


Abstract
743
Objectives: PET with 15O labelled water ([ 15O]H2O) is currently the gold standard for measuring cerebral perfusion. Iterative reconstruction of low count PET data as encountered with short frames from dynamic [15O]H2O images can yield biased and noisy images1. The recently proposed complementary frame reconstruction (CFR)2 indirectly generates a short frame by subtracting two long frames which differ only by the inclusion of counts from the short frame. This approach allows the inclusion of negative values and the authors claim that it can reduce both bias and noise in the low count frames. The current work investigates the benefits and limitations of CFR on dynamic [15O]H2O images using both phantom and clinical brain data acquired on the High Resolution Research Tomograph.
Methods: A modified Esser image quality phantom3 was filled with around 100MBq of [15O]H2O with a 4:1 contrast ratio for the 4, 6, 8, 12 and 16mm diameter cylinders while the 25mm diameter cylinder was filled with unlabelled water. Two patients with glioblastoma and two healthy volunteers were also scanned for 5min after bolus injection of [15O]H2O (357-606MBq). Each frame was reconstructed using OP-OSEM without and with resolution modelling (RM) using the default 18F kernel, either conventionally (independent frame reconstruction, IFR) or with CFR (using all frames as the long frame), for 16 subsets and up to 20 iterations. Images were smoothed post reconstruction using Gaussian filters of varying widths (2-6 mm FWHM). The frame durations of the phantom images were chosen to match the net trues in the clinical images4. Regions of interest were manually delineated on the cylinders and background of the phantom images. Bias and noise were quantified using the contrast recovery coefficient (CRC in hot and cold cylinders), background variability (BV)5 and image roughness (IR)5 modified by using the mean volume instead of the mean slice radioactivity concentration. Cerebral perfusion was estimated for the brain images by fitting a one-tissue compartment model with delay and dispersion to region and voxel dynamic data using a sampled arterial blood input function.
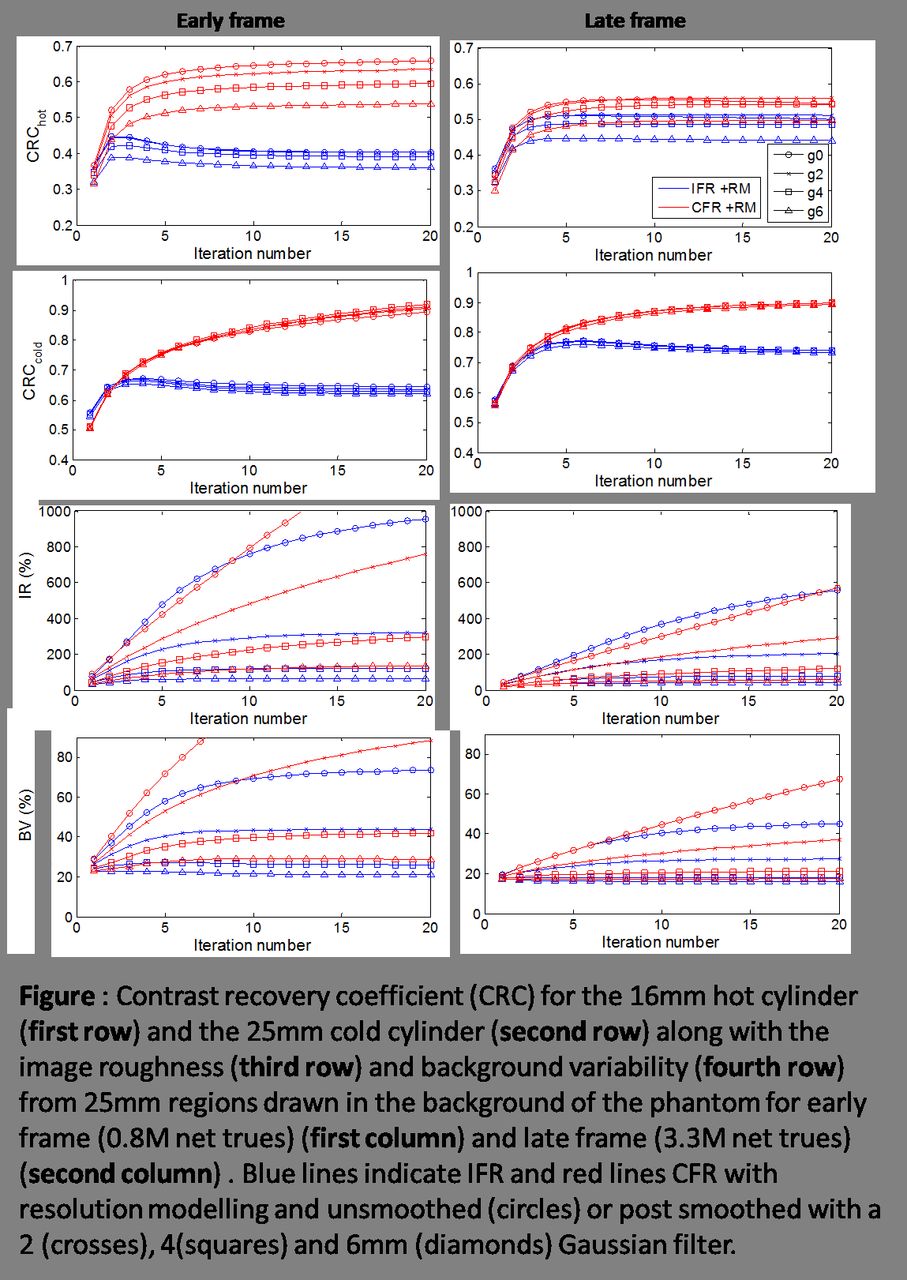
Results: In the low count frame (early, 0.8M net trues) of the phantom, CFR with RM improved contrast in both the hot cylinder (CRC increased from 0.4 to 0.6) and the cold cylinder (CRC increased from 0.6 to 0.9). Improvements were less in the high count frame (late, 3.3M net trues) with CRC increasing from 0.5 to 0.55 in the hot cylinder and from 0.7 to 0.9 in the cold cylinder (figure). Greater improvements with CFR were gained in the cold cylinder by increasing the number of iterations. However, the reduction in bias was accompanied by an increase in noise both voxel-to-voxel (IR) and region-to-region (BV), particularly in the low count image. CFR required smoothing with a 6mm filter to reach a similar noise level as the IFR images smoothed with a 4mm filter, necessary to generate parametric maps of perfusion4 but still yielded superior contrast (figure). CFR also improved contrast in the reconstructed brain images, mainly by halving perfusion in the necrotic core of the glioma. As with the phantom images, greater smoothing was required for CFR (6mm filter) than for IFR (4mm filter) images. A higher noise level in the time-activity curves led to an iteration dependent bias on the perfusion and dispersion estimates at the voxel level.
Conclusion: CFR provided better image contrast and more accurate radioactivity concentrations than IFR at the cost of increased noise. Inclusion of RM lowered noise while minimally improving the accuracy of CFR images, in contrast to IRF images for which both contrast and noise were improved. Further improvements of RM may be gained for both IFR and CFR by widening the point spread function kernel to account for the longer positron range of 15O. Research Support: This research is supported by the Cancer Research UK and EPSRC Cancer Imaging Centre in Cambridge and Manchester (grant C8742/A18097).

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.