


Article Figures & Data
Figures
- FIGURE 1.
Metaiodobenylguanidine (A) and noradrenaline (B).
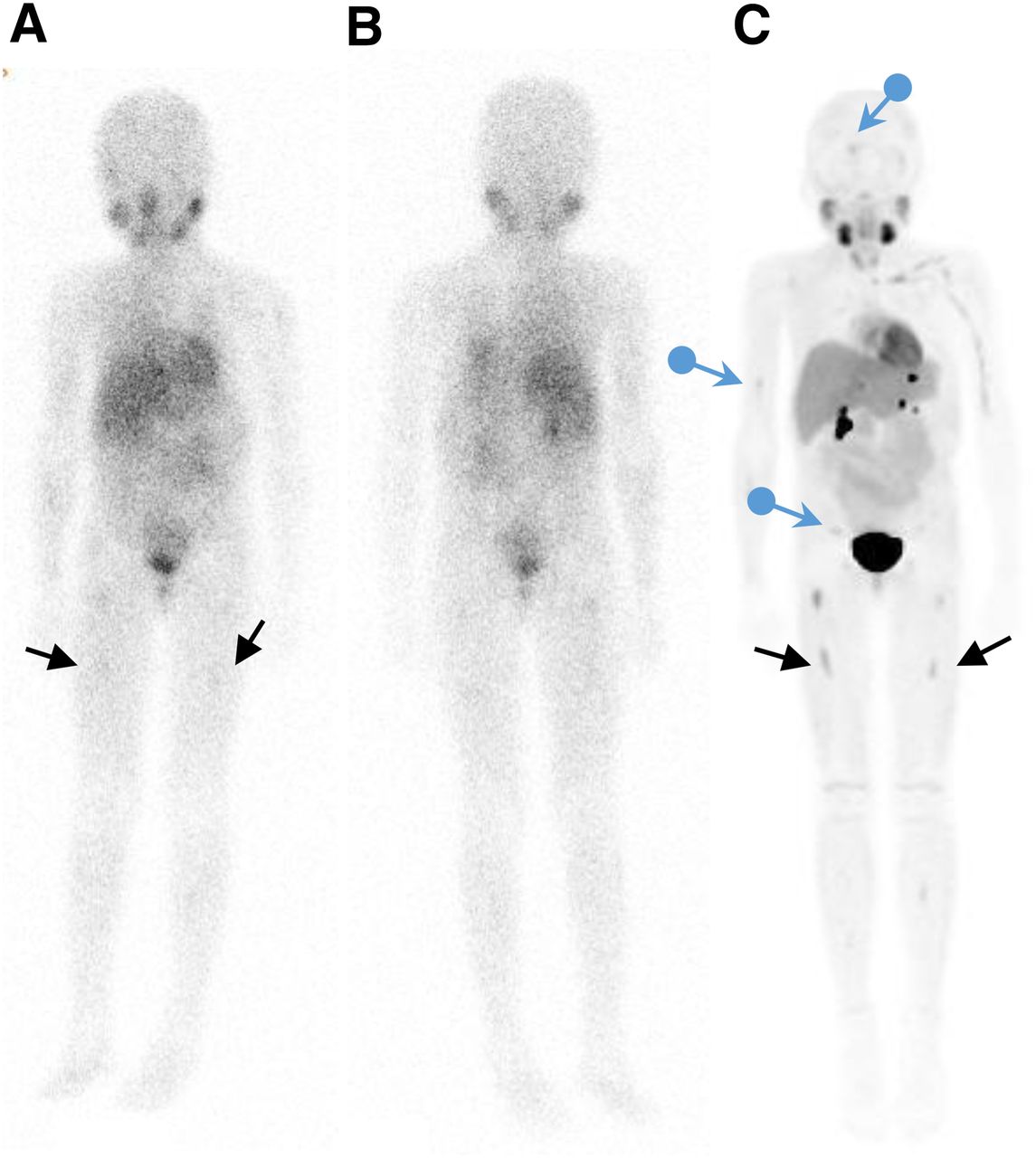
- FIGURE 2.
Imaging with 123I-MIBG and 18F-MFBG. 123I-MIBG whole-body anterior (A) and posterior (B) images show minimal uptake in bilateral femora (arrows). These lesions are better visualized on 18F-MFBG PET/CT imaging (C), which also shows additional lesions (blue arrows) not seen on 123I-MIBG imaging.
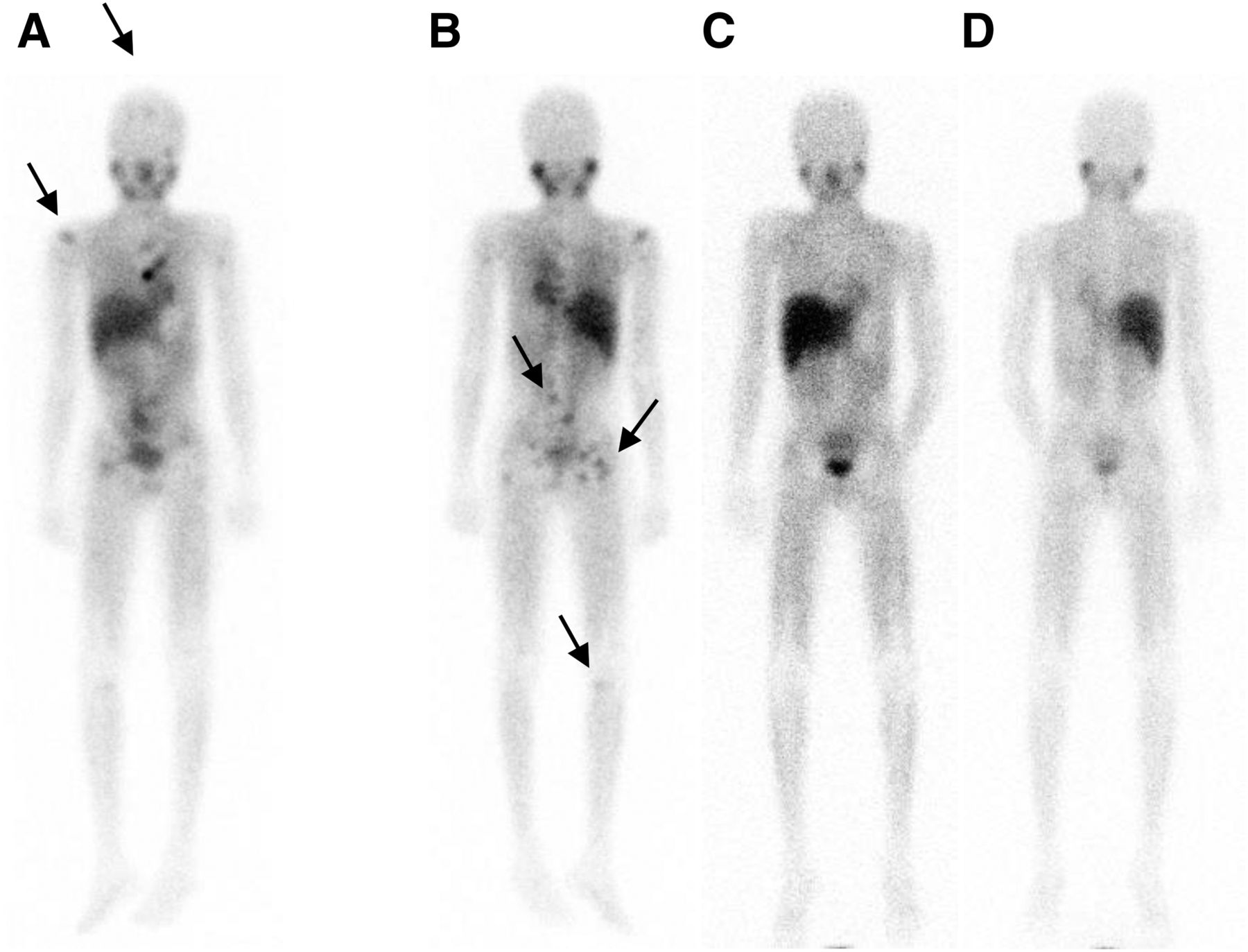
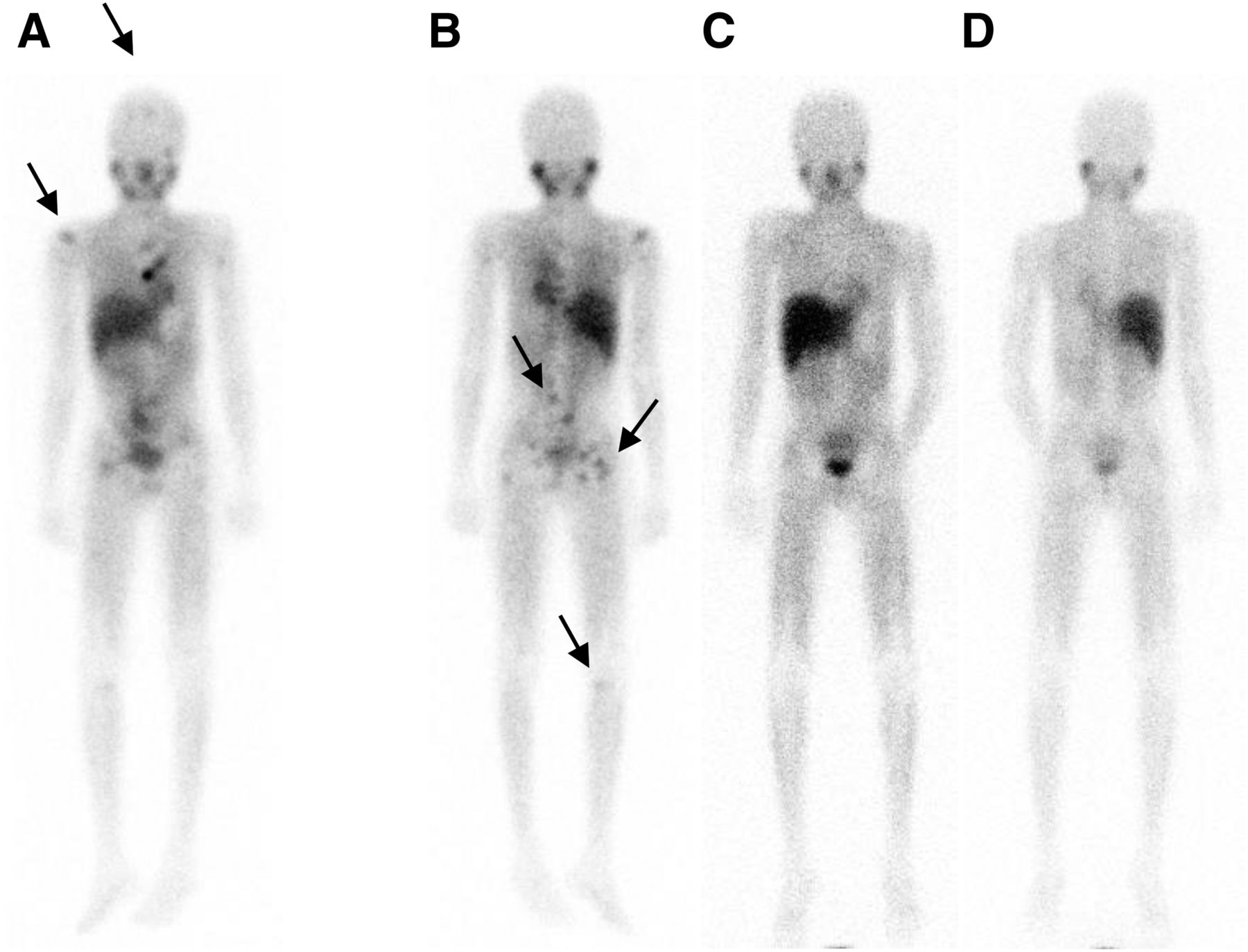
- FIGURE 3.
12-y-old with neuroblastoma. 123I-MIBG pretherapy anterior (A) and posterior (B) images show multiple foci of uptake consistent with lesions in skull, right humerus, vertebrae, pelvic bones, and right tibia (arrows). These lesions are not seen in posttherapy scans (C and D) obtained 8 wk after treatment with 21.8 GBq (590 mCi) of 131I-MIBG (dose of 666 MBq [18 mCi]/kg).
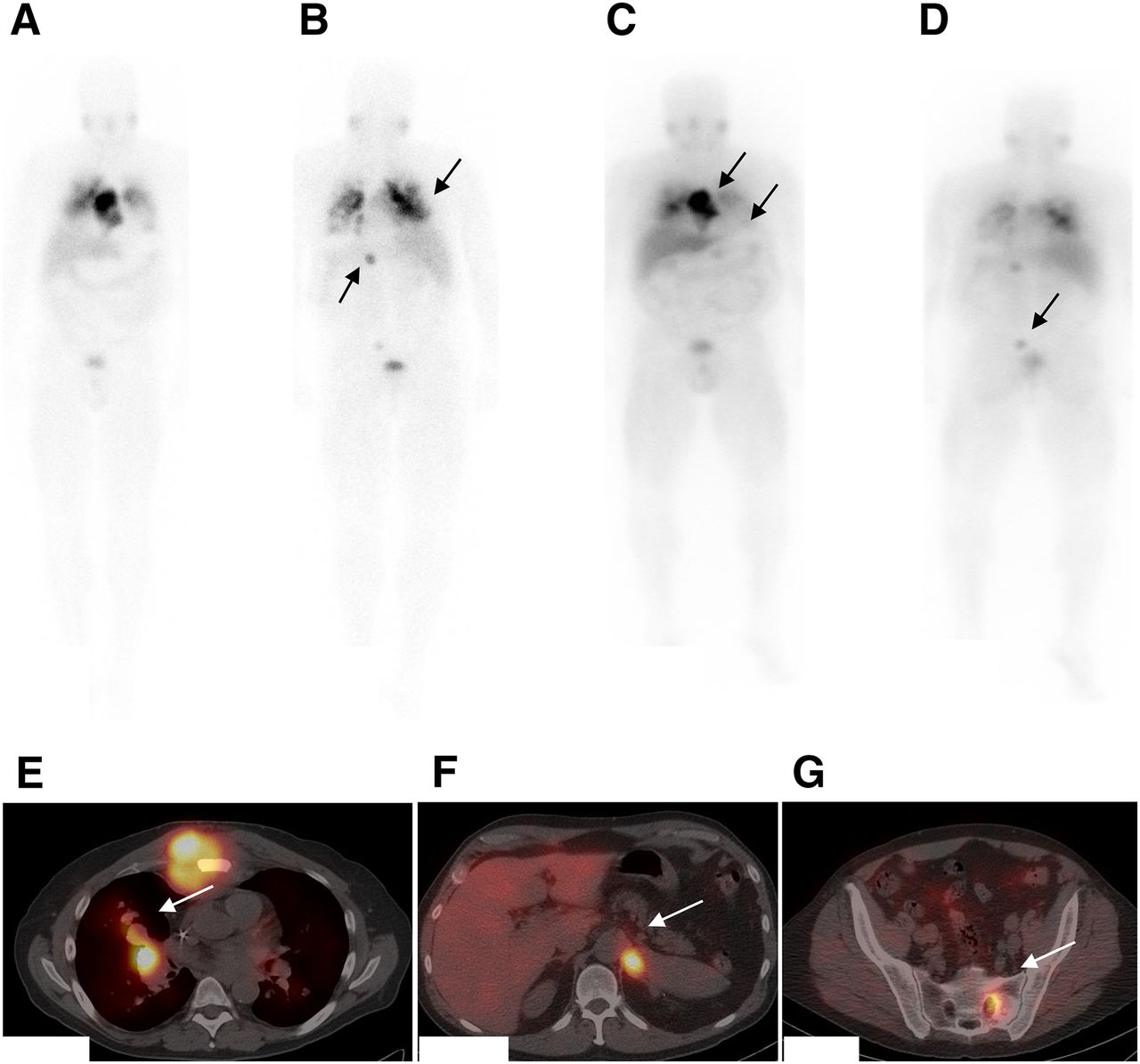
- FIGURE 4.
Patient with metastatic pheochromocytoma presented with progression of disease. 123I-MIBG pretherapy anterior (A) and posterior (B) images show increased uptake in bilateral lung lesions and intense uptake in large sternal lesion, left adrenal lesion, and sacral lesion (arrows). Patient was eligible for 131I-MIBG and was treated with approximately 8,510 MBq (230 mCi) of 131I-MIBG. (C–G) Posttherapy planar anterior (C) and posterior (D) scans and SPECT/CT fused images at 3 levels (E–G) show good targeting of lesions (arrows). Plasma normetanephrine and total metanephrine levels decreased from greater than 20,000 and 40,000 pg/mL, respectively, at baseline to 14,295 and 14,329 pg/mL, respectively, at 13 wk after treatment.

Tables
MIBG treatment dose used Phase No. of patients ASCT Combination Salient results Reference Up-front/induction First of 2 doses: 157–804 MBq (21.7 mCi)/kg; second dose: 113–727 MBq (3–19.6 mCi)/kg Retrospective 66 No None Tolerability established in patients with newly diagnosed stage IV disease (n = 66); after 1 and 2 doses: combined grade 3–4 leucopenia in 9% and 25%, respectively, and thrombocytopenia in 11% and 12%, respectively 89 Single dose after 10 d of chemotherapy: 5.5–7.4 GBq (7.4– 16.6 mCi)/kg (not more than 200 mCi) Retrospective 13 Yes Prior chemotherapy Stages III and IV; newly diagnosed; feasible; responses in patients treated with doses of 444 MBq (12 mCi)/kg and higher 90 2–5 doses: fixed dose of 7.4 GBq (200 mCi) for dose 1 and 3.7–5.6 GBq (100–150 mCi) for follow-up treatments Retrospective 44 (41 evaluable) No None High-risk neuroblastoma; OR in 66%; PR in 63% (26/41); greater thrombocytopenia with higher cumulative doses 91 Fixed dose: 3.7–7.4 GBq (100–200 mCi) or 174–563 MBq (4.7–15.2 mCi)/kg for dose 1 and 244–529 MBq (6.6– 14.3 mCi)/kg for dose 2 Retrospective 21 Yes None Feasible in 66%; RR: 38%; no stem cell support needed; mild thrombocytopenia 92 Relapsed/refractory 2 doses (escalation in cohorts); dose 1: 444–777 MBq (12–21 mCi)/kg; dose 2 (based on cumulative body dose): ≤777 MBq (21 mCi)/kg; tandem; red marrow radiation index based 1 21 Yes None Doses given 14 d apart; red marrow dose levels: 4.0, 6.0, and 8.0 Gy; mild toxicity; double MIBG therapy feasible 36 Single dose of 555–666 MBq (15–18 mCi)/kg 2 19 with neuroblastoma; 2 with metastatic PGL/PHEO Yes Arsenic trioxide Toxicity of combination manageable; objective RR: 29% 72 Dose escalating from 296 to 666 MBq (8 to 18 mCi)/kg 1 27 Yes Vorinostat (escalation of dose from 180 to 270 mg/m2) High-risk relapsed or refractory neuroblastoma; toxicity of combination manageable; RR: 12% 74 555–666 MBq (15–18 mCi)/kg; maximum cumulative dose: 44.4 GBq (1,200 mCi) 1/2 32 Yes Irinotecan and vincristine Advanced high-risk neuroblastoma; toxicity of combination manageable; thrombocytopenia and grade 3 diarrhea common toxicities; RR: 32% 75 444–666 MBq (12–18 mCi)/kg 1 24 Yes Myeloablative chemotherapy Refractory neuroblastoma; MTD at 444 MBq (12 mCi)/kg; combination feasible; hepatotoxicity encountered; RR: 27% 78 444–666 MBq (12–18 mCi)/kg (no carrier added) 1 9 Yes None 131I-MIBG dosimetry study to assess renal, liver, and lung doses before therapy; toxicities similar to those of conventional MIBG therapy; RR: 27% 79 444 MBq (12 mCi)/kg in patients without stem cell treatment (n = 16); 666 MBq (18 mCi)/kg in those with stem cell treatment 2 164 Yes (33%) None Progressive, refractory, or relapsed neuroblastoma; RR: 36% (148 patients treated with 666 MBq [18 mCi]/kg; 16 treated with 444 MBq [12 mCi]/kg); CR + PR: 36%; OS: 49% at 1 y and 29% at 2 y 80 1–6 doses: 82–578 MBq (2.2–15.6 mCi)/kg Retrospective 47 No None Relapsed, refractory, or metastatic neuroblastoma; RR: 46% 82 2.4–12.1 GBq (65–327 mCi), based on WB dosimetry 1/2 25 No None Dosimetry-based approach to delivering 1–2.5 Gy of WB absorbed dose; 80% with grade 3–4 thrombocytopenia at 2.5-Gy WB dose; ORR: 33% 83 111–666 MBq/kg (3–18 mCi)/kg 1 30 Yes, in some None High-risk, relapsed neuroblastoma; ASCT required in most patients receiving ≥444 ΜΒq (≥12 mCi)/kg; DLT: 555 MBq (15 mCi)/kg; response in 37%; CR in 1 patient 85 2 doses of 666 MBq (18 mCi)/kg (tandem) ∼6 wk (up to 100 d) apart Retrospective; safety–efficacy 2 76 (41 with second treatment) Yes None Extensively pretreated relapsed neuroblastoma; RR to double MIBG therapy: ∼30% 94 Median dose: 0.44 GBq/kg (11.89 mCi) Retrospective 111 No Yes Stage IV neuroblastoma with refractory disease; better event-free 3-y survival in patients who received MIBG therapy; however, MIBG therapy did not improve survival in patients who had refractory neuroblastoma and were undergoing ASCT 96 1–5 doses: 1.1–4 GBq (30–108 mCi)/treatment 2 26 No None Stage III–IV refractory, relapsed disease; 8 patients with prior ASCT; palliation of pain in 50%; objective response: 0% 98 2 doses; dose 1: 444 MBq (12 mCi)/kg; dose 2 based on remainder for 4-Gy WB dose Feasibility 8 Yes Topotecan In vivo dosimetry for 4-Gy WB dose; MIBG doses given 15 d apart; combination feasible; range of measured absorbed WB doses from treatment: 3.7–4.7 Gy 126 RR = response rate; OR = overall response; PR = partial response; DLT = dose-limiting toxicity; CR = complete response; OS = overall survival; WB = whole body; ORR = objective response rate; MTD = maximum tolerated dose.
131I-MIBG therapy Overall response Reference No. of patients Disease status Activity No. of doses Total activity Objective* Biochemical Symptomatic response Survival Comments 109 48 Metastatic PHEO/PGL High specific activity: 3.7–14.8 GBq (1.32–5.69 mCi)/kg 1–4 NA 1 PR, no CR NA NA; no significant decrease in BP in patients with high systolic BP NA No significant toxicity 107 Group 1: 12 9/12 secreting 555 MBq/dose every 3–4 mo Maximum: 10; median: 7 Maximum: 66.6 GBq; median: 39.4 1 CR, 3 PR (33%) 5 PR (42%) NA 1.9 y No grade 3–4 hematologic toxicity 107 Group 2: 16 9/16 secreting 7.4–12.95 GBq/dose every 6–8 mo Maximum: 6; median: 2 57.2 GBq (median: 24.1) 2 CR, 3 PR (31%) 2 CR, 3 PR (31%) NA 3 y 6 patients had grade 3–4 thrombocytopenia 116 10 Metastatic; symptomatic 5.6 GBq/dose (n = 9); 3.7 GBq every 4–12 mo (n = 1) 1–4 (mean: 2) 10–13.2 GBq (mean 11.6 ± 1.6) (310 ± 44.0 mCi) 3 PR (30%) 5 patients (50%) 5 patients (50%) Mean PFS: 17.5 mo (2–47 mo) No grade 3–4 hematologic toxicity 118 50 Metastatic; 50% with SDHB mutation Phase 2: high dose; 222–333 MBq (6–9 mCi)/kg 1–3 18,204–145,003 GBq (492–3,919 mCi) 27% after first treatment; 50% after second treatment 35% after first dose; 71% after second dose NA OS at 5 y: 64% Grade 3–4 hematologic toxicity in up to 87% 111 33 Metastatic PGL/PHEO Mean first dose: 14.47 ± 4.8 GBq (391 ± 130 mCi) 1–6 Mean: 20.3 ± 11.24 GBq (549 ± 304 mCi); maximum: 1,223 38% 60% 86% Median OS: 56 mo; median survival: 4.7 y Bone marrow suppression in 12% 106 116 (compilation of data from multiple studies at 10 institutions) Metastatic PGL/PHEO Mean dose: 158 (96–300) 1–11 (mean: 3.3) Mean: 490 (96–2,322) 30% 45% 76% 5 patients had CR lasting up to 16–58 mo; better responses were seen in those with soft-tissue disease Mild adverse effects in 41%; 1 patient had fatal marrow aplasia; 45% of the responders had median PFS of 19 mo ↵* Complete response (CR) plus partial response (PR).
NA = not available; BP = blood pressure; PFS = progression-free survival; OS = overall survival.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- First Experience Using 18F-Flubrobenguane PET Imaging in Patients with Suspected Pheochromocytoma or Paraganglioma
- PARP-1-Targeted Auger Emitters Display High-LET Cytotoxic Properties In Vitro but Show Limited Therapeutic Utility in Solid Tumor Models of Human Neuroblastoma
- Does Delayed Excretion of Therapeutic 131I-MIBG Interfere with a 123I-MIBG Diagnostic Scan 6 Weeks After the Therapy?
- Radiolabeled (4-Fluoro-3-Iodobenzyl)Guanidine Improves Imaging and Targeted Radionuclide Therapy of Norepinephrine Transporter-Expressing Tumors
- Theranostic Concepts: More Than Just a Fashion Trend--Introduction and Overview