


Abstract
In addition to the well-known estrogen receptor (ER) and human epidermal growth factor receptor 2, the androgen receptor (AR) is also a potential drug target in breast cancer treatment. Whole-body imaging can provide information across lesions within a patient. ER expression in tumor lesions can be visualized by 18F-fluoroestradiol (18F-FES) PET, and AR expression has been visualized in prostate cancer patients with 18F-fluorodihydrotestosterone (18F-FDHT) PET. Our aim was to assess the concordance between 18F-FDHT and 18F-FES PET and tumor AR and ER expression measured immunohistochemically in patients with metastatic breast cancer. Methods: Patients with ER-positive metastatic breast cancer were eligible for the study, irrespective of tumor AR status. The concordance of 18F-FDHT and 18F-FES uptake on PET with immunohistochemical expression of AR and ER in biopsies of corresponding metastases was analyzed. Patients underwent 18F-FDHT PET and 18F-FES PET. A metastasis was biopsied within 8 wk of the PET procedures. Tumor samples with more than 10% and 1% nuclear tumor cell staining were considered, respectively, AR- and ER-positive. Correlations between PET uptake and semiquantitative immunohistochemical scoring (percentage positive cells × intensity) were calculated. The optimum threshold of SUV to discriminate positive and negative lesions for both AR and ER was determined by receiver-operating-characteristic analysis. Results: In the 13 evaluable patients, correlation (R2) between semiquantitative AR expression and 18F-FDHT uptake was 0.47 (P = 0.01) and between semiquantitative ER expression and 18F-FES uptake 0.78 (P = 0.01). The optimal cutoff for AR-positive lesions was an SUVmax of 1.94 for 18F-FDHT PET, yielding a sensitivity of 91% and a specificity of 100%; the optimal cutoff was an SUVmax of 1.54 for 18F-FES PET, resulting in a sensitivity and specificity of 100% for ER. Conclusion: 18F-FDHT and 18F-FES uptake correlate well with AR and ER expression levels in representative biopsies. These results show the potential use of whole-body imaging for receptor status assessment, particularly in view of biopsy-associated sampling errors and heterogeneous receptor expression in breast cancer metastases.
The estrogen receptor (ER) is expressed in 75% of the breast carcinomas, which makes patients with such tumors eligible for ER-targeted therapy (1). Although the ER, human epidermal growth factor receptor 2, and progesterone receptor are routinely determined in breast cancer for prognosis and treatment decision making, this is not the case for the androgen receptor (AR). Nevertheless, several studies have shown that the AR is also present in 70%–80% of the breast carcinomas, which offers a potential new treatment strategy with AR-affecting drugs (2).
Patients with metastatic breast cancer received androgens in the first half of the 20th century, with response rates of 19%–36% (3,4). However, side effects of androgens, including hirsutism and lowering of voice, combined with awareness of the conversion of androgens into estrogens resulted in the discontinuation of androgen therapy in breast cancer patients. With several emerging, less toxic AR-targeted therapies for patients with prostate cancer, and the development of resistance to current breast cancer treatment options, AR-targeted therapies in breast cancer have reentered clinical trials.
A challenge in this era of rapidly emerging drug targets and treatment options is to administer the right drug to the right patient. It is well recognized that only those patients with ER-expressing tumors can benefit from endocrine therapies (1). Because the ER is functionally and structurally highly comparable to the AR, response to AR-targeting drugs may also rely on AR expression in the tumor.
Standard immunohistochemical staining of the primary tumor is inexpensive, easy to apply, and well established in decision making for adjuvant therapies. However, discordant ER expression between the primary breast tumor and metastases has been observed in 18%–40% of the patients (5–8). Molecular imaging offers the possibility to noninvasively determine the presence of relevant drug targets in all metastases within an individual patient. Tumor ER expression can be visualized by 18F-fluoroestradiol (18F-FES) PET in breast cancer patients (9). AR expression in prostate cancer patients has been evaluated using 18F-fluorodihydrotestosterone (18F-FDHT) PET (10,11). If 18F-FDHT PET is also able to determine the AR status in metastatic breast cancer patients, this technique has the potential to select patients eligible for AR-targeted therapies. The aim of the present study was to assess whether uptake on 18F-FES and 18F-FDHT PET correlates with levels of both ER and AR expression on a simultaneous biopsied metastasis.
MATERIALS AND METHODS
Patients
Postmenopausal patients with metastatic breast cancer with previous ER-positive primary tumor were eligible if they had a metastasis outside the liver that was safe to biopsy. Patients were staged with full-body bone scintigraphy (bone scan) and a contrast-enhanced CT scan (chest/abdomen) within 6 wk before the PET examinations. A tumor biopsy was performed within 8 wk of the PET examinations. Exclusion criteria for the study were the use of ER ligands less than 6 wk before entering the study, and a life expectancy of less than 3 mo. Aromatase inhibitors and chemotherapy were allowed. All patients gave written informed consent before study participation, according to the Declaration of Helsinki, and the protocol was approved by the local Ethical Committee (EudraCT no., 2012-003981-42)
Study Design
We performed a prospective, 2-center feasibility trial (NCT01988324). The primary endpoint was the concordance of 18F-FDHT and 18F-FES uptake with, respectively, AR and ER expression in a newly obtained biopsy of a metastasis measured by immunohistochemistry. Secondary endpoints were the optimum threshold to discriminate positive and negative lesions for both AR and ER on PET, inter- and intrapatient 18F-FDHT and 18F-FES heterogeneity, and correlation between tracer uptake and serum hormone levels at the time of scanning. Venous blood was collected before 18F-FES tracer injection to evaluate serum estradiol (luminescence immune assay), luteinizing hormone, follicle-stimulating hormone (both fluorescence immune assay), and sex hormone–binding globulin (chemiluminescence microparticle immune assay). These have been reported to affect tumor 18F-FES uptake in breast cancer studies (12). Before 18F-FDHT injection, blood was collected for serum testosterone and dihydrotestosterone levels (both liquid chromatography-mass spectrometry assay).
Tumor Histology
All patients underwent a biopsy of a metastasis, detectable by conventional imaging, within 8 wk of the PET procedures. Biopsies were formalin-fixed and paraffin-embedded. Biopsies were centrally revised by a dedicated breast pathologist. ER (CONFIRM anti-Estrogen Receptor [SP1] Rabbit Monoclonal Primary Antibody; Ventana) and AR (anti-Androgen Receptor [SP107] Rabbit Monoclonal Primary Antibody; Ventana) were stained with a Benchmark automated stainer (Ventana) at the Department of Pathology of the University Medical Center Groningen. Antibodies were prediluted by the supplier. ER was scored according to the guideline of the American Society of Clinical Oncologypathologists (13) and semiquantitatively: the percentage of positive tumor nuclei was multiplied by the intensity of staining (0, negative; 1, weak; 2, moderate; and 3, strong). This led to a score of 0–300 (14). Because AR is not a routine staining in breast cancer, a threshold of more than 10% positive nuclear staining was used as a discriminator for AR positivity, based on current use in literature (2).
Imaging
CT scans were evaluated by a radiologist. Bone scans were evaluated by 2 nuclear physicians. All tumor lesions visible on CT (>1 cm) and bone scans were documented. Patients underwent 18F-FDHT PET and 18F-FES PET on separate days within 14 d. 18F-FES and 18F-FDHT were produced as described previously (15,16). Patients received approximately 200 MBq of 18F-FDHT and 18F-FES. Whole-body PET/CT was performed 60 min after tracer injection with a Siemens 64-slice mCT (PET/CT) (University Medical Center Groningen) or a Philips Gemini 64 TF PET/CT camera (VU University Medical Center) using the European Association of Nuclear Medicine Research Limited (EARL)–approved protocols (17). Low-dose CT (for attenuation and scatter correction) and PET imaging were performed within 1 procedure. All images were reconstructed according to the specifications of the EARL accreditation program (17).
Tumor 18F-FES uptake was quantified for all lesions seen on CT and bone scans, as well as for nonphysiologic uptake visible above background with an SUVmax of greater than 1.5 based on previous studies (18,19). All lesions detected on bone, CT, and 18F-FES PET scans were also quantified on the 18F-FDHT PET scan. In line with previous studies, we used the SUVmax to calculate tumor 18F-FDHT and 18F-FES uptake (18,19). We also measured the SUVmean using a 50% isocontour of the hottest pixel to assess the average SUV computed in the volume of interest. The SUVpeak was used to calculate uptake in a 1-cm3 spheric volume of interest surrounding the voxel with the highest activity. Background correction was applied using a volume of interest at the unaffected contralateral site whenever available, or at the surrounding tissue of the same origin and deducted from the SUV of the tumor (i.e., lesion SUVmax/mean/peak minus background SUVmax/mean/peak, resulting in background corrected SUVmax/mean/peak.
Statistical Analysis
18F-FDHT PET/CT and 18F-FES PET/CT findings were compared with immunohistochemical findings for AR and ER expression, respectively. The optimum threshold of SUV to discriminate positive and negative lesions for both AR and ER was determined by receiver-operating-characteristic analysis. Correlations between semiquantitative receptor analysis and SUV were calculated using the Pearson correlation coefficient. A P value of 0.05 or less was considered significant.
RESULTS
Patient Characteristics
Twenty-one patients were included between September 2014 and August 2015 (Table 1), and 13 were evaluable for the primary study endpoint. Nonevaluable were 5 patients with a nonvital tumor biopsy (24%), and 3 patients (14%) with biopsied lesions not visible on conventional imaging or PET (n = 2 skin lesions, n = 1 intestinal lesion). All evaluable patients had an ER-positive and AR-positive primary breast cancer based on immunohistochemistry. Three patients (23%) showed conversion between the primary tumor and the metastasis of either ER (8%), AR (8%), or both (8%) measured with immunohistochemistry.
Patient Characteristics
Concordance Between SUV and Immunohistochemistry of Same Tumor Lesion
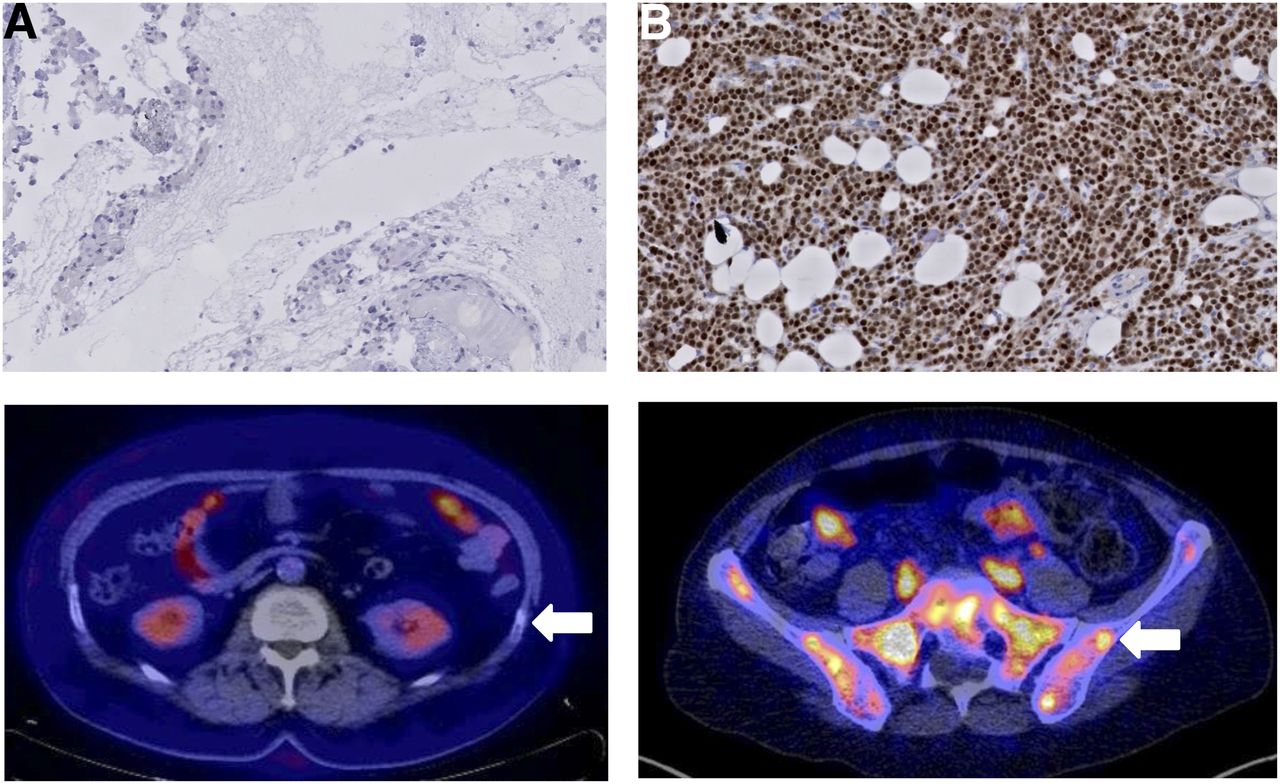
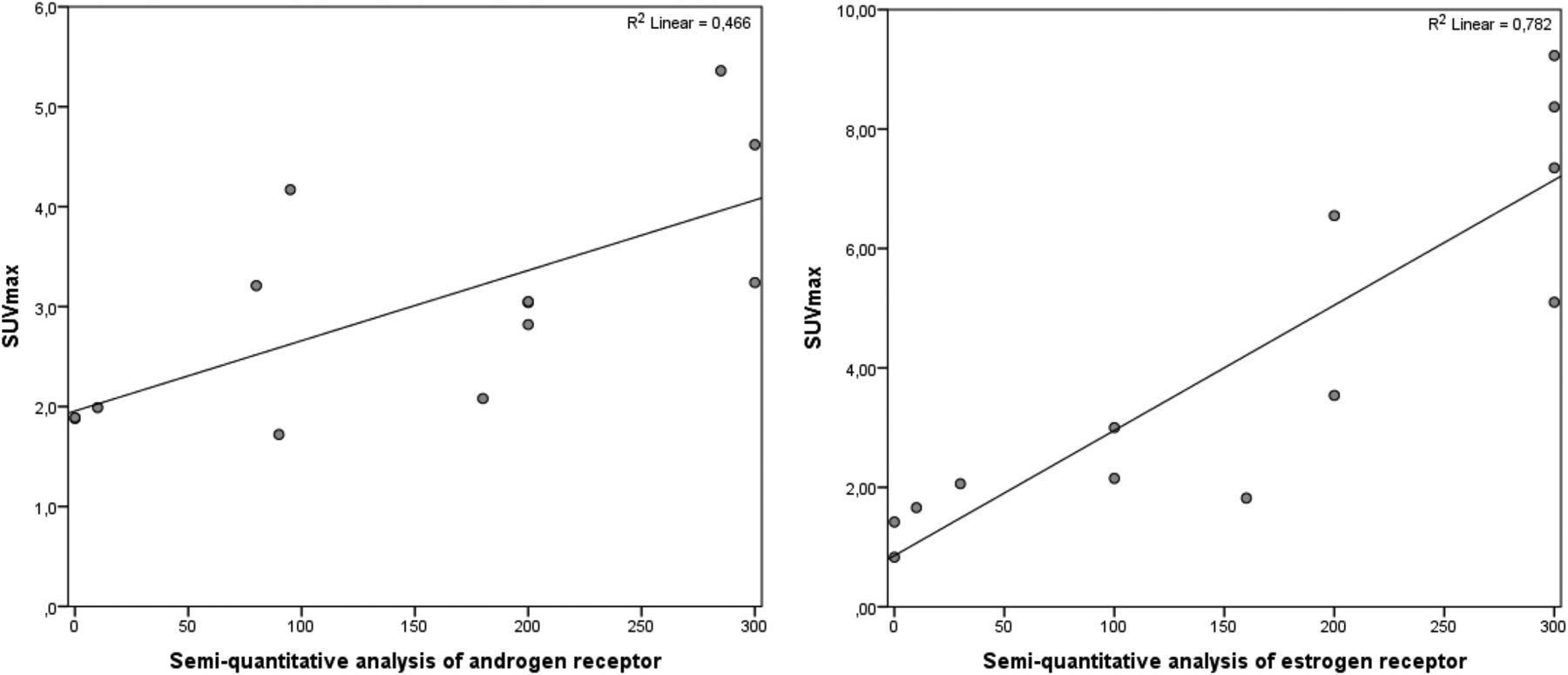
Figure 1 shows 2 representative examples of AR immunohistochemical staining results and corresponding 18F-FDHT PET scans. Mean 18F-FDHT SUVmax of the biopsies in AR-positive lesions was 3.1 (SD, 0.90) versus a mean 18F-FDHT SUVmax in AR-negative lesions of 1.9 (SD, 0.01). Mean 18F-FES SUVmax of the biopsied ER-positive lesions was 4.3 (SD, 2.4) versus a mean 18F-FES SUVmax in biopsied ER-negative lesions of 1.1 (SD, 0.4). The correlation between semiquantitative AR expression and 18F-FDHT uptake was R2 = 0.47 (P = 0.01), and between semiquantitative ER expression and 18F-FES uptake it was R2 = 0.78 (P = 0.01) (Fig. 2). The correction for background uptake did not improve the correlation between semiquantitative AR and ER expression and 18F-FDHT and 18F-FES uptake, because background correction resulted in a correlation of R2 = 0.39 and 0.78, respectively. The correlations between immunohistochemistry and SUVpeak, SUVmean, and background-corrected SUVpeak and SUVmean did not differ from the correlations observed between immunohistochemistry and SUVmax (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org).
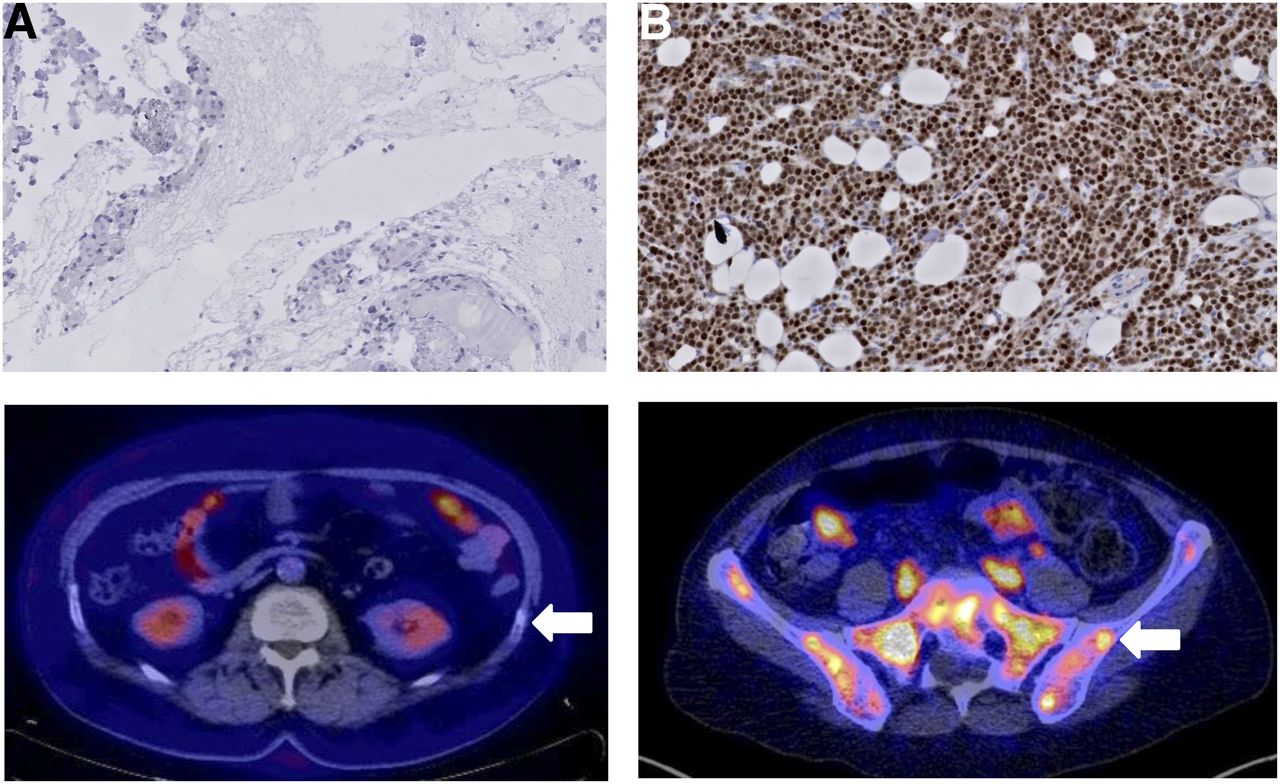
Comparison of immunohistochemistry staining of AR between an AR-negative (0% AR staining) lesion (A, top) and AR-positive (100% staining) lesion (B, top). (Bottom) Horizontal 18F-FDHT PET/CT fusion images. (A, bottom) Physiologic uptake in small intestines and kidneys. Arrow indicates biopsied lesion (rib) with no visual enhanced uptake. (B, bottom) Physiologic uptake in small intestines and high uptake throughout pelvic bones. Arrow indicates biopsied lesion in iliac bone with visually enhanced uptake.
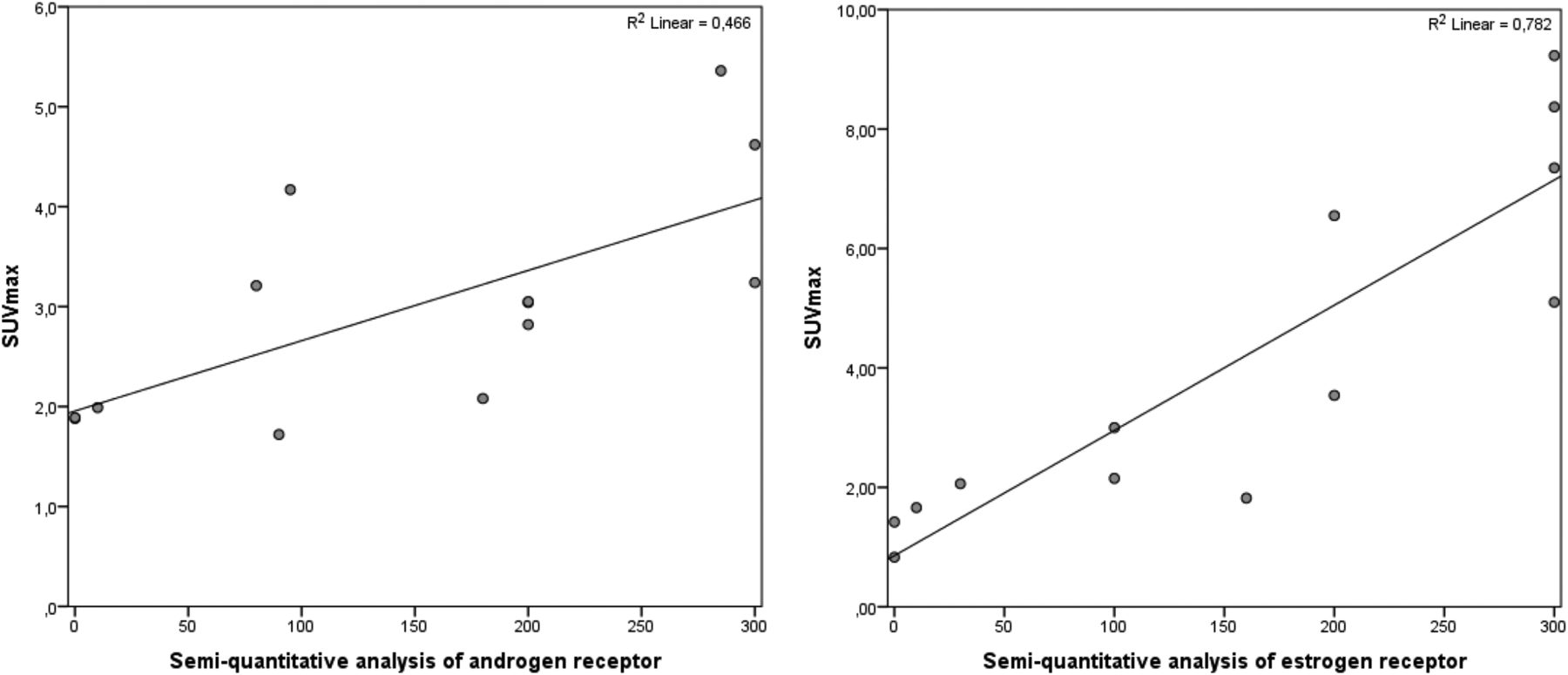
Correlation plot of semiquantitative analysis of receptor status and SUVmax as measured by PET scan for AR (left) and ER (right).
The optimal SUVmax cutoff for 18F-FDHT PET was 1.9, leading to a sensitivity of 91% and a specificity of 100% (area under the curve, 0.91; 95% confidence interval, 0.74–1.0). Receiver-operating-characteristic analysis showed an optimal cutoff value for 18F-FES PET to be SUVmax 1.5, resulting in a sensitivity and specificity of 100%. The correction of tracer uptake for background or using SUVmean or SUVpeak instead of SUVmax did not improve the results (Supplemental Table 2).
Heterogeneity in Uptake
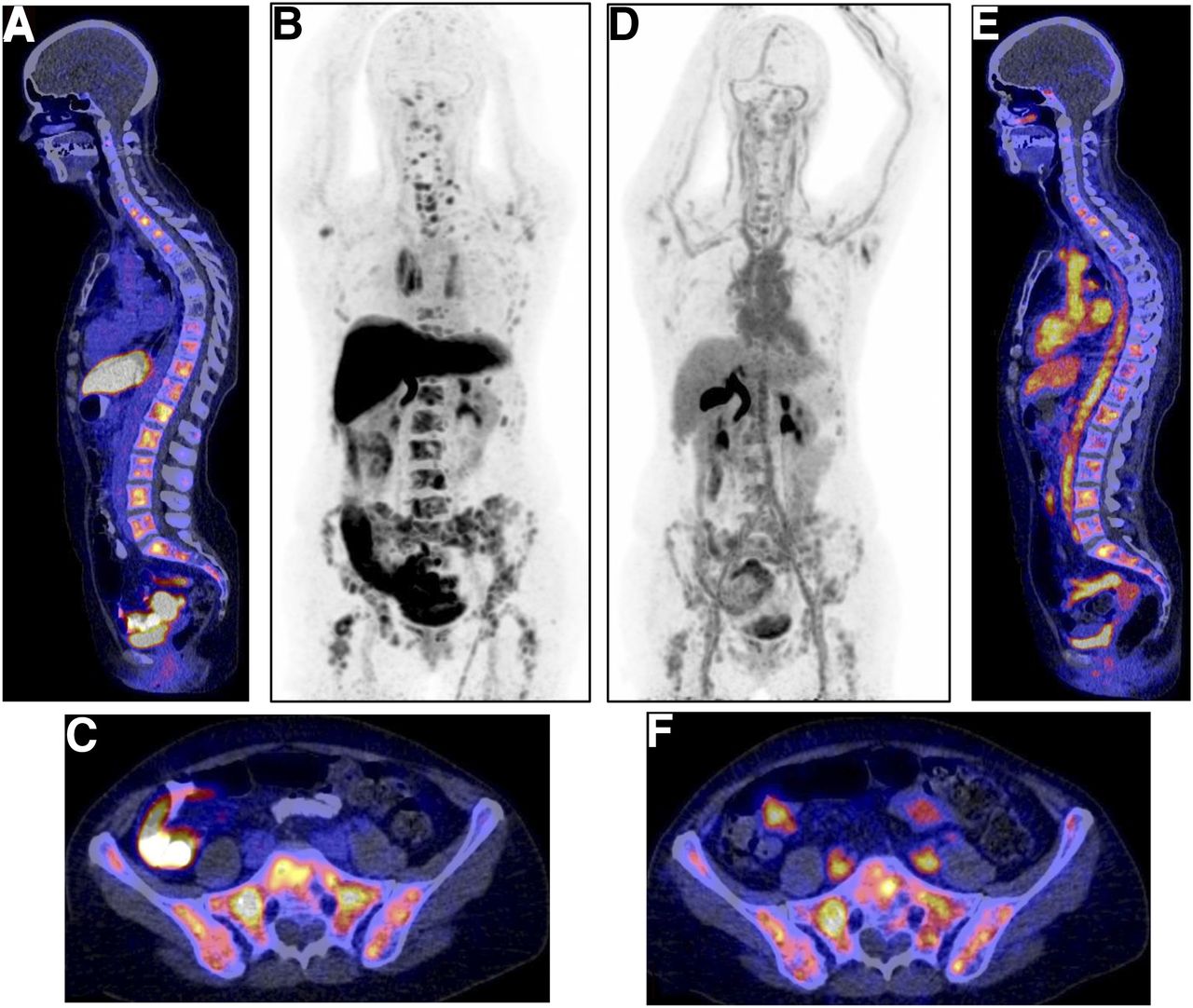
Heterogeneity in lesion uptake was seen between patients and across lesions within individual patients for both 18F-FES and 18F-FDHT uptake. An example of a typical 18F-FDHT and 18F-FES PET is shown in Figure 3. With the cutoff at 1.9 for 18F-FDHT PET, all patients had both 18F-FDHT–positive and 18F-FDHT–negative lesions. SUVmax on 18F-FDHT for tumor lesions varied within patients (median, 2.8; range, 0.8–6.5) and between patients (median, 2.7; range, 1.7–3.7). Eleven of 13 patients had visually both 18F-FES–positive and 18F-FES–negative lesions. SUVmax on 18F-FES PET varied widely between lesions (median, 3.2; range, 0.6–12.2) and patients (median, 2.4; range, 1.3–6.0).

Example of typical 18F-FES (A–C) and 18F-FDHT (D–F) distribution in same patient with multiple bone metastases. (A) Sagittal 18F-FES PET/CT fusion image with physiologic uptake in liver, small intestine, and urinary tract and pathologic uptake in multiple vertebra. (B) 18F-FES PET maximum-intensity-pixel format to allow visualization of biodistribution of 18F-FES tracer. (C) Horizontal 18F-FES PET/CT fusion image with physiologic uptake in small intestine and pathologic uptake throughout pelvic bones. (D) Maximum-intensity-pixel format of 18F-FDHT PET scan, with physiologic uptake in blood pool of heart and liver and excretion via bile to small intestine, and urinary tract. (E) Sagittal 18F-FDHT PET/CT fusion image with physiologic uptake and pathologic uptake in multiple vertebrae. (F) Horizontal 18F-FES PET/CT fusion image with physiologic uptake in large vessels and small intestines and pathologic uptake throughout pelvic bones.
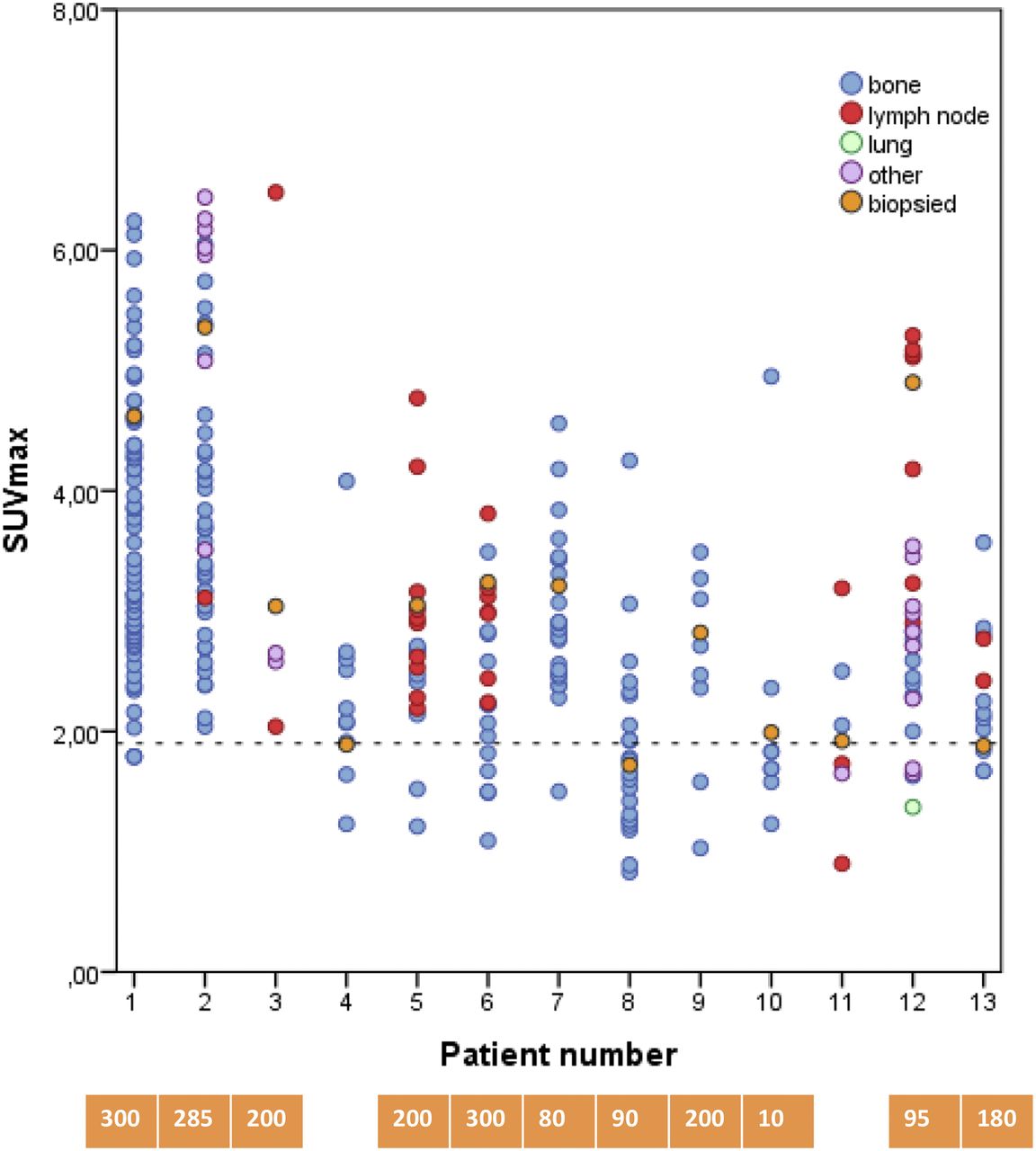
A total of 298 lesions were detected with CT scans (n = 95), bone scans (n = 126), or 18F-FES PET scans (n = 239). Most lesions (81%) showed uptake above background on 18F-FES PET. CT or bone scan identified 59 lesions that showed no 18F-FES uptake above background. 18F-FES PET identified 48 lesions not visible on conventional imaging. In total, 278 lesions could be used for 18F-FES PET analysis. Because of the high physiologic background uptake near the lesion such as in the liver and intestines, 20 lesions could not be reliably quantified. Most of the lesions were in the bone (n = 219); 34 lesions were in the lymph nodes, and 25 were visceral lesions (Fig. 4).

Distribution of SUVmax per lesion per patient measured by 18F-FES PET. Lesions are divided into bone (blue), lymph nodes (red), lung (green), and others (purple). Orange circles are biopsied lesions. Blue boxes indicate ER-positive biopsies (>1% staining); numbers indicate score of biopsy (i.e., intensity times percentage positive cells). Dashed line indicates threshold set based on receiver-operating-characteristic analysis. White boxes indicate negative biopsies (<1% staining).
On 18F-FDHT PET scans, 196 lesions (66%) were visible above background, of which 42 lesions could not be reliably quantified because of high physiologic background uptake near the lesion (e.g., the liver, blood vessels, and intestines). One hundred two lesions were not visible above background but were visible on either CT scan, bone scan, or 18F-FES PET scan. In total, 256 lesions were included for 18F-FDHT PET analysis. Most of the lesions were bone lesions (n = 222), 14 lesions were lymph nodes, and the remaining 20 lesions were visceral lesions (Fig. 5).
Distribution of SUVmax per lesion per patient measured by 18F-FDHT PET. Lesions are divided into bone (blue), lymph nodes (red), lung (green), and others (purple). Orange circles are biopsied lesions. Orange boxes indicate AR-positive biopsies (i.e., >10% staining); white boxes indicate negative biopsies. Numbers in boxes indicate score of biopsy (i.e., intensity times percentage positive cells). Dashed line indicates threshold set based on receiver-operating-characteristic analysis.
Uptake in healthy liver tissue was high on both 18F-FDHT PET and 18F-FES PET scans, rendering analysis of liver metastases impossible. The mean liver uptake on 18F-FDHT SUVmean was 4.4 (range, 3.6–5.8) versus the mean liver uptake on 18F-FES SUVmean of 12.8 (range, 8.2–19.6). Several lesions were nonquantfiable due to high blood-pool accumulation on the 18F-FDHT PET. The blood-pool accumulation measured in the descending thoracic artery was higher on 18F-FDHT PET than 18F-FES PET: SUVmean of 4.6 (range, 3.8–6.2) versus SUVmean of 1.3 (range, 0.9–2.1), respectively.
Correlation Between PET Uptake and Serum Hormone Levels and Sex Hormone–Binding Globulin
18F-FDHT tumor uptake did not correlate with serum sex hormone–binding globulin, DHT, or testosterone levels (Supplemental Tables 3–5). Serum estradiol levels correlated positively with18F-FES tumor uptake (R2 = 0.52; P = 0.01). 18F-FES tumor uptake did not correlate with sex hormone–binding globulin, luteinizing hormone, or follicle-stimulating hormone serum levels.
DISCUSSION
This is the first study in which the 18F-FDHT uptake is evaluated in breast cancer patents and in which 18F-FDHT tracer uptake was correlated with semiquantitative AR analysis in a biopsy of the corresponding metastasis. 18F-FDHT uptake shows a moderate correlation with AR expression, and 18F-FES uptake shows a strong correlation with ER expression.
In this study, we showed that 18F-FDHT can identify AR-positive metastases in breast cancer patients. 18F-FDHT PET may therefore be an interesting tool to select patients eligible for clinical trials with AR antagonists and to analyze the receptor occupancy of these drugs. AR-targeted therapy is not yet standard in breast cancer patients, but preliminary results of phase II trials are promising, with stable disease in 35% of metastatic breast cancer patients (20,21). More clinical studies exploring the efficacy of AR-targeted therapy in AR-positive metastatic breast cancer are currently ongoing (e.g., NCT00468715, NCT00755885). Even combined AR- and ER-targeted therapies are currently under way (NCT02910050, NCT02953860).
To date 18F-FDHT PET has been used only in trials with metastatic prostate cancer patients. A comparison of 59 metastatic prostate cancer lesions visible on conventional imaging showed that 97% were also visible on the 18F-FDHT PET (10). Here, conventional imaging also included 18F-FDG PET. In our study, we found that 66% of the lesions visible on conventional imaging were visible on 18F-FDHT PET.
With serial 18F-FES PET scans in patients treated with ER modulators such as fulvestrant, we were able to visualize residual ER availability during therapy, which was associated with early progression (22). For other ER modulators such as GDC0810 and Z-endoxifen, 18F-FES PET provided information about ER occupancy and guided dose selection for phase II trials (23,24). 18F-FDHT uptake in tumor lesions of patients with prostate cancer diminished in 3 patients after treatment with a high dose of testosterone. Treatment with the AR blocker enzalutamide also resulted in a reduced uptake on 18F-FDHT PET in prostate cancer patients (10). We are currently investigating the effect of the AR blocker bicalutamide on residual AR availability assessed by 18F-FDHT PET in patients with metastatic breast cancer. Secondary endpoints are the relation between percentage decreased uptake on 18F-FDHT PET and response to treatment measured by RECIST in the case of measurable disease (NCT02697032).
This study enforces the earlier observed correlation between 18F-FES uptake and ER expression. Correlations between the 18F-FES PET uptake parameters and immunohistochemistry on the metastatic biopsy using an SUVmax of greater than 1.5 showed a 100% sensitivity and specificity similar to previously published results (9,18,19). The parameters SUVmax, SUVmean, and SUVpeak did not differ, and correction for background did not influence the correlation. Therefore, for 18F-FES PET analysis in the diagnostic setting SUVmax can be used, and correction for background is not required. The correlation between uptake on 18F-FDHT PET scans and immunohistochemical staining was lower than on 18F-FES PET and immunohistochemical staining. The kinetic properties and metabolism of 18F-FES and 18F-FDHT are similar (25,26). But 18F-FDHT has a lower relative binding affinity of 0.43 for AR than FES, which has a binding affinity of 0.83 for ER (21). Furthermore, SUV might not be the best quantification method for 18F-FDHT uptake. In a small study with 4 metastatic prostate cancer patients, SUV corrected for plasma 18F-FDHT concentration showed a better correlation (27).
We analyzed factors that potentially could influence tracer uptake such as circulating hormone levels. We found only estradiol levels to be correlated with higher uptake on 18F-FES PET scans, which might be related to higher ER expressions in tumor lesions in postmenopausal patients with higher residual estradiol levels. In fact, we found a correlation of R2 of 0.42 (P = 0.02) between serum estradiol levels and ER expression determined by immunohistochemical staining on a metastasis biopsy. There was no correlation between other serum hormone levels and 18F-FES or 18F-FDHT tumor uptake. These data indicate that physiologic circulating hormone levels are too low to directly affect tracer uptake in the tumor. Tracer uptake can be influenced by volume, that is, partial-volume effect, where smaller tumor sizes results in an underestimation of uptake (28). However, in our study there was no correlation found between the volumes of interest of the lesions and 18F-FES or 18F-FDHT uptake.
Because of the feasibility setting of this study, only a limited number of patients were evaluable for primary endpoint. Therefore, larger studies should confirm the optimal cutoff value for 18F-FDHT PET. In our study, 5 of the 21 entered patients did not have vital tumor tissue in their metastatic biopsies. CT may have also shown bone lesions that were no longer active, as patients were heavily pretreated. This might have resulted in an overestimation of 18F-FES– and 18F-FDHT–negative sites. Others have used 18F-FDG PET to visualize hormone receptor–negative lesions. We refrained from doing so, because 18F-FDG PET can also be negative in hormone receptor–positive breast cancer lesions (29). PET imaging of hormone receptors also has some restrictions. Liver lesions are nonevaluable by 18F-FES and 18F-FDHT PET because of high uptake of both tracers in the liver. In addition, 18F-FDHT PET has the disadvantage of high accumulation in the blood pool, rendering it difficult to analyze lesions near large veins. This has also been described in a 18F-FDHT PET study in prostate cancer patients (9). If the 18F-FDHT PET would be used as a diagnostic tool, this would be complementary to the current conventional imaging.
CONCLUSION
In our heavily pretreated patient population, hormone receptor conversion in the metastasis, when compared with the primary tumor, occurred in 23% of the patients. This is similar to previously reported conversion rates (7,8). Heterogeneous uptake in tumor lesions on both 18F-FES and 18F-FDHT PET was seen in most patients, suggesting that both receptor-positive and -negative lesions are present in 1 patient. Current guidelines advise on a biopsy being performed when metastatic disease presents. This may not always be feasible. However, when omitted, changes in receptor status over time might lead to suboptimal therapy choices. 18F-FDHT and 18F-FES PET have the potential to serve as a surrogate for metastasis biopsy, especially when lesions are difficult to access or sampling errors are prone to occur.
DISCLOSURE
This work was supported by CTMM-MAMMOTH WP5, the Alpe d’HuZes/Dutch Cancer Society (RUG 2013-5960), the Ubbo Emmius Fund grant (510215), the van der Meer-Boerema Foundation, and the Anna Dorothea Hingst Foundation. No other potential conflict of interest relevant to this article was reported.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication March 29, 2017.
- Accepted for publication April 24, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Report on the PET/CT Image-Based Radiation Dosimetry of [18F]FDHT in Women, a Validated Imaging Agent with New Applications for Evaluation of Androgen Receptor Status in Women with Metastatic Breast Cancer
- Report on the PET/CT Image-Based Radiation Dosimetry of [18F]FDHT in Women, a Validated Imaging Agent with New Applications for Evaluation of Androgen Receptor Status in Women with Metastatic Breast Cancer
- Summary: Appropriate Use Criteria for Estrogen Receptor-Targeted PET Imaging with 16{alpha}-18F-Fluoro-17{beta}-Fluoroestradiol
- Imaging Androgen Receptors in Breast Cancer with 18F-Fluoro-5{alpha}-Dihydrotestosterone PET: A Pilot Study
- Breast Cancer: Evaluating Tumor Estrogen Receptor Status with Molecular Imaging to Increase Response to Therapy and Improve Patient Outcomes
- Recent Advances in Imaging Steroid Hormone Receptors in Breast Cancer