


Abstract
The purpose of this study was to investigate and assess the correlation and reproducibility of multiparametric imaging in head and neck cancer patients. Methods: Twenty-one patients were included in this prospective scan–rescan study. All patients were scanned twice on an integrated PET and MRI scanner. Gross tumor volumes were defined on T2-weighted MR images, and volumes of interest were defined on diffusion-weighted MRI and 18F-FDG PET (VOIDWI, VOIPET). Overlap between volumes was assessed as a percentwise overlap. 18F-FDG uptake and diffusion were measured using SUV and apparent diffusion coefficient, and correlation was tested across and within patients and as a voxel-by-voxel analysis. Results: Seventeen patients were available for correlation analysis, and 12 patients were available for assessment of tumor overlap. The median tumor overlap between VOIDWI and VOIPET was 82% (VOIDWI in VOIPET) and 62% (VOIPET in VOIDWI) on scan 1 and scan 2, respectively. Across patients, the correlation between SUV and apparent diffusion coefficient was weak and nonsignificant. However, in individual patients a weak but significant correlation was identified on a voxel-by-voxel basis. Conclusion: In multiparametric imaging with the integrated PET/MR scanner, the VOIs from DWI and 18F-FDG PET were both within the target volume for radiotherapy and overlapped substantially although not completely. No correlation between 18F-FDG uptake and DWI could be found across patients, but within individual patients a statistically significant, but weak, voxel-by-voxel correlation was found. The findings suggest that information on glucose uptake and diffusion coefficient carries complementary information of interest that may be relevant for radiotherapy treatment planning.
The concept of personalized medicine has brought increased awareness to inter- and intratumor heterogeneity (1), and the evidence supporting the importance of considering tumor heterogeneity in therapy planning is increasing (2–4). Single tumor biopsies cannot detect all intratumor heterogeneity, and it is not realistic to perform multiple biopsies of individual tumors or to biopsy all lesions in individual patients with metastatic disease in an attempt to assess intra- or intertumor heterogeneity. Therefore, a new diagnostic method, which can provide a more comprehensive view of the tumor biology, including intratumor heterogeneity, is warranted. Tumor heterogeneity can now be investigated with multiparametric imaging (5,6), and in this respect hybrid-imaging with PET/MR (integrated PET and MRI) provides a promising and noninvasive alternative (7–9).
Squamous cell carcinoma of the head and neck (HNSCC) is a heterogeneous disease (10–12), and with the introduction of PET/MR imaging it is now possible to assess some of this heterogeneity by comparing 2 functional imaging techniques simultaneously on a voxel-by-voxel basis. For example, comparisons can be made between diffusion-weighted imaging (DWI) and 18F-FDG, both of which can be quantified, DWI as apparent diffusion coefficient (ADC) and 18F-FDG uptake as the SUV.
Low ADC and high SUV have both been reported to correlate with poor patient outcome (13,14). DWI and 18F-FDG PET can potentially offer complementary information in HNSCC (15,16), and it is hypothesized that biologically different subvolumes can be identified with functional imaging and targeted with radiation dose painting (17). Integrated PET/MR can provide DWI and 18F-FDG uptake, simultaneously reducing misalignment due to time, positioning, and biologic changes, thus allowing assessment of several relevant dose-painting targets and the concordance between such targets. Several studies have stated that ADC and SUV may be important parameters in describing heterogeneity and defining subvolumes within gross tumor volume (GTV) for dose painting. Both PET and DWI may reflect various functional properties of tumor tissue, although this approach obviously requires that the subvolumes are stable over time and lie within the actual target volume. The correlation between ADC and SUV has been explored by several research groups and for various tumor types. In general, there is a consensus that a negative correlation between the minimum ADC value and the SUVmax exists, which can be used to distinguish between benign and malignant tumors (18–20). Schmidt et al. (21) suggested that a voxelwise correlation of ADC and 18F-FDG PET using PET/MR might provide a more sophisticated spatial characterization of tumors, as did Metz et al. in 2015 (22). To the best of our knowledge, this is the first study evaluating the correlation between DWI and 18F-FDG PET on a voxelwise basis as well as scan–rescan stability on an integrated PET/MR scanner in patients with HNSCC.
The hypothesis of this study is that there is a strong and reproducible correlation between 18F-FDG PET and DWI both by ADC/SUV measures and by volume of interest (VOI). Here, strong should be interpreted as a sufficiently reliable correlation to allow assessment of ADC from the SUV in a voxel and vice versa with sufficient accuracy for clinical use. The following 4 specific aims are addressed to test the hypothesis of the study: investigate and quantify the overlap between the tumor volumes defined by DWI and 18F-FDG PET images simultaneously on an integrated PET/MR scanner and report the reproducibility, investigate the correlation between 18F-FDG uptake (SUV) and ADC across patients, investigate the voxelwise correlation of 18F-FDG uptake and ADC, and explore the potential of an unsupervised cluster analysis of joint 18F-FDG and ADC data to identify tumor subvolumes.
MATERIALS AND METHODS
Patients
Twenty-one patients were included in this prospective scan–rescan study after written informed consent was obtained. The patients were scanned twice with exactly 3 d between scans. All patients in the present study were from a patient cohort of 30 patients originally included in a study designed to test reproducibility of 18F-FDG uptake on both PET/CT and PET/MR (23). The study was approved by the local ethics committee (approval no. H-3-2012-072).
18F-FDG PET/MR
All patients were scanned on the same integrated PET/MR system (Biograph mMR; Siemens) (24) with a 3-T magnet using a head and neck coil. Patients were instructed to fast for a minimum of 6 h and scanned 100–120 min after injection of 18F-FDG (4 MBq/kg). For the time interval between 18F-FDG injection and time to scan on the second scanning day, we attempted to match the actual time interval on the first scanning day.
PET was performed as a single-bed, 20-min acquisition. PET data were reconstructed using ordinary Poisson ordered-subset expectation maximization with 3 iterations, 24 subsets, and 4 mm gaussian postprocessing filter into 344 × 344 matrices. Resolution modeling (point spread function) was not applied.
A T2-weighted sequence was acquired, followed by a Dixon volumetric interpolated breath-hold examination sequence for attenuation correction. All scans were obtained without a gadolinium contrast agent. The imaging protocol for the DWI consisted of a 2-dimensional echoplanar sequence (echo planar imaging) using a matrix size of 92 × 92 × 24, voxel size of 2.71 × 2.71 × 4 mm, repetition time/echo time of 3,000/84 ms, parallel imaging factor (generalized autocalibrating partial parallel acquisition) of 4, and flip angle of 90°, and was performed in all patients with 3 different b-values (0, 500, 1,000 s/mm2). DWI was measured as 3 stacks, each at isocenter to maximize field homogeneity. DWI had an effective echo spacing of 0.145 ms, and DWI distortions were corrected using the algorithm (FMRIB's Utility for Geometrically Unwarping EPIs [where FMRIB is Oxford Centre for Functional MRI of the Brain] [FUGUE]) of the FSL software package (Analysis Group, FMRIB) (25).
Definitions of VOI
A region of interest covering the primary T site was defined on MR and PET, respectively. The PET images were assessed by a specialist in nuclear medicine, and the 18F-FDG PET–positive tumor volume, that is, VOIPET, was defined and delineated manually. This was done by a visual adaptation of an SUV isocontour starting at 40% of the SUVmax so as to include the steepest gradient of SUV-avid tissue and exclude physiologic 18F-FDG uptake (26).
The DWI was assessed by an MR radiologist. Before the delineation of the VOI defined from DWI (VOIDWI), the PET and anatomic images were assessed to exclude patients with a large signal drop out or other severe artifacts on DWI. An example of signal drop out can be seen in Supplemental Figure 1 (supplemental materials are available at http://jnm.snmjournals.org). The radiologist did not have access to the PET imaging during the actual delineation of the VOIDWI; likewise, the specialist in nuclear medicine did not have access to the MR scan during the delineation.
The definition and delineation of the anatomic GTV on MR (GTVT2) were performed by a radiologist specializing in tumor delineation. The delineation was performed on the T2-weighted images without access to or prior evaluation of the functional images (i.e., both PET and DWI). The tumor volume was delineated as a target volume for radiotherapy, that is, if there was doubt regarding tumor extension it was included in the GTVT2. The MR-defined target volume (GTVT2) was chosen to ensure that the volumes defined from 18F-FDG PET and DWI were within the relevant target volume for radiotherapy.
Analysis of DWI and PET Data
SUV, ADC, and volume metrics were extracted from the software package Mirada XD3 (MIRADA Medical). Tumor volume overlap between the respective imaging modalities was assessed as a percentwise overlap.
In addition, a voxelwise analysis of PET, T2-weighted MR images (T2-MRI), and DWI was executed using MATLAB R2014b (8.4.0.150421; 64 bit [The MathWorks]). PET and T2-MRI were initially resampled to the same dimensions as the ADC sequence (92 × 92 × 24 voxels; voxel spacing, 2.71 × 2.71 × 4 mm) in OsiriX (version 5.7.1; 32 bit), so the dimensions of the PET, T2-MRI, and ADC sequences were all in accordance before a voxelwise analysis. PET and DWI VOIs were imported from Mirada and resampled to the ADC sequence. All voxels present in the delineated VOIs were used in the voxelwise analysis. A gaussian mixture model was used as a data-driven cluster analysis to cluster-specific voxels according to their likelihood of belonging to a certain subvolume (e.g., a multivariate normal distribution), as previously described by Schmidt et al. (21). In our specific context, it was assumed that a small area in the tumor (voxel) belonged to a certain subvolume (e.g., representing underlying biologic tissue characteristics, such as inflammation, necrosis, malignant tissue, benign tissue) defined by a multivariate normal distribution with cluster-specific mean and covariance. On visual assessment, the tumors did not appear heterogeneous and thus the analysis was restricted to search for 2 clusters, and the cluster with the highest SUV was called cluster 2.
Statistical Analysis
Statistical analysis was performed in SPSS (version 19; IBM). The reproducibility of SUV and ADC values was assessed using the paired t test. Correlations between SUVmax and ADCmin and SUVmean and ADCmean, respectively, on both scans were assessed using Pearson correlation. Correlation of the distribution of ADC and SUV in a voxelwise comparison was assessed using Spearman rank correlation.
RESULTS
Patients
Twenty-one patients were scanned twice with PET/MR, as previously described (23). Four patients had to be excluded because of a large signal drop out at the tumor site on the DWI caused by geometric distortion (Supplemental Fig. 1), leaving 17 patients available for further analysis of correlation between SUV and ADC. After the FUGUE correction, no patients had to be excluded because of signal drop out. In 4 other patients, FUGUE correction was not possible in either of the 2 scans and in another 2 patients FUGUE correction was possible only in 1 of the 2 scans, leaving 12 patients available for assessment of tumor overlap between 18F-FDG PET and DWI and for the voxel-by-voxel comparison (11 + 1 with FUGUE correction from the first scan and 11 + the other with FUGUE correction data from the second scan). The reproducibility of tumor overlaps and voxelwise comparison was therefore feasible in 11 patients who had all data available from both PET/MR scans. A flowchart of patient inclusion can be seen in Figure 1, and Table 1 summarizes the number of patients with data available from the first and second scans.

Flowchart of patients included.
Patients with Data Available from First and Second Scan in Regards to PET, ADC, and Postprocessing (FUGUE), Which Is Necessary to Perform Voxel-by-Voxel Comparison
Overlap of Tumor Volumes
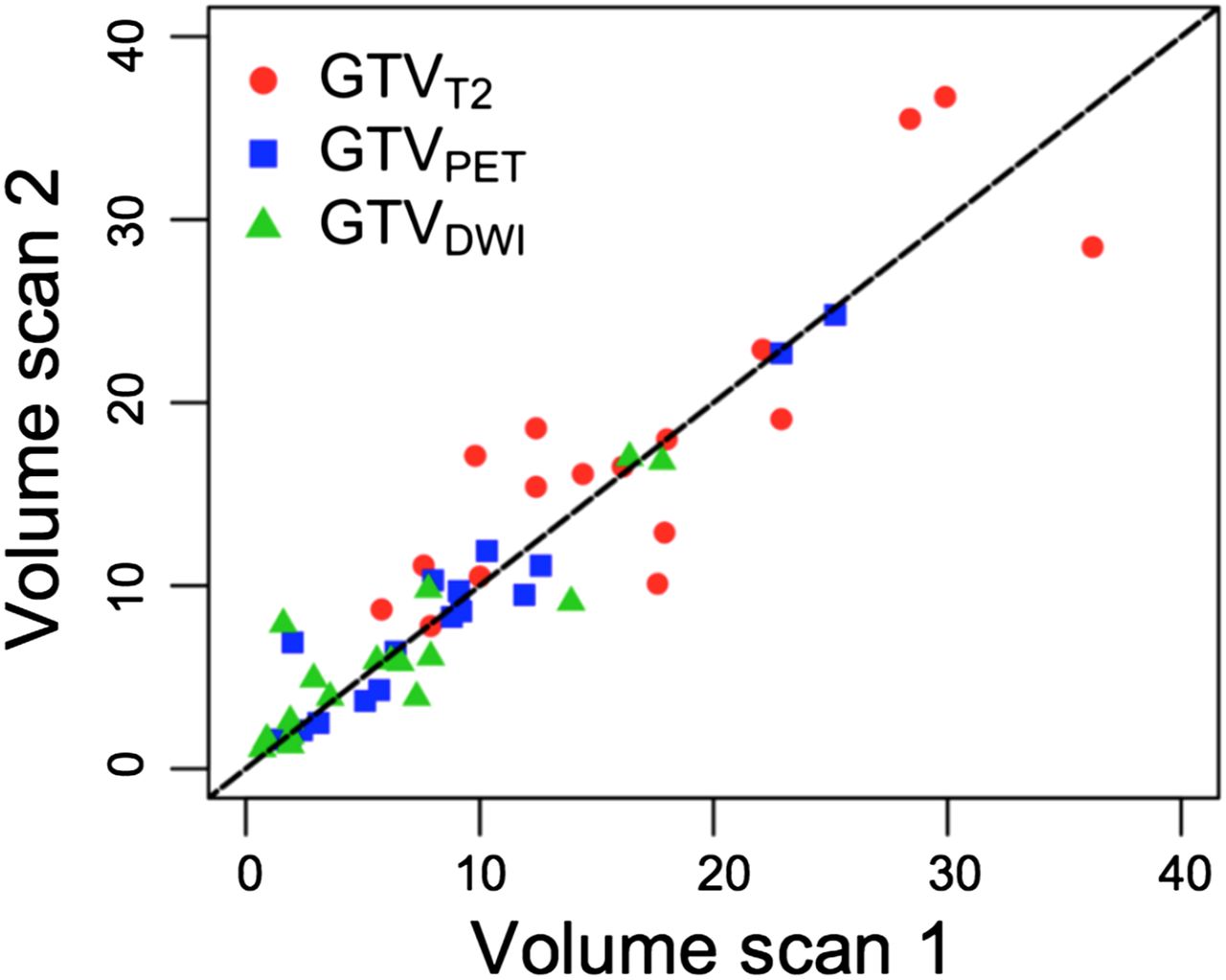
The volumes from the 3 imaging modalities measured on scans 1 and 2, respectively, are illustrated in Figure 2. The median tumor volume and the median tumor overlap between the 3 different imaging modalities can be seen in Table 2. For all cases VOIDWI < VOIPET < GTVT2. As expected, the GTV assessed with both DWI (VOIDWI) and 18F-FDG PET (VOIPET) was encompassed in the anatomically defined tumor volume (GTVT2) on both the first and the second scan, respectively (98% and 99%) (Table 2). In all but 1 case, more than 73% of the tumor volume defined from DWI was encompassed in VOIPET. In the remaining case, only 58% and 48% of VOIDWI was encompassed in VOIPET on the first and second scans, respectively. The median tumor overlap was above 80% (VOIDWI within VOIPET) on both scans 1 and 2 and proved to be reproducible (Table 2). The difference in overlap from scan 1 to scan 2 was small (average 3%). Two examples of mismatch of VOIDWI and VOIPET can be seen in Figure 3: a worst case (Fig. 3A) and a representative case (Fig. 3B). Because of the relatively small tumor volume in this patient, even a small mismatch between T2, DWI, and PET has a relatively large percentwise impact in the overlap analysis.

Tumor volumes measured with VOIDWI, VOIPET, and GTVT2 on the 2 PET/MR scans.
Median Tumor Volume from DWI, 18F-FDG PET, and Anatomic T2-Weighted MR
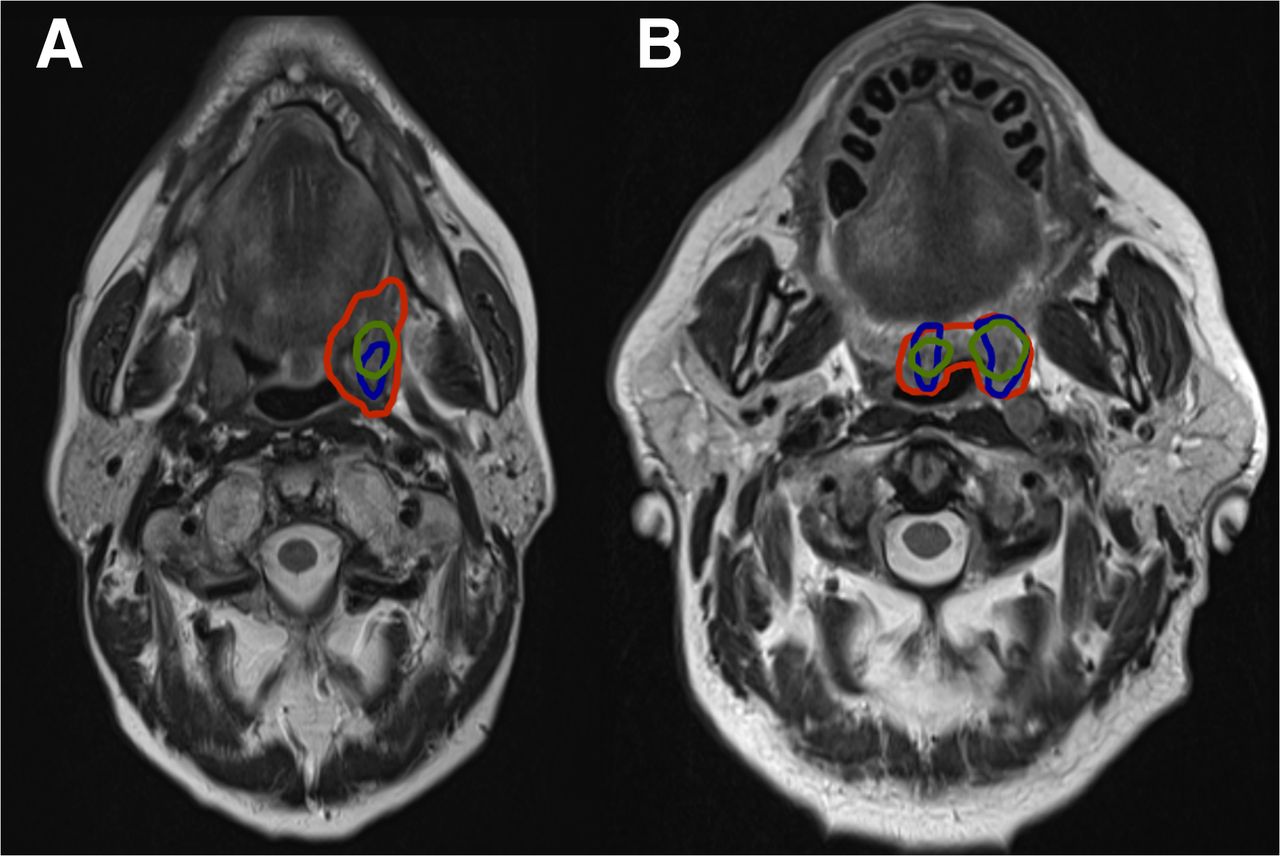
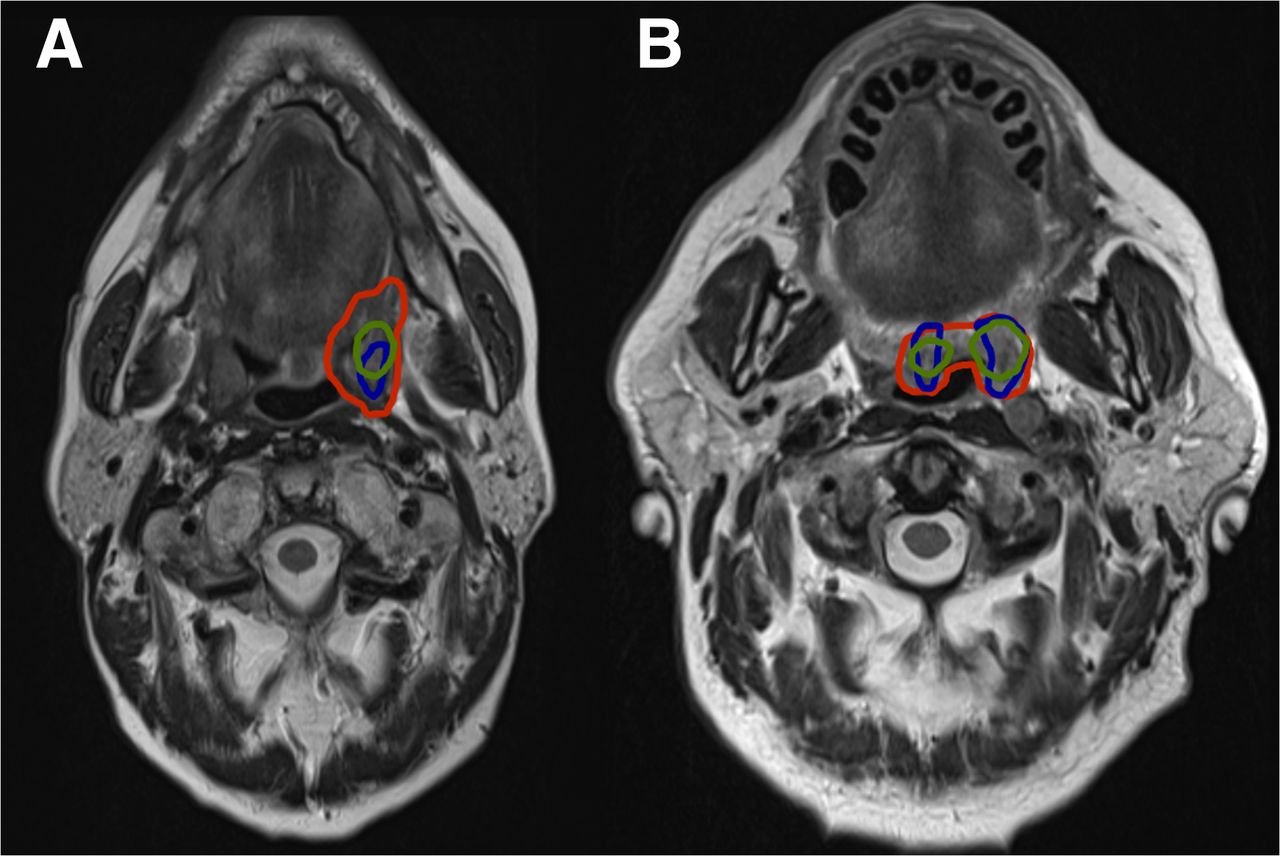
Examples of tumor overlap between tumor defined from DWI (blue contour), 18F-FDG PET/MR (green contour), and T2-weighted MR (red contour). (A) Worst case of overlap between VOIDWI and VOIPET. Forty-two percent of VOIPET is within VOIDWI, and 63% of VOIDWI is within VOIPET. (B) Representative case in which 67% of VOIPET is within VOIDWI, and 68% of VOIDWI is within VOIPET.
Correlation Between SUV and ADC
A scatterplot of SUVmax and ADCmin can be seen in Figure 4, from both the first scan (Fig. 4A) and the second scan (Fig. 4B). There were no significant differences in SUVmax (mean difference, 0.9; P = 0.11) or ADCmin (mean difference, 9.7; P = 0.69) between the first and the second scans. On a tumor basis, the correlation between SUVmax and ADCmin was not significant, with correlation coefficients of −0.26 (P = 0.32) and −0.37 (P = 0.15) on scans 1 and 2, respectively. Similarly, no significant difference between SUVmean and ADCmean was observed (P = 0.9 and 0.5) and the correlation was not significant (−0.05 [P = 0.85] and −0.39 [P = 0.13]).

Scatterplot of SUVmax and ADCmin from first scan (A) and from second scan (B). Data are fitted to linear model, and laid over with 95% confidence interval (blue).
The correlation between ADC and SUV on a voxelwise level was significantly negative in 9 of 12 patients on the first scan. However, the correlation coefficients were small, suggesting only a weak correlation (mean correlation coefficient ρ, −0.23 [range, −0.63 to 0.31]) including data from all 22 scans).
Cluster Analysis
The voxel-by-voxel comparison and the cluster analysis proved feasible and in most of the 11 cases reproducible (assessed visually). All results can be seen in Table 3 and in the supplemental materials (Supplemental Fig. 2).
Overlap Between the 2 Clusters and VOI Defined from DWI and 18F-FDG PET/MR Is Reported in Percentage
Cluster 2 (red) encompassed most of the VOIPET (median overlap of 91% and 97% on the first and second scans, respectively) and most VOIDWI (median overlap of 65% and 52% on the first and second scan, respectively). Likewise, cluster 1 encompassed only a small part of VOIDWI and VOIPET on both scans (Table 3). In most but not all patients, separation between clusters appeared to be defined by an SUV threshold and hence not dependent on ADC (Supplemental Fig. 2).
In Figure 5, slices from the PET and the DWI scans from the same 2 patients as in Figure 3 as well as the correlation plots from the voxel-by-voxel analysis can be seen. The representative overlap case (Figs. 5E–5H) has clusters defined primarily by an SUV around 6. For the poor overlap case (Figs. 5A–5D), conversely, the clusters are not separated by a single SUV but depend on both SUV and ADC in a nontrivial manner.
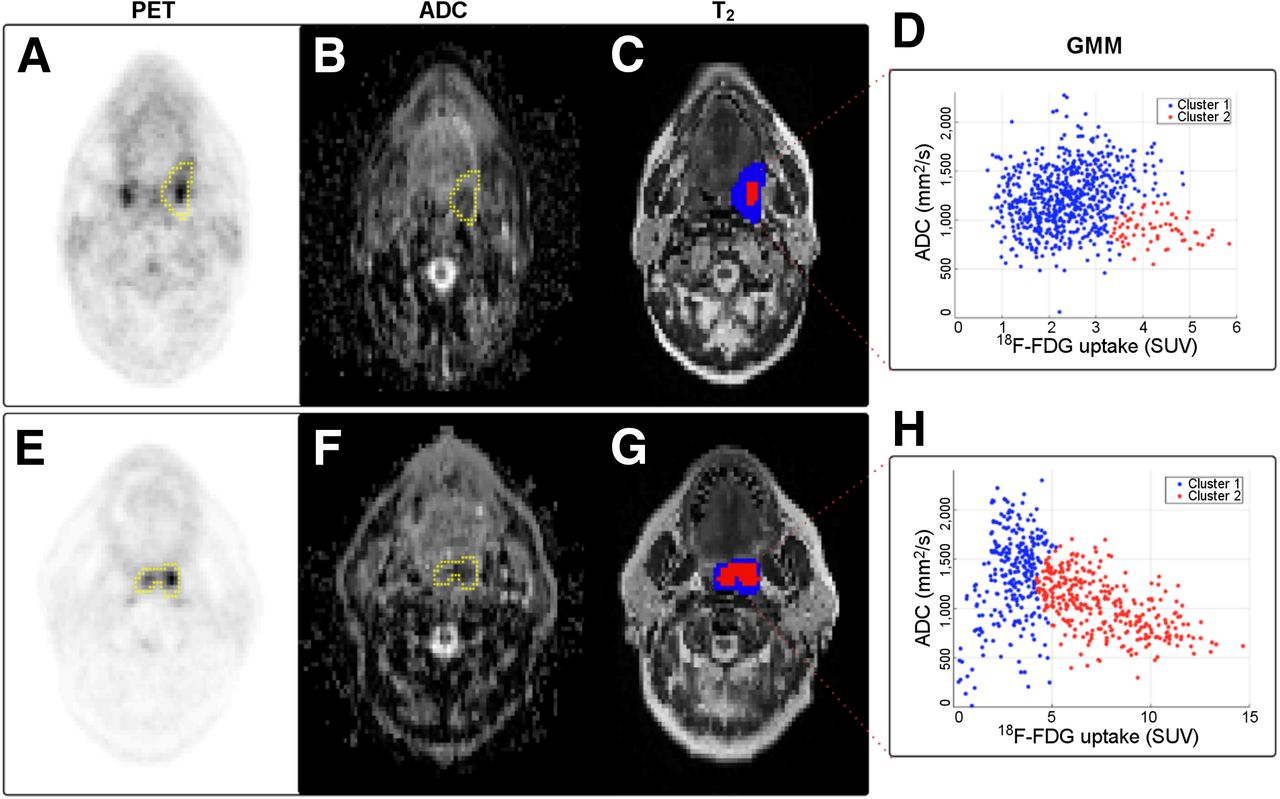
PET image (A), image from ADC map (B), and T2-weighted image (C) from patient in Figure 3A (poor overlap case). Yellow contour represents GTVT2. (D) Scatterplot from voxel-by-voxel analysis showing respective clustering assignment from cluster analysis. PET image (E), ADC map (F), and T2 image (G) for patient in Figure 3B (representative overlap case). (H) Scatterplot and clustering assignment from cluster analysis.
DISCUSSION
The tumor overlap between VOIDWI and VOIPET was not complete but substantial and reproducible, with most VOIDWI encompassed in VOIPET (>80%) and most VOIPET encompassed in VOIDWI (>60%) on both scans. There was no significant correlation between the quantifiable measures SUVmax and ADCmin across patients; however, on a voxel-by-voxel basis the correlation between ADC and SUV was significant, albeit probably too weak to allow any meaningful assessment of one image metric from the other. The cluster analysis proved feasible and reproducible, identifying a volume encompassing most VOIPET and a smaller part of VOIDWI.
With the integrated PET/MR scanner, the tumor is assessed simultaneously, and the head and neck coil used limits the movement of the patient during scanning. Hence, it is unlikely that a misalignment between the DWI and PET images is the main reason for discrepancy between the volumes VOIPET and VOIDWI. Other technical reasons for the partial overlap include geometric distortions of the DWI signal close to air cavities such as in the pharynx, which may remain despite the optimized DWI acquisition and FUGUE correction. Both image acquisition and postprocessing were optimized to minimize distortions. The visually judged correspondence of DWI and 18F-FDG PET was overall good, as seen in the figures (25). After this FUGUE correction was implemented, no patient had to be excluded because of signal drop out (Supplemental Fig. 1). The remaining part of the observed mismatch is likely due to a biologic difference—that is, intratumor heterogeneity. Thus, when the mismatch due to repositioning and technical distortions is minimized, the method presented here might have the potential to identify and describe areas of the tumor with different biologic characteristics, which is a prerequisite for personalized treatment in the future.
Dose painting is a novel concept in radiotherapy in which the radiation dose is escalated in parts of the tumor thought to be treatment resistant such as hypoxic regions or regions with high pretreatment 18F-FDG uptake (27,28). Tumor areas with high glucose uptake or high cellularity are hypothesized as relevant targets for dose painting (17,29), and if the tumor subvolume defined by DWI and 18F-FDG PET is identical it could in theory be possible to replace 18F-FDG with another PET tracer without significant loss of information when imaged simultaneously with DWI on an integrated PET/MR scanner. The replacement of 18F-FDG with another PET tracer could provide additional potentially important information of tumor biology. For instance, tumor subregions with high proliferation (3′-deoxy-3′-18F-fluorothymidine), hypoxia (18F-fluoroazomycin arabinoside), or markers for aggressiveness; for example, urokinase-type plasminogen activator receptor PET would be interesting in terms of not only multiparametric imaging research but also potential clinical relevance (30,31). These subregions might be used for treatment guidance such as in dose painting or be used to select patients for other more aggressive treatment regimens in the future. The tumor overlap of VOIDWI and VOIPET assessed in this study is substantial but nevertheless only partial, and together with the relatively weak correlation between image surrogates of high cellularity (assessed with DWI) and high glucose uptake (assessed with 18F-FDG PET), our results indicate that the 2 imaging modalities provide complementary information on tumor biology. Moreover, these subvolumes of the tumor seem to be stable over time with regard to both quantitative ADC and SUV and spatial placement. The reproducibility of the 18F-FDG measurements has been documented in another study (23), but the reproducibility of the ADC values has not previously been assessed.
The partial overlap demonstrated in this study is in concordance with the study by Houweling et al. (32). Thus, substituting one modality with the other is not possible without some loss of information. It can also be concluded that replacing 18F-FDG PET with DWI for tumor delineation would yield smaller target volumes in radiotherapy, potentially missing substantial tumor volume as defined by 18F-FDG PET. It is also possible that the subvolume identified by the cluster-analysis based on information from both DWI and 18F-FDG PET could be a potential target for dose escalation. But this needs confirmation in studies with histologic correlation or failure pattern analysis (33). It could be argued that the cluster analysis did not seem to provide further useful information compared with the overlap analysis from the manual delineated tumor volumes (VOIPET and VOIDWI). Nevertheless, the substantial overlap of information from DWI and 18F-FDG PET may be encouraging if non–18F-FDG is to be used as part of PET/MR imaging.
To our knowledge, only 1 study has evaluated the correlation between DWI and 18F-FDG PET on an integrated PET/MR scanner in patients with HNSCC (6). This study also reported a negative correlation, however, the study included only 7 patients with different tumor subsites (6). The existing studies in the literature either are not performed on an integrated PET/MR scanner or do not include patients with head and neck tumors (21,22,34–38). The nonsignificant correlation found across patients suggests that information on glucose metabolism and cellularity from only 1 voxel, the voxel within the tumor either with the highest 18F-FDG uptake (SUVmax) or with the lowest diffusion (ADCmin), may be too crude to adequately describe the tumor and depict a potential correlation. This is substantiated by the significant correlation reported in most cases in the voxel-by-voxel analysis (Supplemental Fig. 2); nevertheless, the weak correlation shows that a biologic mechanistic hypothesis in which diffusion of water is uniformly impaired in areas with high glucose metabolism is an oversimplification.
Though the results in this study also seem reproducible from scan 1 to scan 2, the small number of patients is a limitation of this study, and there could be true correlations that the sample size is too small to detect. Moreover, the tumors in this patient cohort are relatively small, and the application of voxel-by-voxel analysis for description of tumor heterogeneity will probably be more relevant and provide more information in larger tumors.
CONCLUSION
In multiparametric imaging with integrated PET/MR, the VOIs from DWI and 18F-FDG PET were both within the target volume for radiotherapy and overlapped substantially although not completely. This is important for further research in tumor biology and may have implications for the use of PET/MR for radiotherapy in head and neck cancer and possibly in other malignancies. No significant correlation between 18F-FDG uptake and DWI could be found across patients. However, in individual patients a weak correlation could be found on a voxel-by-voxel basis. This suggests that, despite the partial tumor overlap, 18F-FDG PET and DWI detect different aspects of tumor biology, and they may possibly have complementary roles in target definition for dose painting, which should be explored further with histologic validation.
DISCLOSURE
Jacob H. Rasmussen received support from the Arvid Nilssons Foundation. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Sep. 8, 2016.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication July 4, 2016.
- Accepted for publication August 18, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.