


Abstract
18F-FDG PET has been widely used in the management of malignant tumors. In gastric cancer, the status of human epidermal growth factor receptor 2 (HER2) predicts the response to anti-HER2 antibody therapy, and testing of HER2 expression is now routine in the management of gastric cancer patients. However, to date, the relationship between 18F-FDG uptake and HER2 expression has not, to our knowledge, been investigated. In this study, we aimed to investigate whether HER2 expression is associated with 18F-FDG uptake and whether 18F-FDG PET/CT can be used to predict the HER2 status of gastric cancer. Methods: A retrospective analysis was performed on 64 gastric cancer patients who had undergone 18F-FDG PET/CT before surgical resection. Tumor SUVmax was calculated from the level of 18F-FDG uptake. Results: No significant correlation was found between SUVmax and HER2 expression in gastric cancer. However, when signet-ring cell carcinoma was excluded, SUVmax was significantly higher in the HER2-negative group than in the HER2-positive group (8.619 ± 5.878 vs. 3.789 ± 2.613, respectively; P = 0.021). Multivariate analysis indicated that SUVmax and tumor differentiation remained significantly associated with HER2 expression (P = 0.048 and P = 0.028, respectively). HER2 expression was predicted with an accuracy of 64.4% when an SUVmax cutoff of 6.2 was used. Conclusion: 18F-FDG uptake by gastric cancer is associated with HER2 expression. 18F-FDG PET/CT may be useful for predicting the HER2 status of gastric cancer and for determining the therapeutic strategy.
Gastric cancer is the fourth most frequently diagnosed cancer in the world and the second most common cause of death from cancer (1). Surgery is still the most common treatment. However, treatment outcomes for gastric cancer remain poor, particularly in patients with inoperable or metastatic disease (2). Therefore, effective therapeutic regimens for such patients need to be identified and developed. Previous studies have shown that 7%–34% of patients with gastric cancer are positive for human epidermal growth factor receptor 2 (HER2) (3–6). For patients with advanced HER2-positive gastric cancer, a combination of chemotherapy and trastuzumab, a monoclonal antibody against HER2, is now a standard option (7). The results of the “Trastuzumab for Gastric Cancer” trial (7) have caused HER2-targeted molecular therapies to become highly relevant in the treatment of gastric cancer. Therefore, it is important to identify clinical characteristics that might be predictive of HER2 status.
Although it has become standard practice to determine HER2 expression in gastric cancer patients, the procedure is invasive. Alternative noninvasive strategies, such as PET/CT, for predicting the mutation profile would therefore be of great value. Several studies have demonstrated that PET/CT has the potential to predict the phenotype of a tumor (8–11), such as the KRAS status in colorectal cancer (9,10) and the lactate dehydrogenase A expression level in lung adenocarcinoma (12), the latter being useful for treatment strategies involving lactate dehydrogenase A inhibitor. 18F-FDG PET/CT has been widely used for diagnosis, monitoring of treatment response, surveillance, and prognostication in a variety of cancers (13–15). However, the relationship between 18F-FDG uptake and HER2 expression, and the possible underlying mechanisms, are not clear.
The present study aimed to investigate whether HER2 expression is associated with 18F-FDG uptake and whether 18F-FDG PET/CT can be used to predict the HER2 status of gastric cancer. To our knowledge, this was the first study to present evidence of the potential value of 18F-FDG PET/CT scans for this use and to suggest that 18F-FDG PET/CT may play a key role in determining the strategy for gastric cancer patients by predicting their response to anti-HER2 antibody therapy.
MATERIALS AND METHODS
Study Population
Sixty-four patients (38 men and 26 women; age range, 18–84 y) with gastric cancer were included in this study. All had undergone 18F-FDG PET/CT followed by tumor resection at the Shanghai Jiaotong University–affiliated Ren Ji Hospital between January 2008 and November 2015. Patients were eligible for inclusion if they met the following criteria: they had been treated exclusively by total or subtotal gastrectomy with lymphadenectomy, according to tumor location; the diagnosis of gastric cancer had been confirmed by histopathologic examination of surgical specimens; adjuvant therapy had not been administered before PET/CT scanning; complete case records, including data on age, sex, tumor size, T stage, and histologic differentiation, were available; and tissue specimens for immunohistochemical staining were available. Sixty-four patients met these criteria and gave written informed consent to participate in the study, which was approved by the Institutional Review Board of Ren ji Hospital and was in accordance with the 2013 revision of the Declaration of Helsinki.
18F-FDG PET/CT
18F-FDG PET/CT was performed using a whole-body scanner (Biograph mCT; Siemens Medical Systems). All patients received an intravenous 3.7 MBq/kg injection of 18F-FDG after having fasted for at least 6 h and rested for 1 h. The mean uptake time was 50 ± 6 min. Blood glucose levels were measured and found to be less than 140 mg/dL at the time the 18F-FDG was administered. The CT component of the scan was performed without contrast administration using 120 kV, 140 mA, and a section thickness of 5.0 mm to match the thickness of the PET images. PET image datasets were reconstructed iteratively, with the CT data applied for attenuation correction.
For quantitative analysis, irregular regions of interest were placed over the most intense area of 18F-FDG uptake. SUVmax was calculated as (maximum pixel value with the decay-corrected region-of-interest activity [MBq/mL])/(injected dose [MBq]/body weight [kg]). The PET/CT images were evaluated by 2 experienced nuclear medicine physicians.
Immunohistochemical Analysis
Immunohistochemical analysis was performed on paraffin-embedded gastric cancer tissues after microtome sectioning (4-mm slices) and staining. Positivity for HER2 was evaluated using light microscopy by 2 independent pathologists who were masked to the clinical information. Membrane immunostaining of HER2 was scored as 0, 1+, 2+, or 3+ (16), following the consensus panel recommendations on HER2 scoring for gastric cancer (3). Slices with a score of 2+ or 3+ were classified as positive, or expressed, and slices with a score of 0 or 1+ were classified as negative.
Statistical Analysis
The data are presented as mean ± SD. Statistically significant differences between groups were compared using 1-way ANOVA and t testing. A P value of 0.05 or less was considered statistically significant. Statistical analysis was performed using SPSS, version 13.0 (SPSS Inc.).
RESULTS
Patient Population
Among the 64 patients, 21 had well- or moderately differentiated adenocarcinoma, 24 had poorly differentiated adenocarcinoma, and 19 had signet-ring cell carcinoma. Lymph node metastasis was detected in 36 patients. Regarding HER2 expression, 17.2% of the tumors were positive (12.5% with a score of 2+ and 4.7% with a score of 3+) and 82.8% negative (60.9% with a score of 0 and 21.9% with a score of 1+).
Correlation Between Patient Characteristics and SUVmax
The SUVmax for the primary tumors ranged from 1 to 27.1, with an average of 6.34. Table 1 shows the relationship between the clinicopathologic parameters and SUVmax. Statistical analysis found no significant differences in SUVmax according to sex, lymph node metastasis, T category, or location of tumor. However, there were significant differences in SUVmax according to histopathologic subtype, age, and tumor size. Poorly differentiated adenocarcinoma had a significantly higher SUVmax than did well- or moderately differentiated adenocarcinoma (9.579 ± 6.474 vs. 5.452 ± 3.722; P = 0.014; Supplemental Fig. 1A) or signet-ring cell carcinoma (9.579 ± 6.474 vs. 3.226 ± 1.209; P < 0.001). In addition, well- or moderately differentiated adenocarcinoma had a significantly higher SUVmax (5.452 ± 3.722 vs. 3.226 ± 1.209; P = 0.017) than did signet-ring cell carcinoma, although the latter also had poor differentiation. When we incorporated signet-ring cell carcinoma into the poorly differentiated adenocarcinoma group, there was no significant difference in SUVmax between the poorly differentiated group and the well- or moderately differentiated group (6.772 ± 5.811 vs. 5.452 ± 3.722; P = 0.347; Supplemental Fig. 1B) because signet-ring cell carcinoma had low 18F-FDG uptake.
Relationship Between SUVmax and Clinicopathologic Characteristics (n = 64)
Correlation Between Patient Characteristics and HER2 Expression
Patients were categorized into 2 groups according to immunohistochemical staining for HER2: patients with HER2 expression (n = 11) and patients without HER2 expression (n = 53). Supplemental Table 1 shows the results of the univariate analysis for each factor. There was no significant difference in SUVmax between gastric cancer patients with HER2 expression and those without HER2 expression (6.893 ± 5.495 vs. 3.673 ± 2.352; P = 0.062; Fig. 1A).

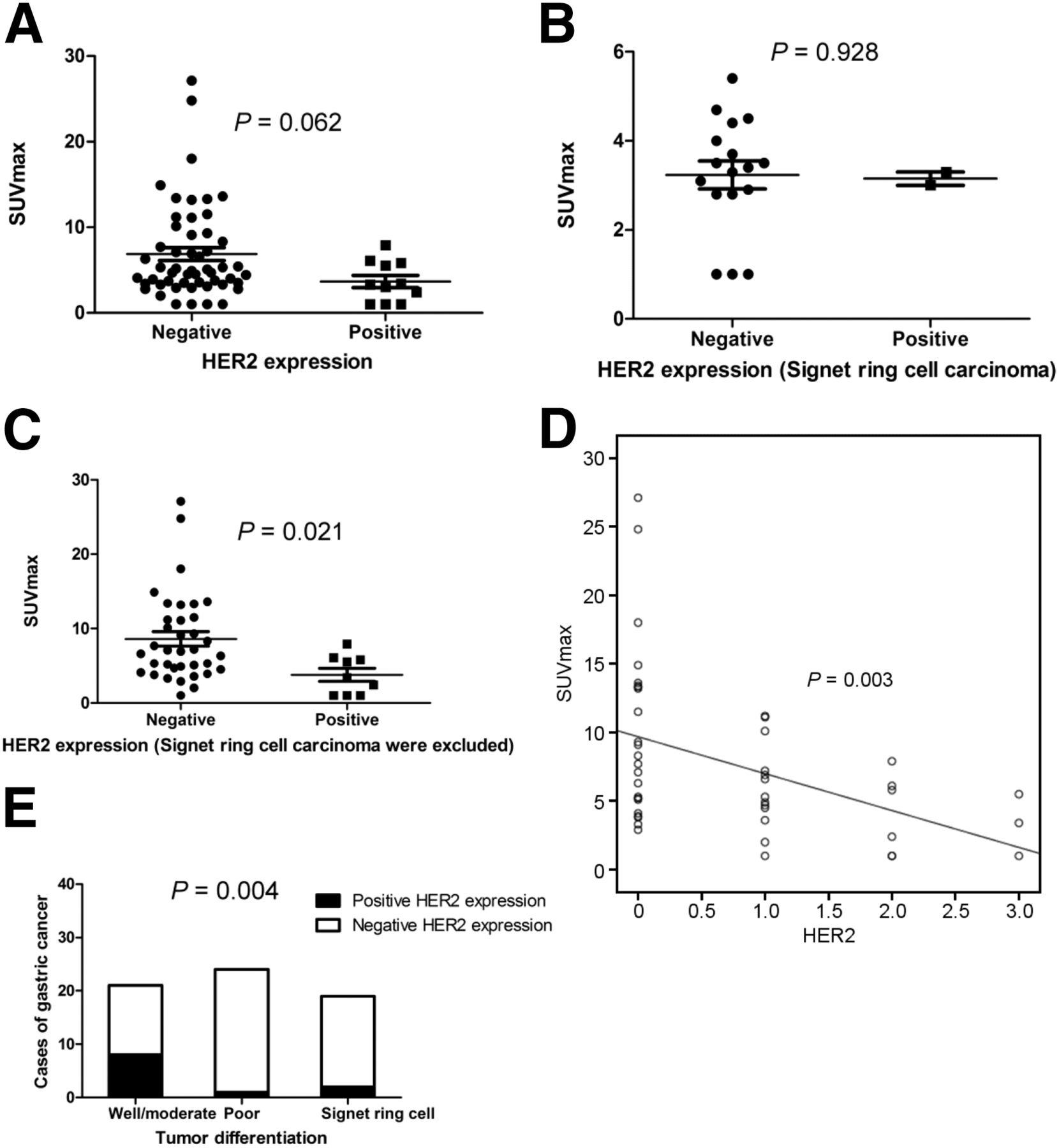
Analysis of SUVmax according to HER2 expression. (A) When all gastric cancer was considered (n = 64), SUVmax of HER2-negative group did not significantly differ from that of HER2-positive group (6.893 ± 5.495 vs. 3.673 ± 2.352; P = 0.062). (B) When only signet-ring cell carcinoma was considered (n = 19), SUVmax of HER2-negative group did not significantly differ from that of HER2-positive group (3.235 ± 1.281 vs. 3.150 ± 0.212; P = 0.928). (C) When signet-ring cell carcinoma was excluded, SUVmax was significantly higher in HER2-negative group than in HER2-positive group (8.619 ± 5.878 vs. 3.789 ± 2.613; P = 0.021). (D) SUVmax correlated inversely with HER2 score (P = 0.003). (E) Rates of HER2 expression were higher for well- and moderately differentiated adenocarcinoma than for poorly differentiated adenocarcinoma or signet-ring cell carcinoma.
We next excluded signet-ring cell carcinoma because it has a low SUVmax regardless of HER2 status (3.235 ± 1.281 vs. 3.150 ± 0.212; P = 0.928; Fig. 1B). Table 2 shows the results of the univariate analysis for each factor. No significant differences in sex, age, tumor size, lymph node metastasis, or T category were found between the two groups. However, the groups differed significantly in SUVmax and tumor differentiation grade. HER2-negative gastric cancer had a significantly higher SUVmax than did HER2-positive gastric cancer (8.619 ± 5.878 vs. 3.789 ± 2.613; P = 0.021; Fig. 1C). There was an inverse correlation between SUVmax and HER2 score (P = 0.003; Fig. 1D). In addition, the rates of HER2 expression in well- or moderately differentiated adenocarcinoma, poorly differentiated adenocarcinoma, and signet-ring cell carcinoma were 38.1%, 4.2%, and 10.5%, respectively (Fig. 1E). The differences between well- or moderately differentiated adenocarcinoma and poorly differentiated adenocarcinoma (38.1% vs. 4.2%; P = 0.005) and between well- or moderately differentiated adenocarcinoma and signet-ring cell carcinoma (38.1% vs. 10.2%; P = 0.044) were statistically significant. Though signet-ring cell carcinoma had a higher rate of HER2 positivity than did poorly differentiated adenocarcinoma, the difference was not statistically significant (10.2% vs. 4.2%; P = 0.416).
Relationship Between HER2 Expression and Clinicopathologic Characteristics After Excluding Signet-Ring Cell Carcinoma (n = 45)
We next sought to determine the SUVmax threshold for optimal differentiation between these two groups. Receiver-operating-characteristic curve analysis revealed that the highest accuracy (64.4%) was obtained with an SUVmax cutoff of 6.2 and that the area under the curve was 0.703 ± 0.084. Sensitivity and specificity for the prediction of HER2 expression were 88.9% (8/9) and 58.3% (21/36), respectively. These results suggest that 18F-FDG PET/CT scans can be useful for predicting the HER2 status of gastric cancer when signet-ring cell carcinoma is excluded.
Predictors of HER2 Expression
Multivariate analysis revealed that SUVmax and tumor differentiation grade correlated significantly with HER2 expression in gastric cancer (Table 3). Therefore, using these parameters, we categorized the patients into groups based on their potential of being HER2-positive: a low-potential group (poorly differentiated adenocarcinoma and SUVmax > 6.2), a moderate-potential group (well- or moderately differentiated adenocarcinoma and SUVmax > 6.2, or poorly differentiated adenocarcinoma and SUVmax ≤ 6.2), and a high-potential group (well- or moderately differentiated adenocarcinoma and SUVmax ≤ 6.2). The probability of HER2 expression in these groups was 0%, 11.1%, and 53.8%, respectively (P = 0.001; Table 4).
Odds Ratios from Multivariate Analysis of Predictors of HER2 Expression
Rate of HER2 Expression in Cancer with Low, Moderate, and High Potential for HER2 Expression
DISCUSSION
Previous studies have shown that the HER2 status of gastric cancer predicts response to therapy with anti-HER2 antibodies (7). Testing for HER2 expression is now routine practice in the management of gastric cancer. Our study found a 17.2% rate of HER2 expression—similar to previous reports (3–6). A combination of chemotherapy and trastuzumab, a monoclonal antibody against HER2, is now a standard option in patients with HER2-positive gastric cancer (17). PET/CT is a molecular imaging technique widely used in the diagnosis and staging of malignant tumors (18). Our results showed that the SUVmax in gastric cancer was significantly lower when HER2 was expressed than when not expressed (excluding signet-ring cell carcinoma from the analysis). To our knowledge, this was the first study to analyze the association between HER2 expression and 18F-FDG uptake in gastric cancer patients.
The differentiation of signet-ring cell carcinoma was poor. However, expression of glucose transporter 1 is low in signet-ring cell carcinoma (19), and our study showed that signet-ring cell carcinoma had relatively low 18F-FDG uptake irrespective of HER2 status. There was no significant difference between the HER2- and HER2-negative groups in our study because signet-ring cell carcinoma accounted for a considerable proportion of the HER2-negative group. However, when we excluded signet-ring cell carcinoma, we found an excellent correlation between HER2 status and SUVmax. SUVmax was significantly lower in the HER2-positive group than in the HER2-negative group. Our data also demonstrated that HER2 expression is more common in well- or moderately differentiated adenocarcinoma than in poorly differentiated adenocarcinoma; this finding is consistent with the findings of previous studies (20–22). In addition, well- or moderately differentiated adenocarcinoma had significantly lower 18F-FDG uptake than did poorly differentiated adenocarcinoma, partly explaining why patients with HER2 expression had a low SUVmax (excluding signet-ring cell carcinoma from the analysis). The reasons for this selective high rate of HER2 expression in well- and moderately differentiated adenocarcinoma remain unclear. The association of HER2 expression with a specific histologic type indicates that certain characteristics may have a tendency to be expressed together. Previous reports have demonstrated higher rates of HER2 expression in tumors at the gastroesophageal junction than in more distally located gastric tumors (7,23), but this was not the case in our study. We attribute this result to the small number of patients with gastric cancer located in this region in our study.
We found an excellent correlation between HER2 status and SUVmax in gastric cancer (excluding signet-ring cell carcinoma from the analysis). The receiver-operating-characteristic curves and the area under the SUVmax curve indicated that 18F-FDG uptake may have a role in predicting HER2 expression. Multivariate analysis revealed that both the SUVmax of the primary tumor and the tumor differentiation grade correlated significantly with HER2 expression. We further categorized patients into groups based on their potential for being HER2-positive: high-potential, moderate-potential, and low-potential. HER2 was expressed in 53.8% of the high-potential group but none of the low-potential group, implying that anti-HER2 therapies are not feasible for patients with a low potential of being HER2-positive. HER2 status is routinely used to predict the efficacy of anti-HER2 therapies in gastric cancer. The INT-0116/SWOG9008 phase III clinical trial demonstrated that patients with HER2 amplification did not derive a survival benefit from chemoradiation therapy whereas patients without HER2 amplification derived a statistically significant survival benefit (24). The “Trastuzumab for Gastric Cancer” trial on metastatic gastric cancer demonstrated a significant overall survival benefit when trastuzumab was combined with chemotherapy (7). Moreover, new targeted therapies are being developed for HER2-positive gastric cancer. For these reasons, noninvasive methods, such as molecular imaging, for predicting HER2 status have great clinical relevance; they have the potential to evaluate the effect of neoadjuvant chemotherapy on advanced HER2-positive gastric cancer with metastatic lesions.
The role of HER2 as a prognostic factor in gastric carcinoma has been controversial. Some studies failed to find an association with prognosis (21,25), whereas others found a direct correlation between HER2 expression or amplification and poor survival (22,26). In our study, most cases were from recent years and the sample size was small. In a future study, we intend to collect more cases to elucidate the correlations between HER2 expression, overall survival, and the SUVmax of primary gastric cancer.
Our study was in part limited by its retrospective design and small sample size. Although PET/CT may have a moderate diagnostic performance, in the clinical setting it is not possible to establish a cutoff for SUVs. Therefore, PET/CT cannot replace conventional methods. Nonetheless, our results may be relevant for the development of noninvasive strategies to predict HER2 expression in gastric cancer patients. Advances in PET radiotracers may increase the sensitivity and specificity of this technique and enable full molecular assessment of gastric cancer.
CONCLUSION
Gastric cancer with HER2 expression shows decreased 18F-FDG uptake. Metabolic imaging has the potential to become a useful complement for assessing the molecular profile of gastric cancer and for predicting its response to anti-HER2 antibody therapies, particularly in advanced gastric cancer with metastases, which may require neoadjuvant chemotherapy. Further large prospective studies are needed to confirm our results and determine whether metabolic imaging can be used to determine the HER2 status of patients with gastric cancer and thus aid clinical decision-making on anti-HER2 antibody therapies.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was supported by grants 30830038, 30970842, 81071180, 81571710, 81530053, 81471685, and 81471687 from the National Natural Science Foundation of China, grant 2012CB932604 from the Major State Basic Research Development Program of China (program 973), and grant 2012ZX09506-001-00 from the New Drug Discovery Project. No other potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Mar. 10, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication December 10, 2015.
- Accepted for publication February 11, 2016.





{kind=link}