


Abstract
18F-FDG PET is an effective method of predicting recurrence of hepatocellular carcinoma (HCC) after liver transplantation. We compared recently introduced metabolic and volumetric 18F-FDG PET/CT indices with the current clinicopathologic predictors for ability to predict recurrence. Methods: In total, 110 HCC patients who underwent 18F-FDG PET and liver transplantation were enrolled. On PET, SUVs and tumor-to-background ratios (TBRs) were measured as metabolic activity indices. Various metabolic tumor volumes and uptake-volume products (UVP) were also measured as volumetric indices. The ability of these indices and other clinicopathologic factors to predict recurrence was compared. Results: All metabolic and volumetric indices were significant for recurrence prediction on receiver-operating-characteristic curve analyses (P < 0.001). On univariate survival analyses, all PET indices—as well as tumor size, tumor number, the Milan criteria, tumor grade, vascular invasion, and T-stage—were significant factors. However, on multivariate analyses, tumor size, tumor grade, maximum TBR, and UVP calculated by inferior vena cava activity were significant factors (P = 0.004, 0.014, 0.009, and 0.021, respectively). When the Milan criteria and PET factors were included in the multivariate analysis, the Milan criteria (P = 0.029), maximum TBR (P < 0.001), and UVP (P = 0.016) were significant. Conclusion: Volumetric and metabolic activity indices of 18F-FDG PET are effective predictors of posttransplantation HCC recurrence. In addition to clinicopathologic factors, these indices need to be considered in the selection of candidates for liver transplantation.
- hepatocellular carcinoma
- liver transplantation
- positron emission tomography
- recurrence
- metabolic tumor volume
Liver transplantation is the best option for radical treatment of early but unresectable hepatocellular carcinoma (HCC), particularly in the setting of liver cirrhosis (1,2). However, HCC recurs after liver transplantation in approximately 20%–30% of patients, and recurrence is difficult to treat and is the rate-limiting factor for long-term survival (3–5). For prediction of HCC recurrence and selection of appropriate candidates for liver transplantation, the Milan criteria, which consider size and number of tumors, have performed well (6), and some other pathologic factors also have been shown to be significant prognostic factors for posttransplantation recurrence (7,8). However, exact assessment of the Milan criteria and pathologic factors is not possible before liver transplantation, and thus, use of other laboratory tests or radiologic factors for selecting candidates has been attempted (8,9).
Currently, PET/CT using 18F-FDG is widely applied in oncologic clinical practice. With regard to HCC, PET/CT is effective in initial staging, prediction of treatment response, and detection of recurrence (10–12). Additionally, PET/CT has been reported to be effective in predicting posttransplantation recurrence using visual analysis or semiquantitative indices such as SUV or tumor-to-background ratio (TBR) (13,14).
In recent years, the use of volumetric indices in PET/CT has been increasing because they can reflect tumor burden as well as metabolic activity. Metabolic tumor volume (MTV) and total lesion uptake on PET/CT are effective indices, particularly in terms of prognosis prediction and treatment response monitoring (15–18). These volumetric indices are also expected to be effective in recurrence prediction after liver transplantation for HCC, because the indices consider tumor burden. However, to our knowledge, use of volumetric indices has not been attempted for prediction of HCC recurrence after liver transplantation.
In this study, we investigated the prognostic value of volumetric indices of PET/CT in predicting posttransplantation recurrence of HCC. Various methods of using volumetric indices were tested to determine those that are optimal, and their prognostic value was compared with that of clinicopathologic factors.
MATERIALS AND METHODS
Patients
From April 2008 to November 2012, liver transplantation was performed on 249 consecutive patients at our institution. Those patients who underwent liver transplantation because of HCC were retrospectively enrolled in this study with the following inclusion criteria; pathologically confirmed HCC before liver transplantation, 18F-FDG PET/CT performed within 4 mo before liver transplantation, and follow-up more than 24 mo after liver transplantation in cases of nonrecurrence. At our institution, candidates for liver transplantation are selected on the basis of the Milan criteria. However, liver transplantation is also performed when the Milan criteria are not met if a patient strongly desires transplantation from a living donor and there is neither major vascular invasion nor extrahepatic metastasis. Patients are routinely followed up using contrast-enhanced CT every 3 mo during the first year after liver transplantation and every 6 mo thereafter. MRI is complementarily used in some cases. Serum α-fetoprotein level is measured every 2–3 mo. Additional imaging studies are performed when the level is increased or other suggestive symptoms or signs appear. Recurrence of a lesion is confirmed by follow-up imaging studies.
The study design was approved, and the need for informed consent waived, by our Institutional Review Board (H-1508-030-696).
18F-FDG PET/CT and Image Analysis
18F-FDG (5.18 MBq/kg) was injected intravenously after the patient had fasted for at least 6 h, and imaging was performed 1 h later using a PET/CT scanner (Biograph 40 TruePoint; Siemens Healthcare) with an imaging resolution of 0.4 mm for CT and 4.2 mm for PET. CT images were acquired from the skull base to the upper thigh for creation of an attenuation map and localization of lesions (50 mA, 120 kVp, 5-mm section width). After the CT scan, PET images of the same area were acquired in 3-dimensional mode at 6–7 bed positions. Images were reconstructed on 128 × 128 matrices using an iterative algorithm and analyzed using a dedicated workstation and software (Syngo.via; Siemens Healthcare).
The images were visually analyzed first by two experienced image specialists working in consensus; the patient’s HCC was classified as hypermetabolic (discernible from the background liver) or nonhypermetabolic (not discernible from the background liver). For quantitative analysis of the PET images, SUV was measured. Additionally, TBR—defined as the ratio between the maximum SUV of a target lesion and background tissue—was calculated, adopting the inferior vena cava (IVC) or normal liver as the background tissue. Cylindric volumes of interest (VOIs; 1 cm3) were drawn on 3 levels of the abdominal IVC, and SUVmean was measured. Spheric VOIs (20 cm3) were drawn on 3 sites of normal liver, and SUVmean was measured (Fig. 1). TBRs calculated using IVC activity and normal-liver activity were defined as TBRIVC and TBRNL, respectively. For tumor lesions, SUVmax and TBRmax (TBRIVCmax or TBRNLmax) were measured as indices of metabolic activity.
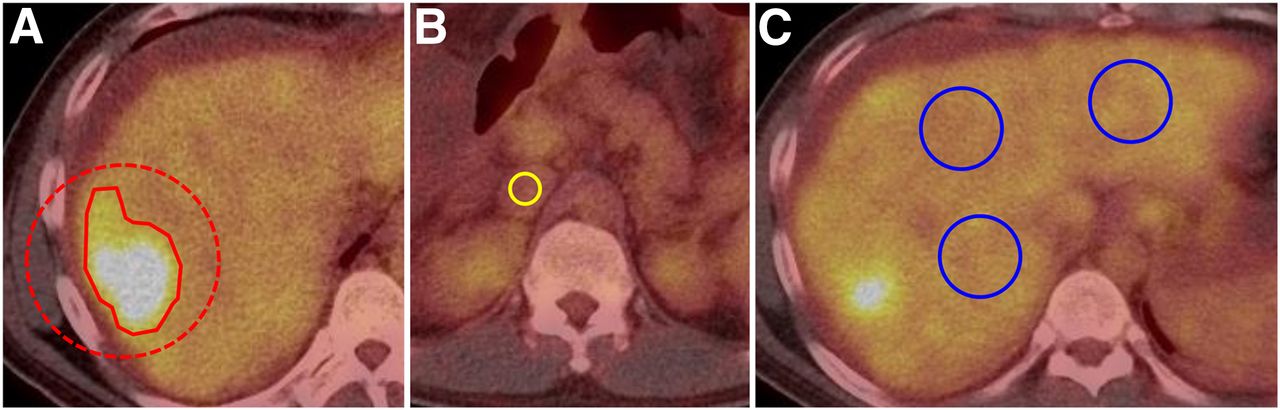
Measurement methods using 18F-FDG PET/CT indices. Spheric VOI (dashed circle) was manually drawn to include entire tumor, and isoactivity contour (solid line) was automatically drawn by setting a certain threshold (A). For background activity, 1-cm3 cylindric VOIs (yellow circle) were drawn on IVC (B) and 20-cm3 spheric VOIs (blue circles) were drawn on normal liver (C).
MTV and uptake–volume product (UVP), indices of metabolic tumor burden, were measured from tumor VOIs defined by isoactivity contours. A spheric VOI was manually drawn with reference to the enhanced CT images to include the entire lesion, and an isoactivity contour was automatically drawn by setting a certain margin threshold around the lesion. Two margin thresholds were adopted on the basis of a pilot study (Supplemental Table 1, available at http://jnm.snmjournals.org): TBRIVC 2.0 and TBRNL 1.5. In a tumor VOI, MTV was defined as the volume (cm3), and UVP was defined as the product of TBRmean and MTV. Values that were measured using thresholds for TBRIVC were defined as MTVIVC and UVPIVC, and those measured using thresholds for TBRNL were defined as MTVNL and UVPNL.
Clinicopathologic Factors and Statistical Analysis
Clinicopathologic information was obtained from medical record review. Sex, age, pretransplantation α-fetoprotein level, viral infection status, and donor type were analyzed as clinical factors. The Milan criteria, tumor size (the largest diameter, in cm), tumor number, necrotic portion of tumors (%), tumor grade, vascular invasion, and T-stage were analyzed as pathologic factors.
Clinicopathologic factors and image indices were compared between the recurrence and nonrecurrence groups using the χ2 test for categoric data, the Student t test for continuous data, and the Mann–Whitney test for nonparametric analysis. For predicting recurrence, the receiver-operating-characteristic curves for quantitative indices of PET/CT were analyzed. For predicting recurrence-free survival, Kaplan–Meier curve and stepwise Cox regression analysis was performed. In survival analysis, optimal cutoffs for quantitative factors were determined using an algorithm (19) that selects the cutoff that maximizes significance. All statistical analyses were performed using commercialized statistical software packages (SPSS, version 18.0 [SPSS Inc.], and MedCalc, version 15.8 [MedCalc Software bvba]). Continuous variables were expressed as mean ± SD, and P values of less than 0.05 were considered significant.
RESULTS
Clinicopathologic Characteristics and Follow-up
Of the 249 patients who underwent liver transplantation during the study interval, the cause was HCC in 215; of those 215, 18F-FDG PET/CT was performed beforehand in 121; of those 121, the inclusion criteria were met by 110 (89 men and 21 women; age 54 ± 9 y, range 22–72 y). Their clinical characteristics are summarized in Table 1.
Clinicopathologic Characteristics According to Recurrence
During the follow-up period (45.6 ± 18.0 mo; range, 7.4–83.1 mo), HCC recurred in 30 patients (27%) at 11.5 ± 9.0 mo after liver transplantation (range, 0.9–36.2 mo), involving extrahepatic organs in 20 patients, only liver in 2 patients, and both liver and extrahepatic organs in 8 patients. None of the analyzed clinical factors significantly differed between the recurrence and nonrecurrence groups. In contrast, most of the pathologic factors differed significantly; the recurrence group had larger tumor size (P = 0.001), more tumor multiplicity (P = 0.011), more vascular invasion (P < 0.001), higher T-stage (P = 0.002) (Table 1), and fewer patients within the Milan criteria (P = 0.003).
PET/CT Indices and Recurrence
18F-FDG PET/CT was performed 0.7 ± 0.6 mo (range, 0.0–3.7 mo) before liver transplantation. On visual analysis of PET/CT images, the rate of hypermetabolic lesions was higher in the recurrence group (P < 0.001). On quantitative analysis, SUVmax, TBRIVCmax, and TBRNLmax were significantly higher in the recurrence group (P < 0.001 for all). Additionally, MTV and UVP were significantly higher in the recurrence group for both of the thresholds used for isoactivity contour drawing (Table 2).
PET/CT Findings According to Recurrence
On receiver-operating-characteristic curve analysis, all PET/CT indices were significantly predictive of recurrence (P < 0.001 for all; Table 3). However, the indices calculated by IVC activity (TBRIVCmax, MTVIVC, and UVPIVC) had higher areas under the curve than those calculated by normal-liver activity (TBRNLmax, MTVNL, and UVPNL). Among the metabolic activity indices, TBRIVCmax had the highest area under the curve, 0.913, with sensitivity and specificity of 83.3% and 88.7%, respectively, at the 1.16 cutoff. Among the metabolic burden indices, UVPIVC exhibited the highest area under the curve, 0.896, with sensitivity and specificity of 90.0% and 81.2% at the 0.73 cutoff. Based on these results, IVC-based quantitative PET/CT indices were used in the survival analysis.
Receiver-Operating Characteristic Curve Analysis of PET/CT Quantitative Indices in Predicting Recurrence
Survival Analysis
Among clinicopathologic factors, tumor size (cutoff, 6.7 cm), tumor number (1 vs. ≥2), Milan criteria (within vs. beyond), tumor grade (1/2 vs. 3/4), vascular invasion (yes vs. no), and T-stage (T1/T2 vs. T3/T4) were included in the univariate survival analysis, and all were significantly predictive of recurrence (Table 4). Among PET/CT factors, visual findings (hypermetabolic vs. nonhypermetabolic), SUVmax (cutoff, 5.16), TBRIVCmax (cutoff, 1.25), MTVIVC (cutoff, 18.3), and UVPIVC (cutoff, 14.3) were also significant for predicting recurrence (P < 0.001 for all). TBRIVCmax and UVPIVC exhibited hazard ratios of 13.65 and 12.49, respectively (Fig. 2).
Results of Survival Analyses

Kaplan–Meier survival analysis with regard to TBRIVCmax and UVPIVC. (A) Patients with low TBRIVCmax (≤1.25) showed significantly longer recurrence-free survival than those with high TBRIVCmax (>1.25). (B) Patients with low UVPIVC (≤14.3) showed significantly longer recurrence-free survival than those with high UVPIVC (>14.3).
On multivariate analysis, when all clinicopathologic factors (except the Milan criteria) and PET/CT quantitative indices were included, tumor size, tumor grade, TBRIVCmax, and UVPIVC were found to be significant (P = 0.004, 0.014, 0.009, and 0.021, respectively). When PET/CT indices with the Milan criteria alone were included, the Milan criteria (P = 0.029), TBRIVCmax (P < 0.001), and UVPIVC (P = 0.016) were significant (Table 4). The hazard ratios for these factors were 2.54, 6.75, and 3.16, respectively. Images of representative cases are shown in Figure 3.

Images of representative cases. (A–C) 65-y-old man who presented with hepatic tumor (arrows) on enhanced CT (A), which showed high TBRIVCmax (2.59) and UVPIVC (18.91) on 18F-FDG PET/CT (B) and PET (C). Although patient was within Milan criteria (3 tumors, with largest being 2.5 cm, and no vascular invasion), tumor recurred 16 mo after transplantation. (D–F) In contrast, 54-y-old man with hepatic tumor (arrowhead) on enhanced CT (D) showed low TBRIVCmax (1.09) and UVPIVC (13.54) on 18F-FDG PET/CT (E) and PET (F). Although he was beyond Milan criteria (3 tumors, with largest being 3.3 cm), he exhibited no tumor recurrence until 41.7 mo after transplantation.
DISCUSSION
In this study, we demonstrated that 18F-FDG PET/CT can provide effective predictors of HCC recurrence after liver transplantation. On comparing several methods of producing metabolic indices on 18F-FDG PET/CT, we found TBRIVCmax and UVPIVC to be significant prognostic factors and to exhibit higher predictive power than the other indices; both were found to be significant prognostic factors on multivariate analysis.
Because liver transplantation requires a limited resource—donor organs—and is expensive, selection of candidates who have a low likelihood of HCC recurrence is of the utmost importance. Several methods, including the Milan criteria, are currently used to select candidates, and most of these methods are based on the size and number of intrahepatic tumors. Although such methods can be effective in predicting recurrence and in selecting candidates (20), their predictive power needs to be enhanced. Moreover, the precise evaluation of pathologic factors such as tumor size, tumor number, vascular invasion, and tumor grade is possible only when the explanted liver is available. Thus, 18F-FDG PET/CT imaging, which shows the metabolic activity of a tumor, has been used to predict HCC recurrence after liver transplantation.
In some previous studies, the metabolic status of HCC as seen on 18F-FDG PET was the only significant factor predicting long-term survival (21) and early recurrence (<6 mo) after liver transplantation (22). Other studies found some additional factors to be significant, such as the metabolic status of the HCC, the extent of vascular invasion (23,24), and the degree of differentiation (23,24). Aside from one discordant result (25), the use of 18F-FDG PET/CT TBR as a metabolic activity index has been reported to be efficacious in predicting HCC recurrence after liver transplantation (14).
In addition to metabolic activity indices such as SUV and TBR, volumetric indices are now widely used to analyze 18F-FDG PET/CT results for various cancers (15–18). MTV is defined as the volume of tissue that exhibits a higher metabolism over a certain threshold, and total lesion uptake, or total lesion glycolysis, is defined as MTV multiplied by SUVmean. In the present study, UVP, an index of total lesion uptake, was calculated as MTV multiplied by mean uptake expressed in TBR. Although SUVmax and TBRmax reflect the metabolic activity of the most malignant component of a tumor, volumetric indices reflect both metabolic activity and tumor burden, that is, the size of the entire tumor. In liver transplantation for HCC, the size and number of tumors—which are considered in the Milan criteria—relate to tumor burden, and thus we tested the predictive values of these volumetric indices in comparison with metabolic activity indices.
Despite the potential value of volumetric indices, there is no single optimal method for metabolic volumetry. Currently, a certain SUV or a certain percentage of SUVmax is commonly used as a threshold for volumetry (26). However, although SUV is often prone to measurement errors, TBR is relatively robust because it is based on the activity of reference tissue in the same image of a patient. We compared several metabolic activity and volumetric indices and, similar to a previous report (14), found that TBRmax exhibited greater significance than SUVmax in predicting posttransplantation recurrence. Thus, TBR was used for measuring volumetric indices with varying thresholds, and UVP was used instead of the commonly used volumetric index, total lesion glycolysis. In the pilot study, we tested various thresholds in the measurement of MTV, and we selected TBRIVC 2.0 and TBRNL 1.5 on that basis. Intriguingly, the indices based on IVC activity were slightly more predictive than those based on normal-liver activity. It is speculated that IVC is a more reliable background than normal liver because normal liver tissue shows varying SUVs of 1.4–5.0 in HCC (27). Additionally, many HCC patients have underlying viral hepatitis and liver cirrhosis, which may influence 18F-FDG uptake in normal liver tissue.
TBRIVCmax had the highest area under the receiver-operating-characteristic curve and the highest hazard ratio on multivariate analysis. This finding suggests that the metabolic activity of the most malignant component of the tumor is a significant prognostic factor in liver transplantation for HCC. In contrast to treatments such as chemotherapy, radiotherapy, and some excisional surgeries, the entire primary organ of the tumor is removed in liver transplantation. All but two of our study patients experienced recurrence in extrahepatic organs. We thus speculate that the potential for distant metastasis relates closely to posttransplantation recurrence and that TBRIVCmax is a marker for metastatic potential. However, UVPIVC also was a significant prognostic factor, suggesting that overall metabolic tumor burden is another independent prognostic factor for metastasis. Further studies on large, prospective patient cohorts are warranted to determine the potential of volumetric indices to complement or add to the prognostic role of metabolic activity indices.
Among the clinicopathologic factors, tumor size was found to be significant on multivariate analysis, in addition to TBRIVCmax and UVPIVC. We adopted a tumor size cutoff that was optimized for our dataset. The cutoff was somewhat different from that established in the Milan criteria, and thus, multivariate analysis was performed again including the Milan criteria as a clinicopathologic factor, with the result being that TBRIVCmax and UVPIVC, as well as the Milan criteria, were still significant prognostic factors. Further studies are required to establish optimal criteria for selection of HCC liver transplantation candidates—criteria combining all significant clinicopathologic and PET/CT factors that are preoperatively available.
The present study had several limitations. It was retrospective, and its protocol was not strictly controlled. The relatively large variation in interval between 18F-FDG PET/CT and liver transplantation may have been a bias factor, even if not a critical one. Additionally, the retrospective design resulted in some missing clinicopathologic data, such as the Child–Pugh score before transplantation (6) and pathologic findings of satellitosis and giant cells (7).
CONCLUSION
In addition to clinicopathologic factors such as tumor size and the Milan criteria, 18F-FDG PET/CT indices such as volumetric and metabolic activity are effective predictors of HCC recurrence after liver transplantation. Among the various PET/CT indices, TBRIVCmax and UVPIVC are significant. It is expected that prediction of HCC recurrence and selection of candidates for liver transplantation can be optimized through a combination of both clinicopathologic factors and PET/CT indices.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This research was supported by grants HI14C1277 and HI14C1072 from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare, Republic of Korea. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Mar. 16, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication November 18, 2015.
- Accepted for publication February 2, 2016.





{kind=link}
{kind=link}
{kind=link}