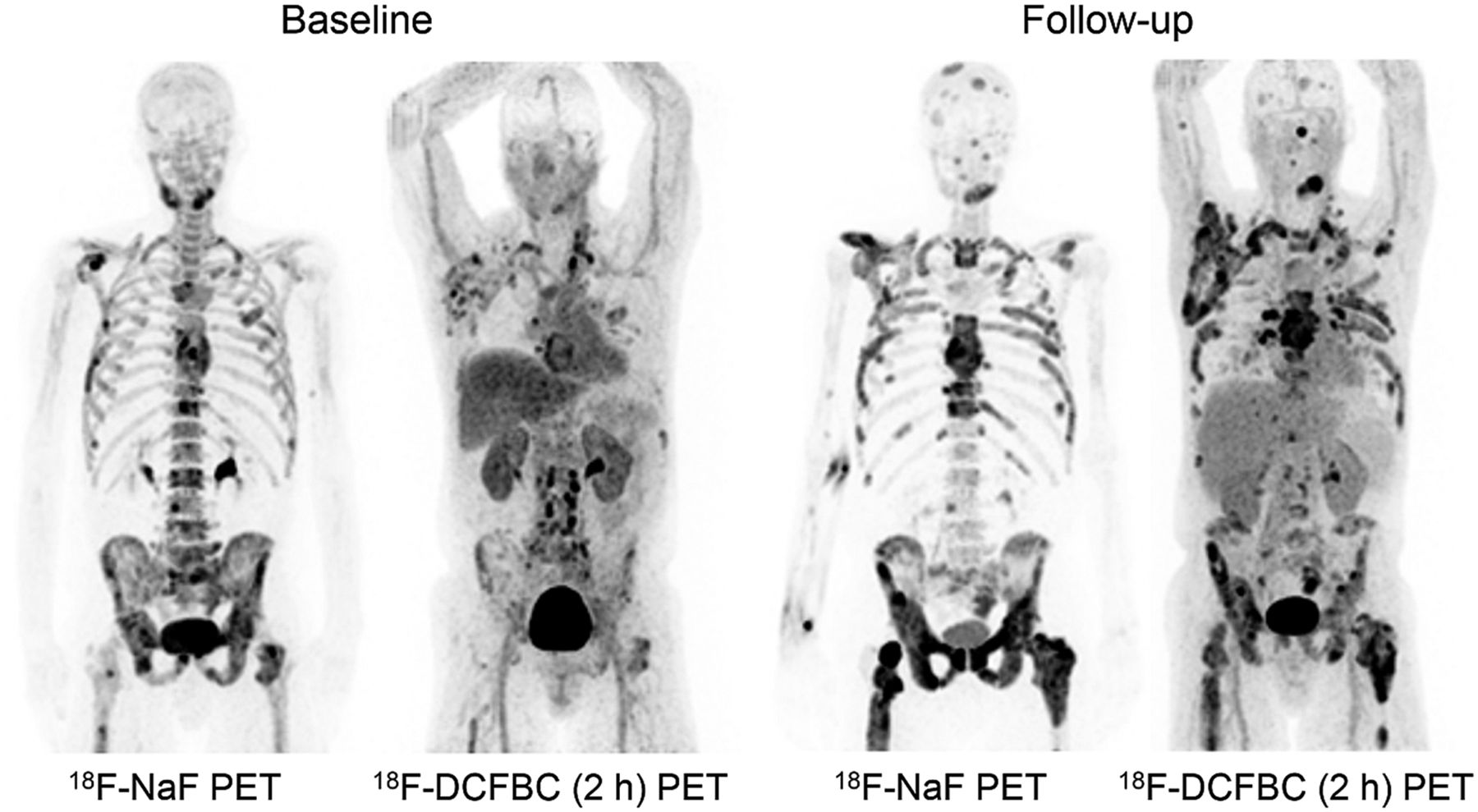
A 64-y-old patient diagnosed with de novo metastatic prostate cancer 4 y before enrollment. Prior treatment history included first- and second-line ADT and chemotherapy. Patient was considered to have CRPC with serum PSA of 812.3 ng/mL at time of baseline imaging. 18F-NaF imaging detected 28 bone lesions, with 17 sites concordant with 18F-DCFBC (2 h) imaging. Three bone and 13 soft-tissue sites were positive only on 18F-DCFBC (2 h) imaging. Treatment at time of baseline imaging included ADT + docetaxel that continued until follow-up imaging 7 mo later, at which time PSA had increased to 1,025 ng/mL. At follow-up, both scans showed disease progression. Number of lesions identified only by 18F-DCFBC (2 h) imaging at follow-up included 25 bone and 11 soft-tissue sites.
Bone Lesion Uptake
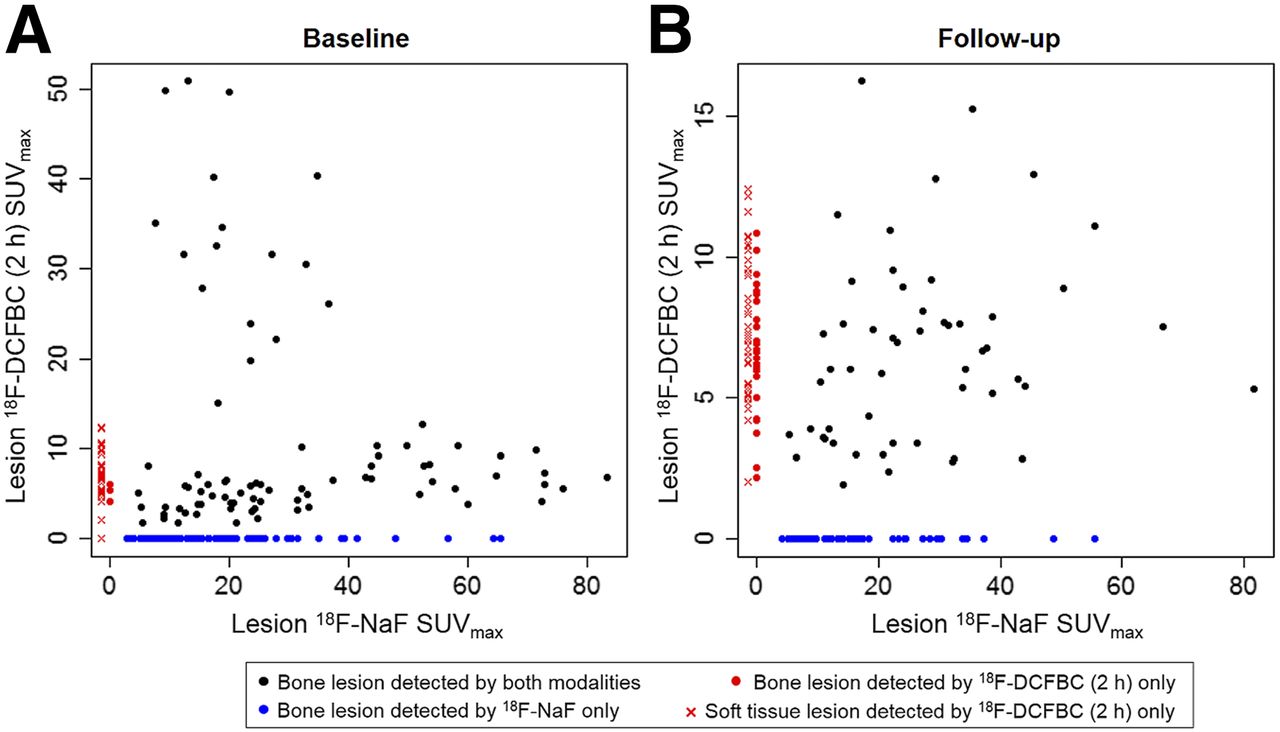
Lesion-level 18F-NaF SUVmax and 18F-DCFBC (2 h) SUVmax were not significantly correlated at baseline (ρ = 0.41, P = 0.095) or follow-up (ρ = 0.29, P = 0.29) (Fig. 2). Lesion-level 18F-NaF SUVmax was lower in bone lesions detected only by 18F-NaF than 18F-NaF SUVmax in bone lesions detected by both tracers, nearing significance at baseline (P = 0.06) and significant at follow-up (P = 0.006) (Table 3). This trend was not noted for 18F-DCFBC (2 h) SUVmax characteristics.

Lesion-based correlation of 18F-NaF and 18F-DCFBC SUVmax at baseline (A: ρ = 0.41, P = 0.095) and follow-up (B: ρ = 0.29, P = 0.29). Lesions detected only by 18F-NaF PET/CT imaging are shown in blue (assigned18F-DCFBC [2 h] SUVmax = 0), and lesions detected only by 18F-DCFBC (2 h) PET/CT imaging are shown in red (assigned 18F-NaF SUVmax = 0), designated by lesion location as soft-tissue (x) or bone (red circle).
18F-NaF and 18F-DCFBC (2 Hour) Lesion SUVmax at Baseline and Follow-up Imaging in Bone Lesions
Correlation to PSA
Median PSA was 2.08 ng/mL (range, 0.01–4379 ng/mL) at baseline imaging and 0.76 ng/mL (range, 0.015–1046 ng/mL) at follow-up. At baseline imaging, patient-level 18F-DCFBC (2 h) uptake characteristics showed significant correlation with PSA levels, with the strongest correlation with the number of lesions (ρ = 0.60, P = 0.001) and SUVtotal (ρ = 0.58, P = 0.003), whereas patient-level 18F-NaF uptake characteristics showed weak correlation to baseline PSA (Table 4; Supplemental Fig. 1). This was maintained at the follow-up imaging time point. For patients receiving treatment in the interim between baseline and follow-up imaging (n = 18), 5 experienced increasing PSA (fold change > 1).
Correlation of PSA with Patient-Level SUV Metrics Derived from 18F-DCFBC (2 Hour) and NaF Uptake at Baseline and Follow-up Imaging, Assessed Using Spearman Correlation Coefficient
Correlation to Disease Status
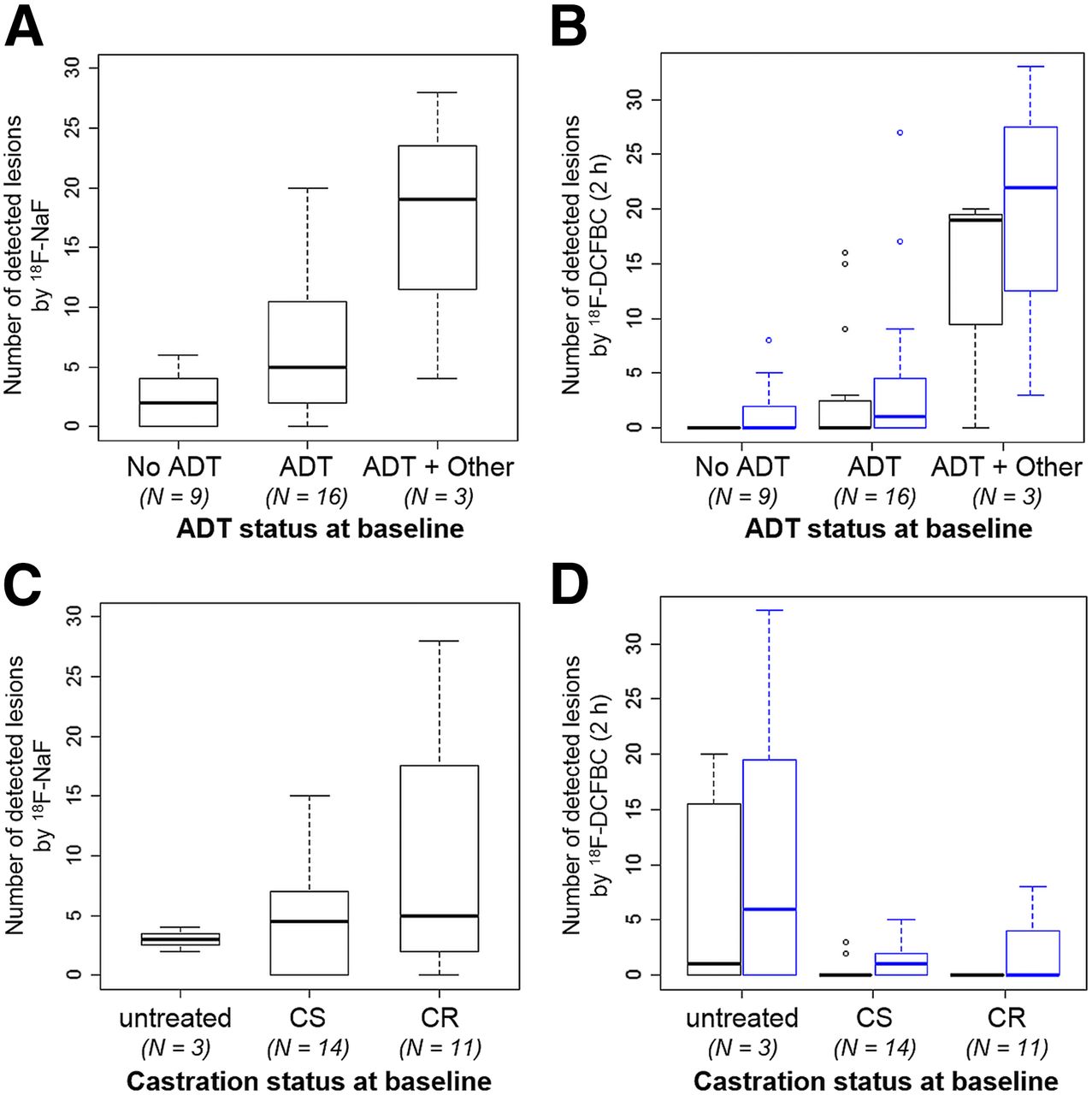
In general, an increasing number of lesions were detected by both tracers as the disease became more advanced, ranging from patients with no treatment at baseline to those with advanced second-line combinations of ADT + chemotherapy (Fig. 3). 18F-NaF detected a higher number of lesions in the group of castrate-sensitive + untreated patients than 18F-DCFBC (2 h) at baseline, nearing statistical significance for all lesions (P = 0.06) and significant for bone-only lesions (P = 0.002) (Figs. 3C and 3D). Patients were then stratified by median PSA value and ADT status, assuming that higher PSA on ADT implied more advanced disease (Fig. 4). The primary difference in detection of metastatic lesions between 18F-NaF and 18F-DCFBC (2 h) at baseline was found to occur in patients with a PSA of less than 2 ng/mL who were on ADT at the time of imaging, where 18F-NaF was able to detect significantly more sites of disease in such patients (P = 0.02 for all lesions and 0.01 for bone lesions in Figs. 4A and 4B, respectively). The most extreme example in this group is highlighted in Figure 5. As PSA advanced beyond 2.0 ng/mL, the number of lesions detected using 18F-DCFBC PET/CT equaled or exceeded the number of lesions found with 18F-NaF PET/CT (Fig. 1; Supplemental Fig. 2).
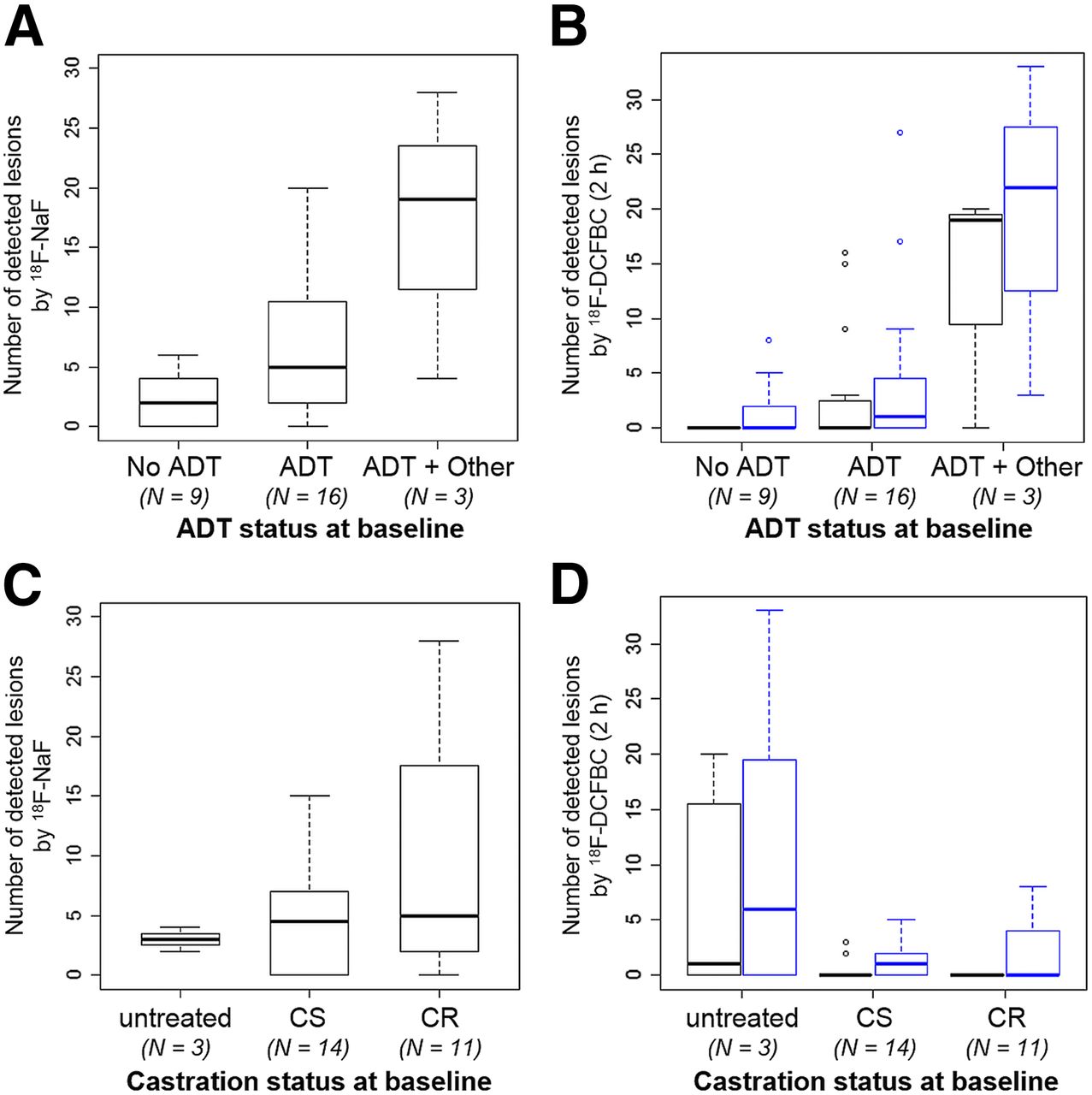
Lesion detection stratified by treatment and castration status at baseline imaging for bone lesions (black) and all lesions (blue). 18F-NaF detection at baseline showed strong dependence on ADT status (A) and castration status (C), where worsening disease status (CR or advanced treatments) show higher disease burden. 18F-DCFBC (2 h) detection also showed dependence on ADT status (B) and castration status (D), though similar levels of detection were only noted in most advanced stages of disease. CR = castrate resistant; CS = castrate sensitive.

Baseline lesion detection stratified by median serum PSA (2 ng/mL) and ADT status (+/−). Patients with low PSA levels not receiving treatment had lowest number of detected lesions for both tracers. In patients receiving treatment and maintaining PSA levels of less than 2 ng/mL, 18F-NaF detected significantly more lesions 18F-DCFBC (2 h) imaging (P = 0.02). In later stages of disease, either by high PSA value (>2 ng/mL) or high PSA and on active treatment, imaging modalities gave similar detection distributions.
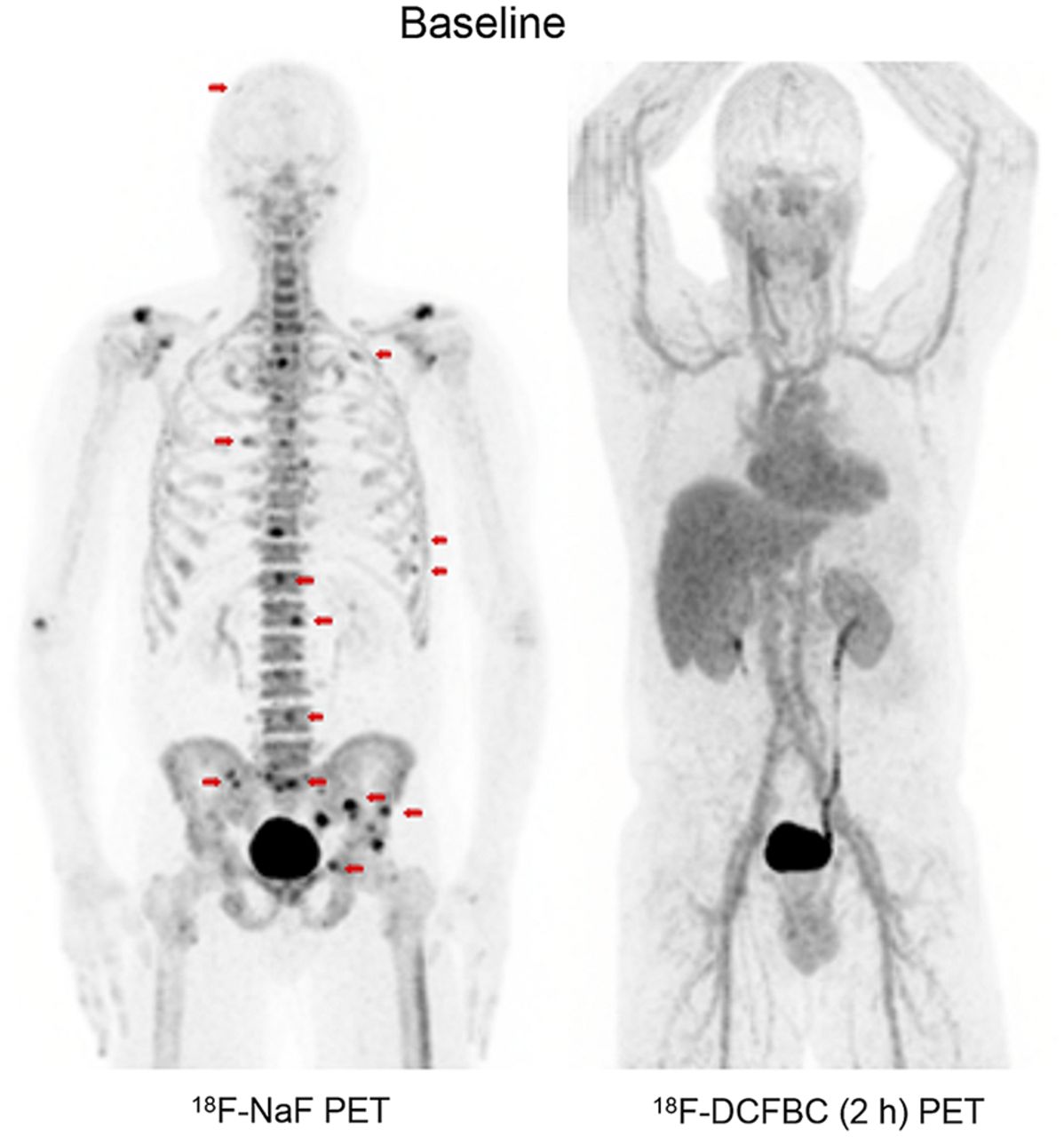
A 48-y-old patient recently diagnosed with de novo metastatic prostate cancer (serum PSA, 20.11 ng/mL), with pathologic validation of metastases in right sacrum and retroperitoneal lymph nodes. Patient started ADT (degarelix) 1 mo before baseline imaging, at which time his PSA was 1.61 ng/mL. 18F-DCFBC (2 h) PET/CT was negative. 18F-NaF PET/CT showed 15 sites detected as highly likely for harboring metastatic disease (red arrows), as well as other regions of uptake secondary to degenerative or benign processes (not included in analysis).
Pathologic Validation
Pathology results were obtained for 6 patients (7 lesions) within 2 mo of study imaging. Of 4 bone lesions, 18F-NaF demonstrated 2 false-positives (both iliac lesions) and 2 true-positives (rib, sacrum) whereas 18F-DCFBC had 1 false-positive (iliac), 1 true-negative (iliac), and 2 false-negatives (rib, sacrum). Of 3 soft-tissue lesions, 18F-DCFBC demonstrated 2 false-negatives (retroperitoneal lymph node, omental lesion) and 1 true-positive (lung).
DISCUSSION
Although PSMA-targeting imaging agents have shown promising sensitivity for recurrent disease after primary cancer treatment, the results in metastatic prostate cancer have yet to be fully characterized. The primary objective of this study was to prospectively explore the detection performance of PSMA-targeted 18F-DCFBC PET/CT in comparison to 18F-NaF PET/CT, a highly sensitive bone scan agent. Within this pilot study, we reported that patient disease and treatment status may influence the diagnostic ability of 18F-DCFBC PET/CT in patients with metastatic disease.
Overall, 18F-NaF PET/CT showed higher detection rates than PSMA-targeted 18F-DCFBC PET/CT at baseline, detecting 98.4% versus 45.9% (2-h after injection) of bone lesions, respectively. The lack of centrally reviewed conventional imaging in this study limits direct comparison to previous works in which 18F-DCFBC PET/CT sensitivity was 88%–92% compared with 71%–82% in conventional bone scan, and 68Ga-PSMA PET/CT achieved a 98%–100% sensitivity compared with 82%–86% in conventional bone scan (12,13). Similar improvements in sensitivity have been shown for 18F-NaF PET/CT compared with planar bone scans, though specificity is still limited by its indirect surrogacy of prostate cancer in the bone (6).
Within this mixed metastatic population, 13 patients had negative 18F-DCFBC scans. The highest discrepancy in modalities was observed in patients early after diagnosis and early after ADT therapy, particularly in hormone-sensitive or minimally symptomatic castrate-resistant disease states (22). Literature tends to support the concept that patients on ADT are more likely to have positive findings on PSMA-targeted imaging (9–11). However, as noted by others, this finding is likely confounded by patients with advanced castrate-resistant disease who are also still on ADT. We have hypothesized the role of ADT and disease status on imaging findings within Figure 6 and the following discussion.
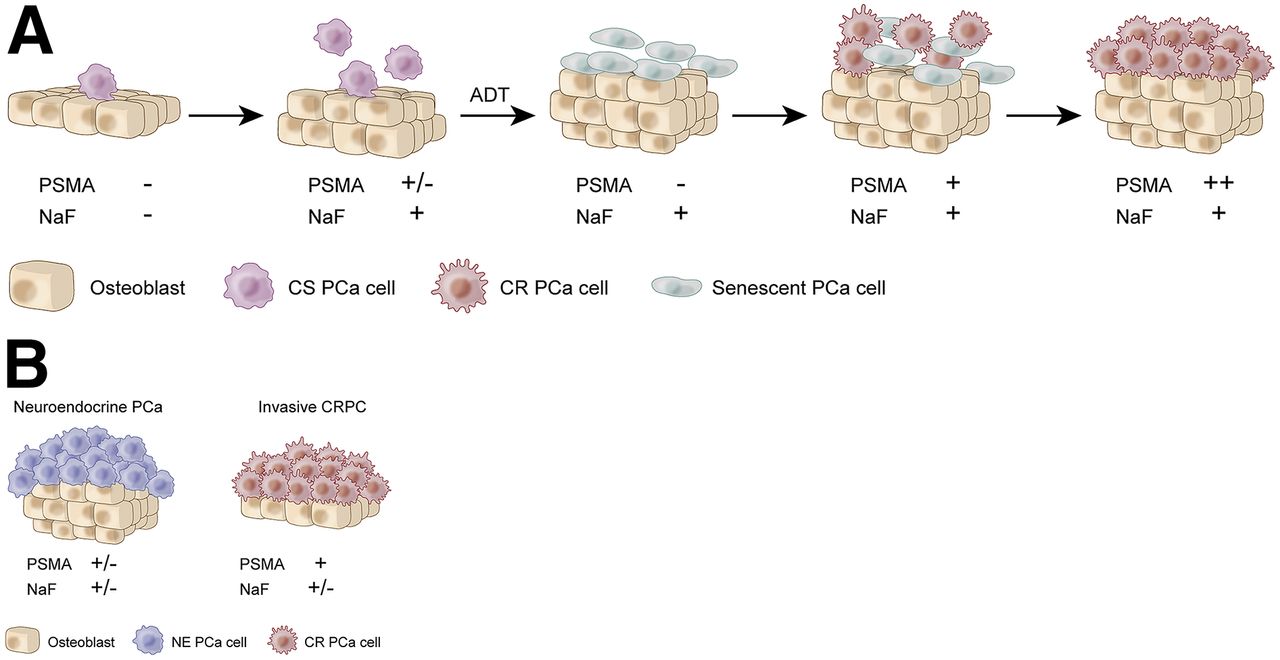
(A) Possible association of prostate cancer disease states with imaging characteristics. In early castrate-sensitive disease states, bone metastases are undetectable by both imaging modalities before eliciting an osteoblastic response enabling 18F-NaF detection that may or may not reach detection limits of PSMA depending on number and PSMA expression of prostate cancer cells . After initiation of ADT, lack of PSMA findings could reflect responsive castrate-sensitive disease-causing involution or initial senescence of cancer cells, whereas persistent 18F-NaF findings may detect regions of residual boney reaction. PSMA and 18F-NaF are expected to show concurrent findings as disease advances to castrate-resistant states before progressive growth of advanced castrate-resistant disease after first- and second-line therapies, where PSMA findings may exceed that of 18F-NaF. (B) Other disease states not captured could include neuroendocrine variants of prostate cancer that may be poorly captured by either modality and invasive castrate-resistant disease characterized by extensive bone marrow replacement in end-stage metastatic CRPC with a weakened bone-reaction (30).
After beginning first-line ADT, androgen-sensitive cells will demonstrate a decrease in cellular proliferation, resulting in apoptosis in some, but not all, cancer cells (23,24). However, prostate cancer bone metastases have often initiated an osteoblastic reaction that persists even after successful ADT (25,26). Within this window, it is possible that ADT has suppressed oncogenic activity in PSMA-expressing cells such that imaging is unable to detect remaining senescent cells, whereas 18F-NaF still recognizes bone response. Additionally, bone scan of any type is susceptible to flare in which the osteoblastic reaction briefly increases after initiation of ADT. In this sense, PSMA-targeted PET provides a more accurate assessment of prostate cancer activity, both in bone and soft tissue, reflected in the strong correlation of 18F-DCFBC and PSA in this study. In the absence of treatment, these findings could also support the hypothesis that a small population of prostate cancer cells may amplify the osteoblastic activity so that 18F-NaF detection is possible but still fails to reach the detection threshold of PSMA-targeting agents (12).
In later stages of disease, lesion detection was not significantly different across the 2 tracers, particularly in advanced, symptomatic metastatic CRPC disease states (22). At the follow-up time point, 18F-DCFBC PET/CT was able to detect more bone lesions than 18F-NaF PET/CT in 1 patient with severe disease progression (Fig. 1). This is in agreement with reports from other PSMA-targeting agents in advanced metastatic CRPC (13,15,16). These findings support the literature indicating PSMA expression increases throughout advanced stages of disease (27). The metastatic foci positive only on 18F-DCFBC appeared as ground-glass findings on CT, likely demonstrating active tumor invasion with insufficient osteoblastic activity to trigger 18F-NaF uptake. Overall, the findings of this study are important to validate in the future for selection and monitoring of targeted radionuclide therapies, where false-negatives on either PSMA-targeting agents or 18F-NaF imaging could hinder treatment effectiveness.
PSA correlation with number of lesions and SUV characteristics were stronger with 18F-DCFBC imaging than with 18F-NaF imaging at baseline. 18F-NaF is inherently limited to only detecting bone disease, compared with PSMA-targeting agents that can capture the burden of both bone and soft-tissue disease. No treatment regimen was defined by this imaging protocol; therefore, the timing of both treatment and follow-up scans was variable but future studies are needed to explore treatment response assessment with both agents.
There are several limitations within this relatively small study of a heterogeneous population of metastatic prostate cancer patients. Very few histopathologic validation specimens were available for review, as is common in the metastatic setting. Two of 4 bone biopsies were shown to be false-positives on 18F-NaF, reflecting its modest specificity. Additionally, results from biopsy indicated some frequency of false-negative PSMA scans. Importantly, 18F-DCFBC is considered a first-generation PSMA-targeting agent with relatively low binding affinity to PSMA and increased vascular background activity. This may compromise its sensitivity in early disease. A second-generation PSMA-targeting agent, 18F-DCFPyL, possessing higher binding affinity to PSMA and rapid blood clearance, is currently in clinical trials (14,15,28). Multiple PSMA-based tracers are currently under development for clinical use in prostate cancer, including 99mTc, 68Ga, and 18F ligands (29). Although the role of PSMA-targeted imaging in the setting of biochemically recurrent disease has been well explored, its role in metastatic disease requires further investigation.
CONCLUSION
In this study, 18F-NaF PET/CT and PSMA-targeting 18F-DCFBC PET/CT were prospectively compared for detection of metastatic disease. Although attractive due to its ability to identify both bone and soft-tissue disease, we present evidence that the utility of PSMA-targeting PET/CT imaging in metastatic prostate cancer appears to depend on patient disease course and treatment status. Notably, 18F-NaF PET/CT and 18F-DCFBC PET/CT were largely concordant in metastatic CRPC. Further research is warranted to elucidate the dependence of disease status and timing of treatment on detection characteristics of PSMA-targeting PET/CT agents.
DISCLOSURE
This project has been funded in whole or in part with federal funds from the National Cancer Institute, National Institutes of Health, under Contract No. HHSN261200800001E. The content of this publication does not necessarily reflect the views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products, or organizations imply endorsement by the U.S. Government. This project was supported in part by the Intramural Research Program of the NIH and NIH grant CA111982. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Anita Ton, Juanita Weaver, Phillip Eclarinal, Alicia Forest, G. Craig Hill, George Afari, Bradford J. Wood, and Maria J. Merino for their contribution. Contract No. HHSN261200800001E. The content of this publication does not necessarily reflect the views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products, or organizations imply endorsement by the U.S. government.
Footnotes
Published online Mar. 30, 2018.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication December 21, 2017.
- Accepted for publication March 21, 2018.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.