


Article Figures & Data
Figures
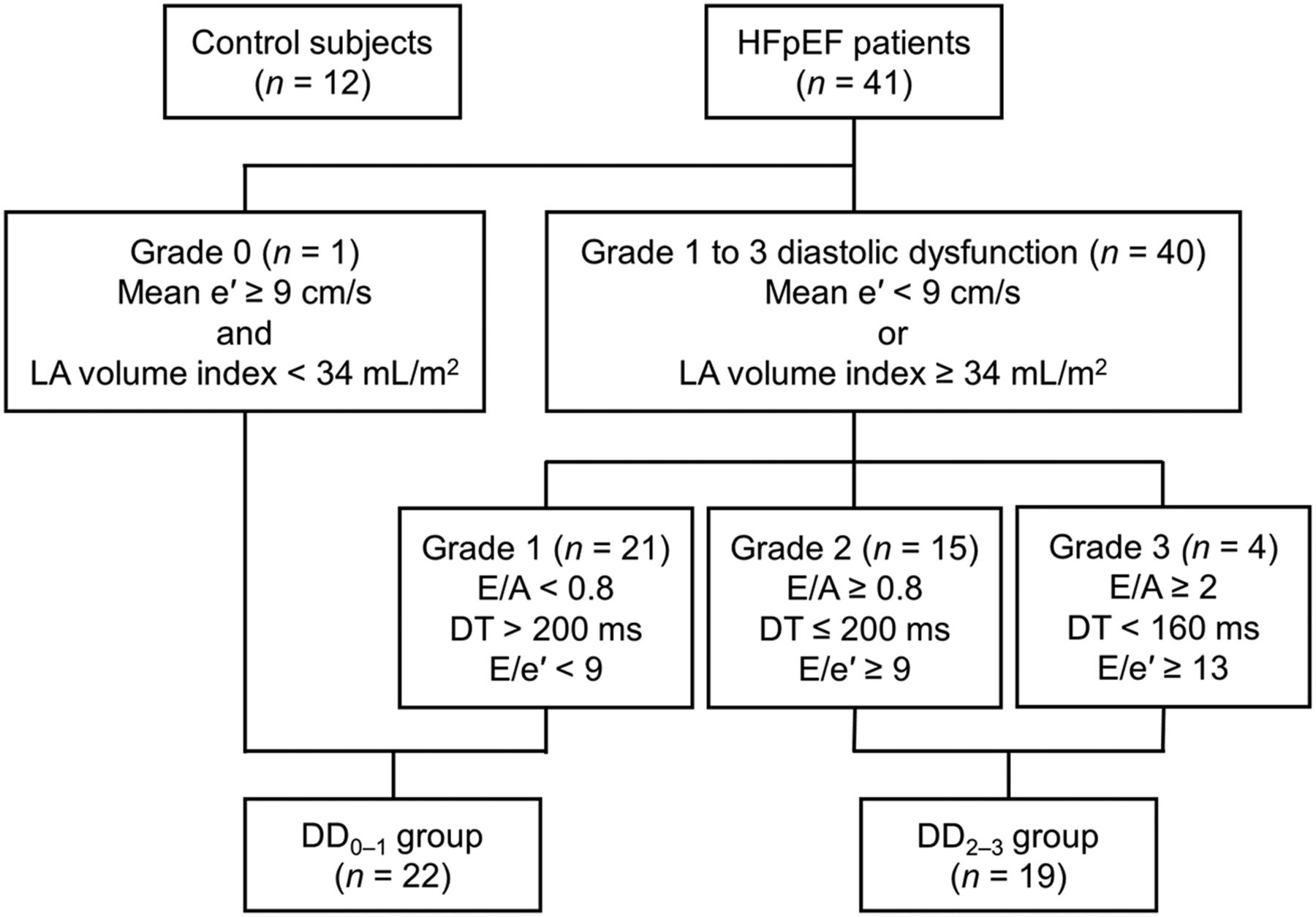
- FIGURE 1.
Participant flowchart and diastolic dysfunction grading of HFpEF patients. DT = deceleration time; LA = left atrial.
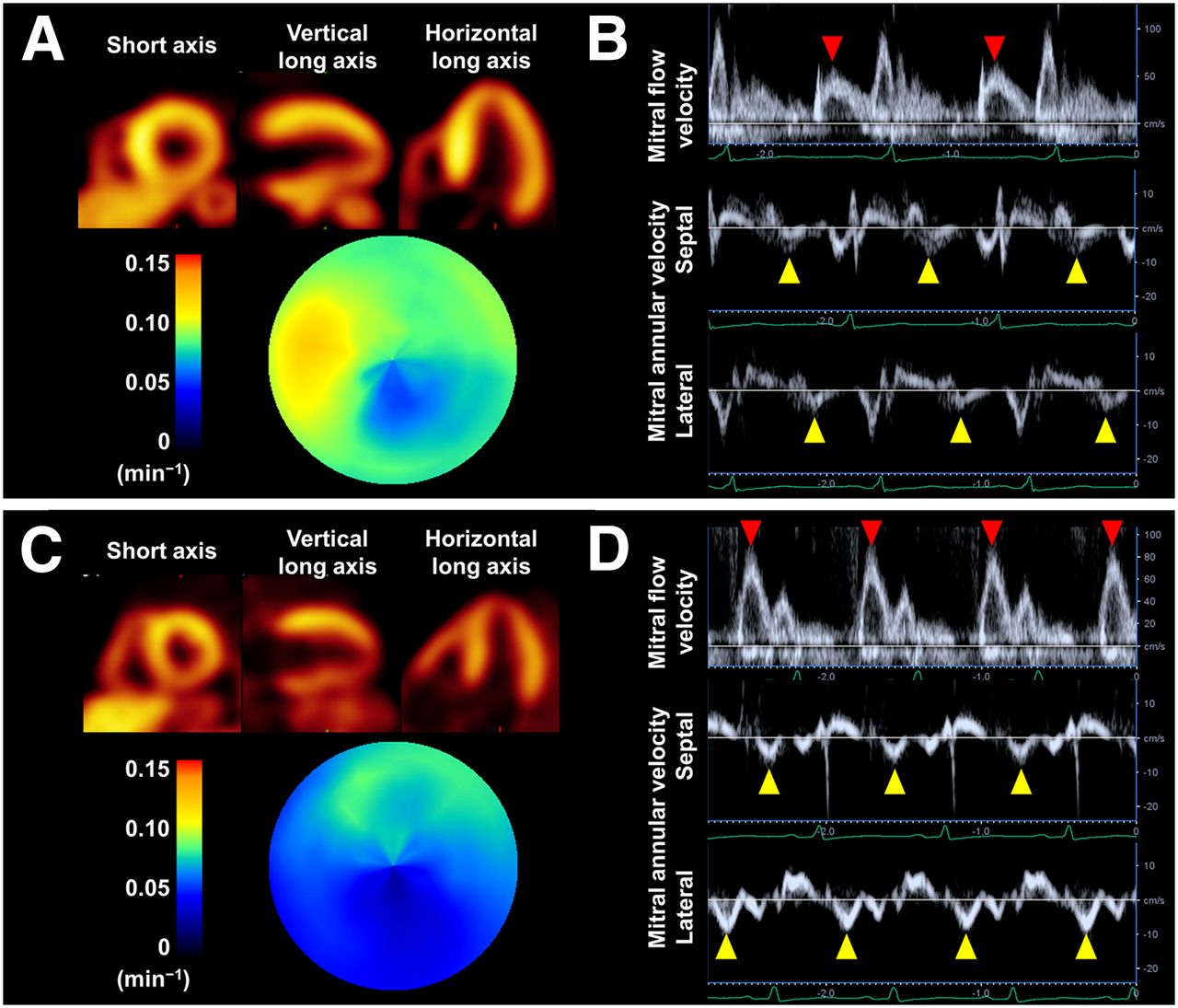
- FIGURE 2.
Representative images of 11C-HED PET (A and C) and Doppler echocardiography (B and D) in 2 HFpEF patients (patient 1 with hypertensive heart disease and grade 1 diastolic dysfunction [A and B]). In patient 2 with cardiac amyloidosis and grade 2 diastolic dysfunction (C and D), the polar map of 11C-HED RI (C) shows more extensive impairment of myocardial sympathetic innervation than that of patient 1 (A). Red arrowheads indicate E wave, and yellow arrowheads indicate e′.
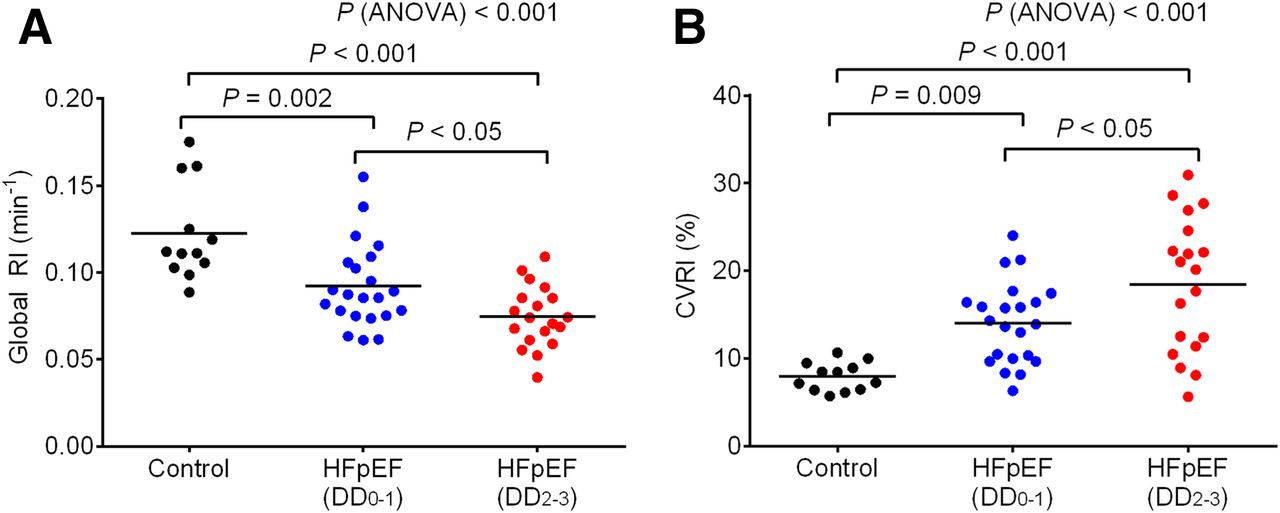
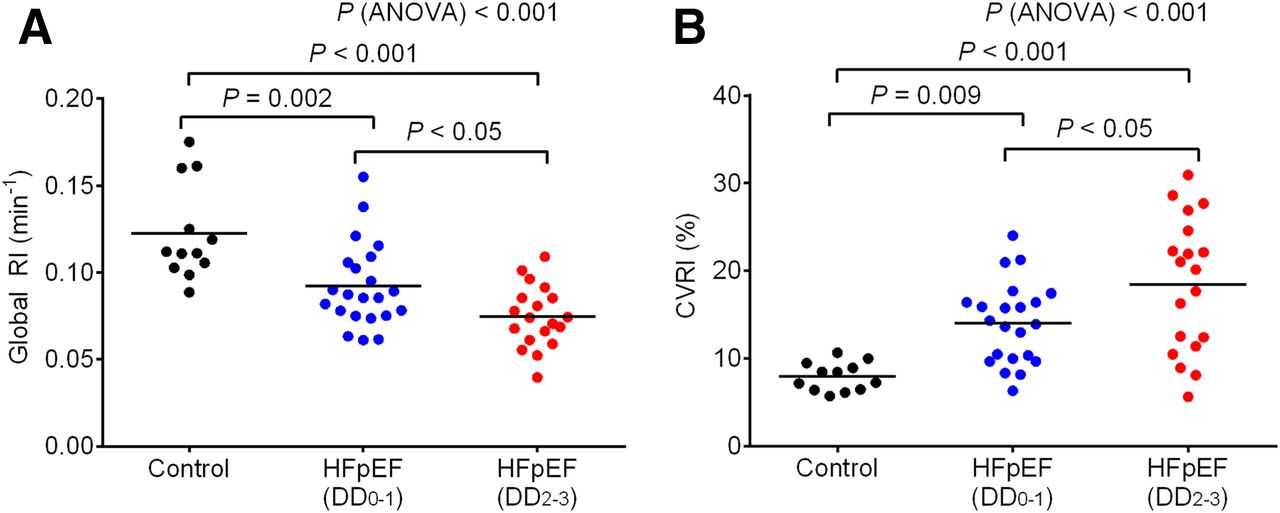
- FIGURE 3.
Scatterplots of global RI (A) and CVRI (B) for comparison among the 3 groups. Horizontal lines indicate mean value.
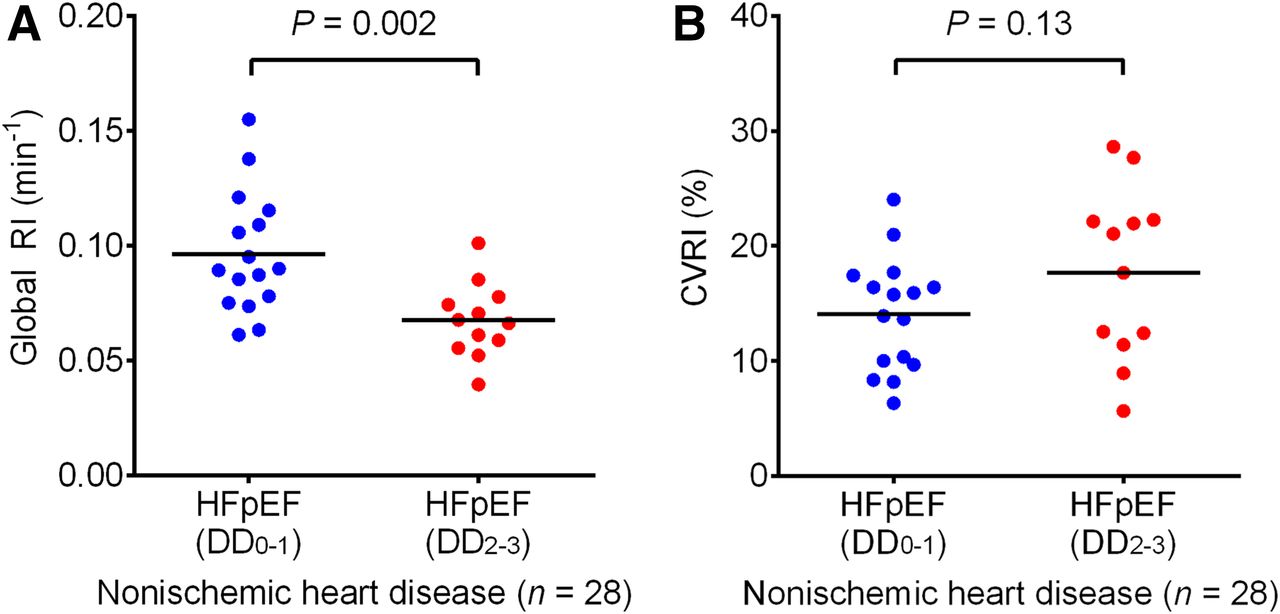
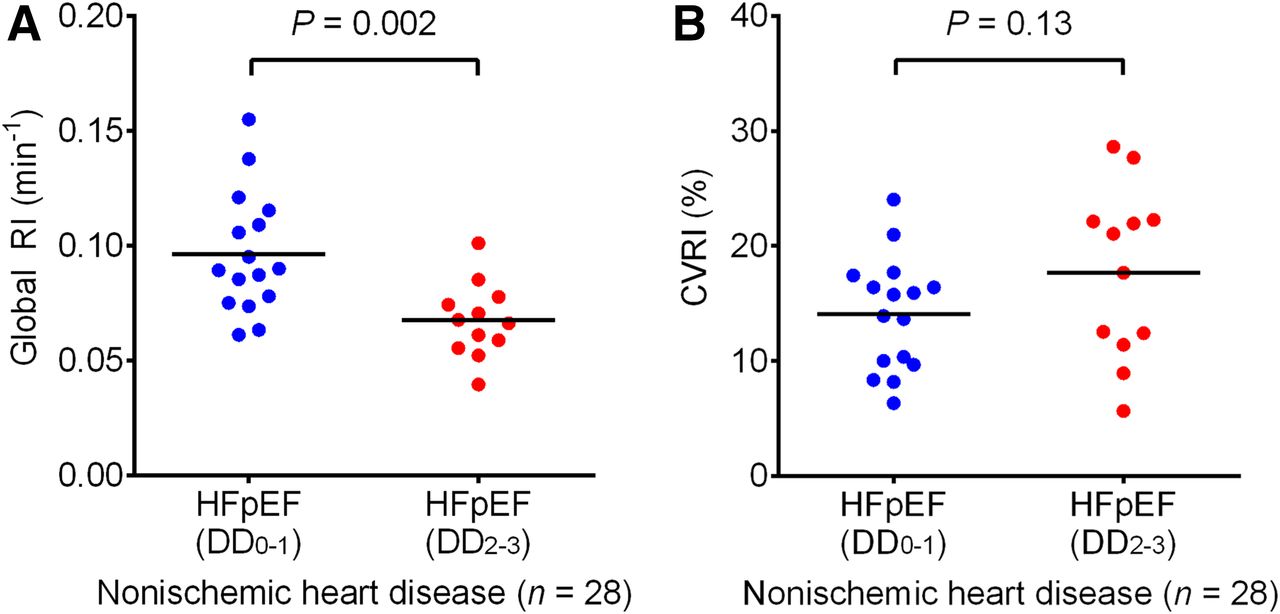
- FIGURE 4.
Scatterplots of global RI (A) and CVRI (B) for comparison between the 2 HFpEF groups with nonischemic heart disease (n = 28). Horizontal lines indicate mean value.
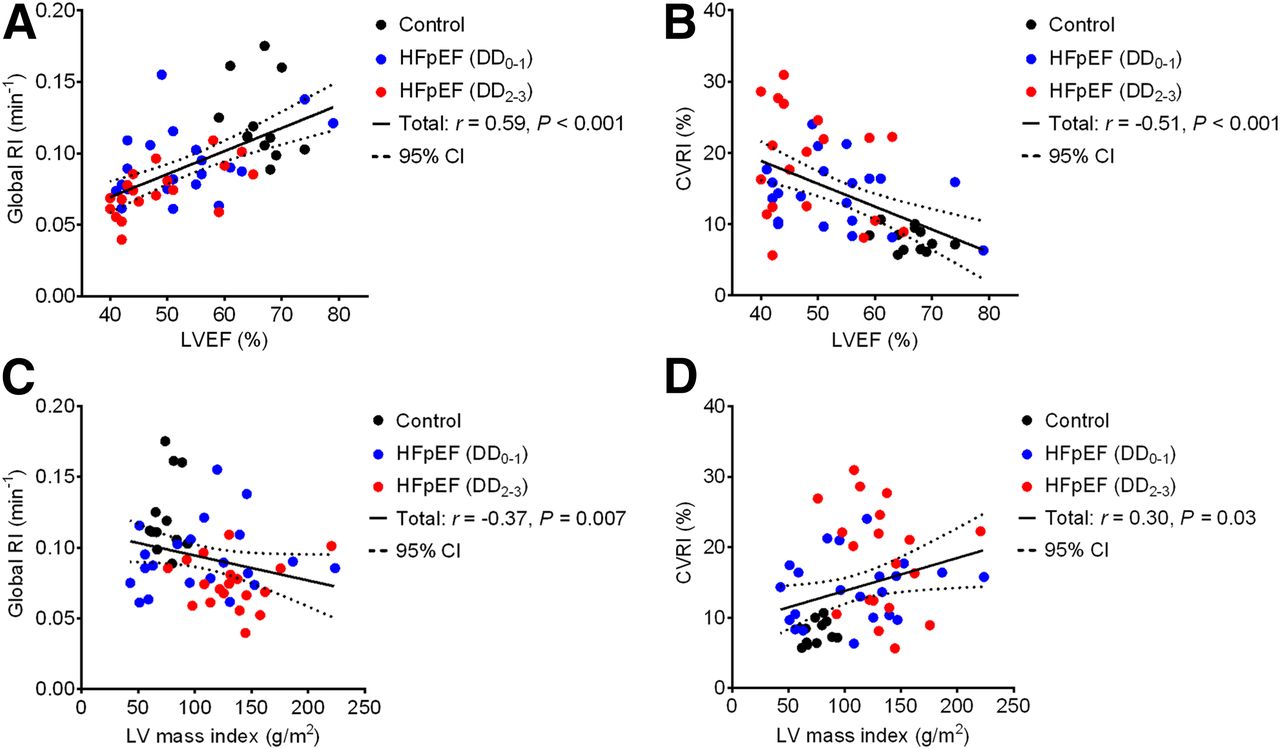
- FIGURE 5.
Scatterplots demonstrate association of LVEF (A and B) and LV mass index (C and D) with global RI and CVRI in study subjects. CI = confidence interval.
Tables
HFpEF Characteristic Control (n = 12) DD0–1 (n = 22) DD2–3 (n = 19) P Age (y) 64 ± 12 65 ± 14 63 ± 16 0.94 Sex 0.20 Male 5 13 14 Female 7 9 5 BMI (kg/m2) 23.4 ± 4.1 24.3 ± 5.0 24.0 ± 4.2 0.87 NYHA functional class (I/II/III) 6/13/3 0/11/8 <0.02 Hypertension 10 (83%) 17 (77%) 8 (42%) 0.02 Diabetes 0 (0%) 10 (45%)† 5 (26%) 0.02 Hyperlipidemia 7 (58%) 15 (68%) 11 (58%) 0.76 Atrial fibrillation 0 (0%) 8 (36%) 7 (37%) 0.047 Coronary artery disease 0 (0%) 6 (27%) 7 (37%) 0.06 Prior myocardial infarction 0 (0%) 6 (27%) 7 (37%) 0.06 Heart failure etiologies 0.03 Ischemic cardiomyopathy 5 (23%) 7 (37%) Hypertrophic cardiomyopathy 5 (23%) 4 (21%) Hypertensive heart disease 6 (27%) 1 (5%) Dilated cardiomyopathy 0 (0%) 5 (26%) Other 6 (27%) 2 (11%) Blood data Hemoglobin (g/dL) 13.0 ± 1.6 12.9 ± 1.9 13.5 ± 1.5 0.46 Creatinine (mg/dL) 0.65 (0.57–0.92) 0.81 (0.66–0.99) 0.87 (0.70–1.13) 0.12 Estimated glomerular filtration rate (mL/min/1.73 m2) 75.6 ± 19.4 66.3 ± 17.2 67.7 ± 33.2 0.56 B-type natriuretic peptide (pg/mL) 11.5 (8.5–19.0) 97.0 (25.2–223.3)* 78.8 (34.1–242.0)* <0.001 Norepinephrine (pg/mL) 426 ± 177 367 ± 216 371 ± 199 0.70 Troponin T (ng/mL) 0.004 (0.003–0.009) 0.016 (0.009–0.045)* 0.038 (0.014–0.058)* <0.001 Medication ACE-Is or ARBs 5 (42%) 20 (91%)* 13 (68%) 0.009 β-blockers 1 (8%) 14 (64%)* 18 (95%)*‡ <0.001 Aldosterone antagonists 2 (17%) 1 (5%) 5 (26%) 0.15 Diuretics 1 (8%) 7 (32%) 9 (47%) 0.08 Calcium-channel blockers 7 (58%) 10 (45%) 6 (32%) 0.33 Statins 4 (33%) 12 (55%) 10 (53%) 0.46 Warfarin 0 (0%) 2 (9%) 5 (26%) 0.08 DOACs 0 (0%) 6 (27%) 3 (16%) 0.13 SHFM mean life expectancy (y) 10.6 ± 4.9 9.7 ± 3.3 0.50 ↵* P < 0.01 vs. control.
↵† P < 0.05 vs. control.
↵‡ P < 0.05 vs. DD0–1.
BMI = body mass index; NYHA = New York Heart Association; ACE-Is = angiotensin-converting enzyme inhibitors; ARBs = angiotensin II receptor blockers; DOACs = direct oral anticoagulants.
Data are mean ± SD; n, with percentages in parentheses; or median, with interquartile ranges in parentheses.
HFpEF Parameter Control (n = 12) DD0–1 (n = 22) DD2–3 (n = 19) P Systolic blood pressure (mm Hg) 121 ± 16 109 ± 22 107 ± 21 0.18 Diastolic blood pressure (mm Hg) 67 ± 10 61 ± 12 62 ± 12 0.29 Heart rate (bpm) 58 ± 7 58 ± 11 57 ± 10 0.96 LVEF (%) 67 (64–69) 51 (43–57)* 45 (42–58)* <0.001 LV end-diastolic diameter (mm) 46 ± 4 51 ± 8 52 ± 9 0.07 LV end-systolic diameter (mm) 28 ± 2 37 ± 10† 41 ± 10* 0.002 Left atrial end-systolic diameter (mm) 37 (33–39) 42 (39–49)† 43 (34–46) 0.03 LV mass index (g/m2) 75 ± 11 123 ± 36* 133 ± 33* <0.001 Left atrial volume index (mL/m2) 33 (31–38) 42 (35–53) 43 (31–59) 0.10 E/A 0.79 (0.67–0.98) 0.61 (0.55–0.77) 1.02 (0.85–1.43)‡ 0.002 E wave deceleration time (ms) 216 (195–242) 219 (184–242) 182 (167–294) 0.69 Septal e′ (cm/s) 7.2 ± 2.4 6.0 ± 2.4 4.7 ± 1.3* 0.009 Lateral e′ (cm/s) 8.8 ± 1.8 8.9 ± 3.9 6.9 ± 2.0 0.07 E/e′ 8.7 (7.9–9.2) 9.2 (8.0–11.1) 13.0 (10.0–16.3)*‡ <0.001 ↵* P < 0.01 vs. control.
↵† P < 0.05 vs. control.
↵‡ P < 0.01 vs. DD0–1.
LV = left ventricular; E/A = peak velocity of early-diastolic mitral flow (E) to peak atrial velocity (A) ratio; E/e′ = E to mean early diastolic annular velocity (e′) ratio.
Data are mean ± SD; n, with percentages in parentheses; or median, with interquartile range in parentheses.
HFpEF Parameter Control (n = 12) DD0–1 (n = 22) DD2–3 (n = 19) P Global RI (min−1) 0.123 ± 0.028 0.092 ± 0.024* 0.075 ± 0.018*† <0.001 Regional RI (min−1) Anterior 0.124 ± 0.028 0.097 ± 0.028‡ 0.078 ± 0.019*† <0.001 Septal 0.128 ± 0.030 0.099 ± 0.025* 0.085 ± 0.024* <0.001 Inferior 0.119 ± 0.029 0.087 ± 0.022* 0.069 ± 0.019*† <0.001 Lateral 0.119 ± 0.027 0.087 ± 0.027* 0.067 ± 0.016*† <0.001 CVRI (%) 7.9 ± 1.6 14.1 ± 4.7* 18.4 ± 7.7*† <0.001 11C-hydroxyephedrine influx rate (mL⋅g−1⋅min−1) 0.302 ± 0.053 0.231 ± 0.065* 0.189 ± 0.053* <0.001 - TABLE 4
Logistic Regression Analysis to Identify Clinical Factors Contributing to Presence of DD2–3 in HFpEF Patients
Univariate Multivariate model 1 Multivariate model 2 Factor OR P OR P OR P Age (per 10 y) 0.92 (0.59–1.43) 0.72 – – – – Sex (male) 1.94 (0.53–7.77) 0.32 – – – – BMI (kg/m2) 0.99 (0.86–1.13) 0.88 – – – – Hypertension 0.21 (0.05–0.79) 0.02 0.29 (0.06–1.37) 0.12 0.18 (0.03–0.98) 0.048 Diabetes 0.43 (0.11–1.56) 0.20 – – – – Coronary artery disease 1.56 (0.41–6.03) 0.51 – – 3.41 (0.59–25.2) 0.17 Atrial fibrillation 1.02 (0.28–3.68) 0.97 – – – – B-type natriuretic peptide (per 100 pg/mL) 1.19 (0.87–1.81) 0.29 – – – – SHFM mean life expectancy (y) 0.95 (0.81–1.10) 0.49 – – – – LVEF (per 5%) 0.76 (0.51–1.08) 0.13 1.04 (0.60–1.83) 0.89 1.08 (0.60–2.05) 0.80 LV mass index (per 10 g/m2) 1.08 (0.90–1.32) 0.39 – – – – Global RI (per 0.01 min−1) 0.64 (0.41–0.90) 0.008 0.66 (0.38–0.99) 0.044 0.62 (0.33–0.98) 0.042 CVRI (per 5%) 1.76 (1.06–3.20) 0.03 1.88 (1.01–3.95) 0.046 1.79 (0.94–3.88) 0.08 OR = odds ratio; model 1 = including LVEF and stepwise-selected variables; model 2 = including coronary artery disease, LVEF, and stepwise-selected variables; BMI = body mass index.
Data in parentheses are 95% confidence intervals.
Supplemental Data
Files in this Data Supplement:





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Cardiac Presynaptic Sympathetic Nervous Function Evaluated by Cardiac PET in Patients with Chronotropic Incompetence Without Heart Failure
- Radiotracers to Address Unmet Clinical Needs in Cardiovascular Imaging, Part 1: Technical Considerations and Perfusion and Neuronal Imaging
- Best Practices in Molecular Breast Imaging: A Guide for Technologists
- Imaging of the Cardiac Sympathetic Nervous System Has Potential Value in the Evaluation of Patients with Heart Failure with Preserved Ejection Fraction