


Abstract
Heart failure is often complicated by arrhythmias that can adversely affect the quality of life and increase the risk for sudden cardiac death. Current risk stratification strategies for sudden cardiac death in the heart failure patient are not ideal, with much potential for further refinement. Overactivation of the sympathetic nervous system has been shown to be associated with worsening heart failure as well as arrhythmic events. Recent advances in our understanding of the autonomic nervous system and new methods for quantification of the pathologic activation of the sympathetic nerves have triggered increasing interest in this field. This viewpoint focuses on the need for and challenges of risk stratification of sudden death in the heart failure patient and discusses the potential value of measuring sympathetic nervous system activity to better stratify risk and to select patients with heart failure for implantable cardioverter defibrillator therapy.
Sudden cardiac death (SCD) is still the leading cause of death in the developed world, claiming up to 450,000 lives per year in the United States alone (1,2). Despite huge efforts to improve the outcomes, including public education in resuscitation and the widespread use of automatic external defibrillators, survival rates for out-of-hospital cardiac arrest are still dismal (3,4). Up to 80% of patients who have SCD have some degree of underlying coronary artery disease, but only around 20% will have actual pathologic evidence of acute myocardial necrosis (5), and only about one third of sudden cardiac arrest survivors will develop enzymatic evidence of myocardial infarction (6). Many of these patients may have triggers other than acute myocardial ischemia for their cardiac arrest, and between 10% and 20% of victims of SCD have dilated cardiomyopathy as the only underlying structural heart disease (7). However, high-risk patients with significant structural heart disease constitute a small minority of the total number of patients who experience malignant arrhythmias every year (8). Approximately 50%–60% of SCDs occur in the general population who have no significant heart disease; and even for those who have SCD and underlying structural heart disease, in up to 50% of the cases, sudden death is the first manifestation of disease (9,10).
Heart failure is a common disease that imposes a significant reduction in the quality of life and life expectancy for the individual patient and an increasing financial burden on the health care system (11). It is well known that patients with heart failure are at increased risk of SCD and ventricular arrhythmias, and a large body of evidence has indicated that patients with reduced left ventricular systolic ejection fraction (≤35%) are at greatest risk (12–15). In the Framingham heart study, patients with heart failure were 6–9 times more likely to have SCD than the general population (16). Interestingly, the mode of death correlates with the symptom class of heart failure: patients with mild to moderate symptoms are more likely to experience SCD, whereas patients with severe symptoms are more likely to die from pump failure (17). Hence, in the group of patients with severe heart failure (i.e., New York Heart Association class IV), the overall prognosis is poor, and the use of an implantable cardioverter defibrillator (ICD) is less likely to significantly prolong life; but in the group with moderate heart failure (New York Heart Association II and III), the risk of SCD is substantially higher and an ICD is more likely to be beneficial. Despite this crude, subjective classification of heart failure, there remains a paucity of risk stratification strategies that may help ferret out the patient with a reduced left ventricular ejection fraction (LVEF) who may benefit from an ICD.
RISK STRATIFICATION
The Need
One of the most important tasks for risk stratification in this context is the appropriate selection of patients who are at such a high risk of ventricular arrhythmias that they will benefit significantly from an ICD. It is well established that ICDs can successfully treat most ventricular arrhythmia episodes, thereby preventing a cardiac arrest from transforming into an SCD, but the treatment is costly from a health economics perspective (18), and it comes with a significant risk of potentially serious complications (19,20). Furthermore, on examination of the Multicenter Automatic Defibrillator Implantation Trial (MADIT II) (18) study data during the first 3 y after implantation, about 70% of the ICD-treated patients in a heart failure population with primary prophylactic ICDs will never need their device, 20% will die from heart failure anyway, and only 10% will be saved by their ICD. Even in the group of patients with adequate ICD therapy, not all arrhythmic events would have resulted in SCD if left untreated by the ICD. The occurrence of self-limiting episodes of ventricular tachycardia detected by the device may falsely indicate that the benefit regarding prevention of SCD is higher than it actually may seem. Indeed, with more conservative programming and delayed therapy up to 60 s after the initiation of ventricular tachycardia, such as in the MADIT-RIT (Reduction in Inappropriate Therapy) trial, the number of patients who were in need of appropriate ICD therapy during a 1.4-y follow-up was only 8%, indicating that most patients in fact did not have sustained malignant arrhythmias (21).
The only consistently reproducible selection criterion for primary prophylactic ICD treatment in the heart failure population so far has been reduced ejection fraction (<30%–35%), but it is widely acknowledged that this selection method is far from perfect (13,15,22–24). For instance, the Multicenter Unsustained Tachycardia Trial (MUSTT) showed that patients whose only risk factor was an ejection fraction of 30% or less had a 2-y arrhythmic risk of less than 5% (25). On the other hand, SCD still does occur in some patients with heart failure who may currently not qualify for ICD therapy (i.e., LVEF > 35%); clearly, a more refined selection tool would fill a clinical need in this area. A reflection of the uncertainty regarding the selection criteria can also be derived from the fact that 22% of all ICDs in the United States are implanted on the basis of indications that do not meet guideline-based criteria (26). Hence, although clinical electrophysiologists believe that ICDs are sometimes underused for those patients who really need them, the general perception may be that the health care system allows too many ICDs in patients who never actually need them. This then reinforces the need for a risk stratification strategy to solve the two key problems plaguing the field—namely, identification of low-risk patient subsets within the existing group of ICD-treated patients and identification of high-risk patient subsets outside the currently accepted criteria for ICD treatment. If imaging of the autonomic nervous system could enhance the risk stratification for high- or low-risk patients, that information could be incorporated into our current risk stratification schemes; and the combined information should then be used and tested in prospective randomized clinical trials comparing ICD intervention with optimal medical therapy.
The Challenges
Risk stratification of arrhythmias has always been challenging, especially because life-threatening rhythm disorders are dynamic events involving several variables. Looking at this simplistically, the minimum requirements for an arrhythmia to manifest typically include a trigger, a willing cardiac substrate, and a modulator such as the autonomic tone. The substrate is reflective of the underlying structural heart disease, such as scar or fibrosis in ischemic or dilated cardiomyopathy, or an inherent ion-channel disorder (e.g., long QT syndrome or Brugada syndrome). Arrhythmia triggers are acute events (e.g., electrolyte disturbances, myocardial ischemia, stress, or alcohol) that work in conjunction with the modulator (e.g., altered neurohormonal balance or pathologic activation of the autonomic nervous system in heart failure) that serves to perpetuate the arrhythmia once it is set in motion.
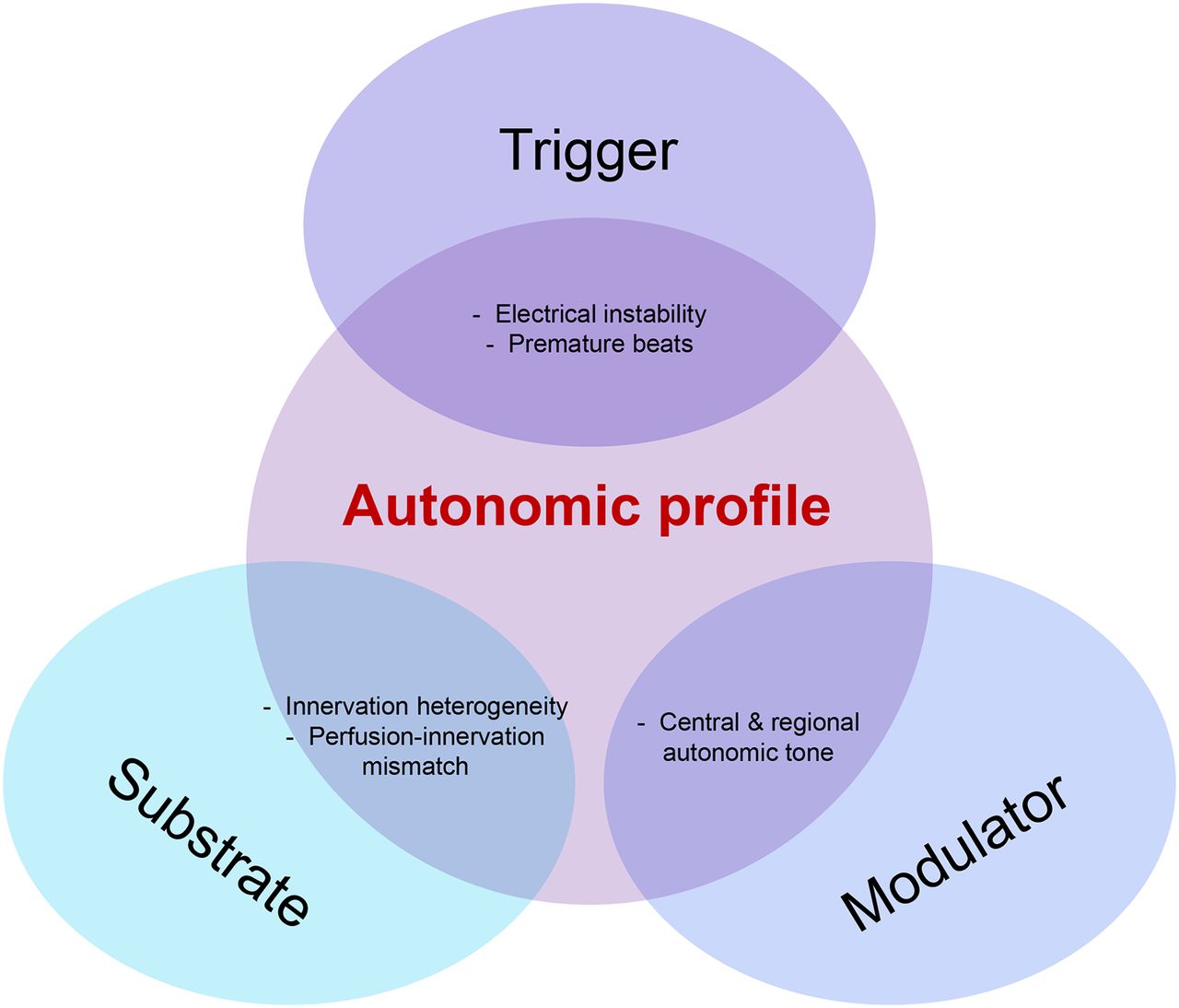
It is well known that increased sympathetic activity can be associated with arrhythmias and SCD and that increased parasympathetic activity can act protectively (27–29). Therefore, altered autonomic balance is increasingly recognized as an important factor in arrhythmogenesis; and in fact, the status of the cardiac autonomic nervous system can be implicated in all 3 major pathways that are believed to contribute to the initiation and perpetuation of lethal arrhythmias (Fig. 1). Cardiac denervation or innervation perfusion mismatch within a particular cardiac region can provide the autonomic substrate for a reentrant arrhythmia (30). An increased sympathetic activation and pathologic neurohormonal activation of the renin–angiotensin–aldosterone system (as seen in heart failure) can then provide the environment that is needed for the continuation of arrhythmias; and, finally, an altered sympathetic and parasympathetic nervous system balance promotes the occurrence of early afterdepolarizations and premature ventricular beats that can act as the crucial arrhythmia trigger. Thus, knowing the patient’s autonomic profile, in addition to other clinical variables, can be key to understanding an individual’s risk of SCD.
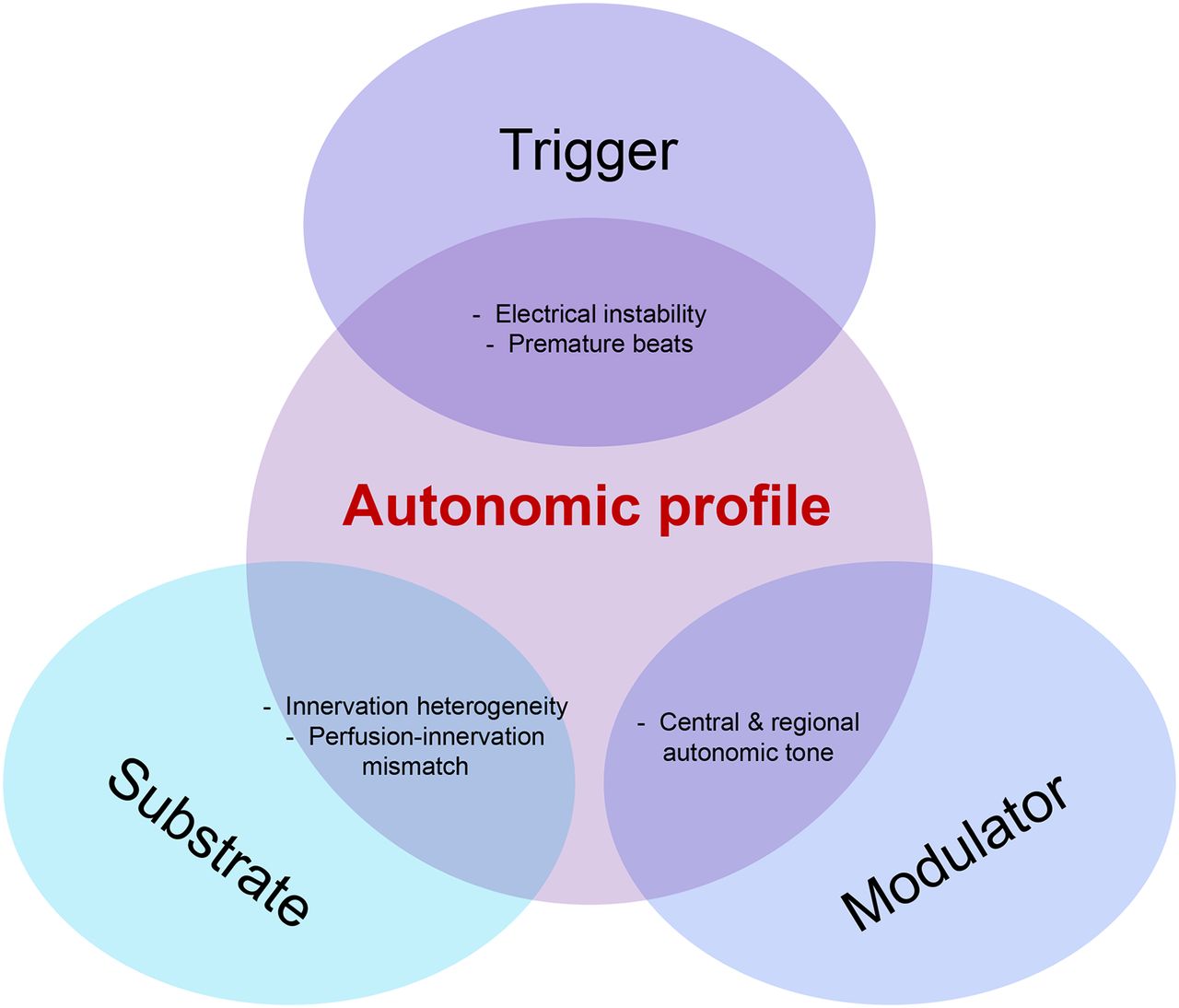
Mechanism of arrhythmia: importance of the autonomic profile.
Several risk stratifiers for SCD have been evaluated over the years (Table 1). In addition to traditional risk factors for coronary heart disease and significant comorbidity such as renal failure and diabetes, these stratifiers include, first, ventricular function (measured by LVEF evaluation by echocardiography, multigated acquisitions, or cardiovascular MR imaging); second, arrhythmias (Holter-electrocardiography [ECG] or implantable loop-recorders); third, electrical markers of substrates for arrhythmias (signal-averaged ECG and electrophysiology study); fourth, surface ECG variables such as T-wave alternans and QT dispersion; fifth, autonomic function (heart rate variability, heart rate turbulence, baroreflex sensitivity, and so forth); sixth, other more rarely used modalities for autonomic function such as blood sampling of norepinephrine spillover, microneurography, and vascular reactivity; and seventh, recently, the quantification of autonomic cardiac innervation (sympathetic nerve terminals) by a 123I-metaiodobenzylguanidine (MIBG) or PET scan. Additionally, several risk score algorithms and risk stratification strategies have been published that try to pinpoint which patients in the population identified by guidelines actually benefit from ICD therapy (31–33). In addition to lacking the appropriate sensitivity and specificity for life-threatening arrhythmias, no risk scoring system has been prospectively evaluated as a selection strategy for device therapy.
Risk Stratification Strategies for Prediction of Sudden Cardiac Death in Patients with Heart Failure
Among the available risk stratifications, depressed left ventricular systolic function is a well-established risk factor for SCD in larger cohorts, but it is hampered by a low predictive accuracy for the individual patient, as discussed previously. Data on myocardial scarring (evaluated by CMR) have the ability to predict the occurrence of ventricular arrhythmias (34), but a major limitation of CMR until now has been that it is expensive, requires considerable expertise, and is contraindicated for patients with ICDs. In retrospective studies, the technique seems promising, and total scar burden has been shown to correlate with arrhythmias in ICD-treated patients, but prospective randomized trials are lacking thus far (35,36). Microvolt T-wave alternans is derived noninvasively from a Holter monitor or high-fidelity electrocardiographic recordings during exercise and has been prospectively evaluated as a risk predictor in patients receiving ICDs, with variable results (37–41). Heart rate variability (HRV) evaluated using a Holter monitor is also noninvasive and readily accessible in most centers. It describes the variation in heart rate from beat to beat and can be represented in several ways, including a time domain and a frequency domain. The results can give information on the sympathovagal balance; a reduced HRV corresponds to impaired autonomic balance. HRV has been shown to provide prognostic information in addition to clinical data in an unselected population of patients with heart failure (42), and a reduced HRV is associated with a higher risk of SCD (43). All these investigative tools, although contributing to better understanding of either the substrate or the modulator, have lacked a sufficient positive predictive value to become mainstream selection strategies. Additionally, recent publications have highlighted the need for standardized testing in a setting that is likely to yield the best predictive value for the outcome of the test—for example, different types of autonomic response to stress testing or other tests that are easily obtained and can be readily interpreted (44).
SYMPATHETIC IMAGING: IS THERE A ROLE?
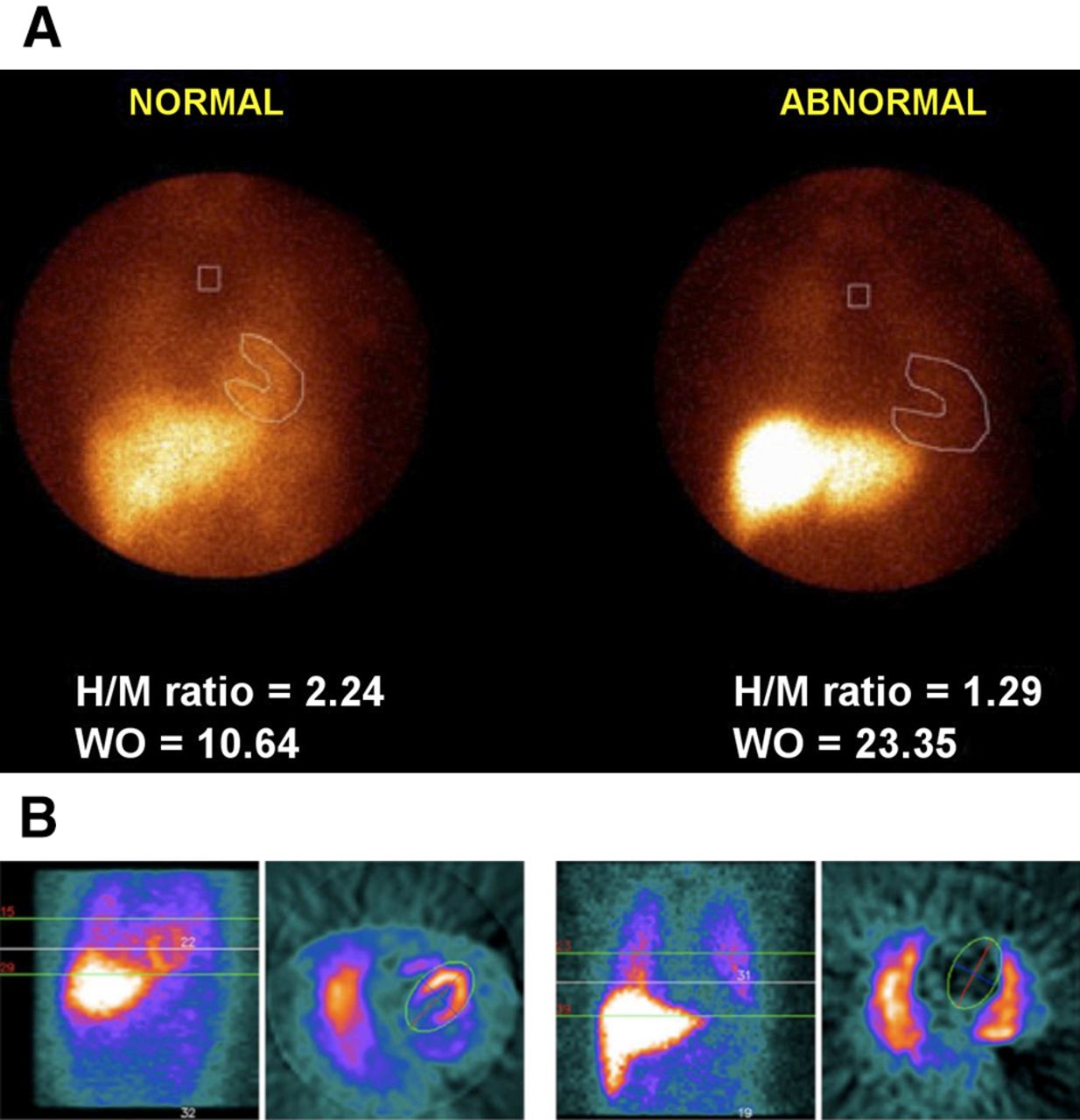
Because the autonomic nervous system can set off the trigger, influence the substrate, and perpetuate the arrhythmia, an investigative modality to better image and understand sympathetic nervous system activity seems quite fitting. Although approved for several years in European countries, the adoption of imaging of the sympathetic nervous system activity in heart failure has been limited in the United States. The 2013 approval of radioactive 123I-MIBG for imaging in heart failure by the Food and Drug Administration has brought radionuclide imaging of sympathetic innervation of the heart to the forefront again (45). The commonly used radiotracers are 123I-MIBG for planar and SPECT imaging and 11C-hydroxyephedrine for PET imaging. The most accepted measure of heart-to-mediastinal (H/M) ratio can be calculated using either planar imaging (area-based region of interest) or SPECT imaging (volume-based region of interest), as shown in Figure 2 (46,47).
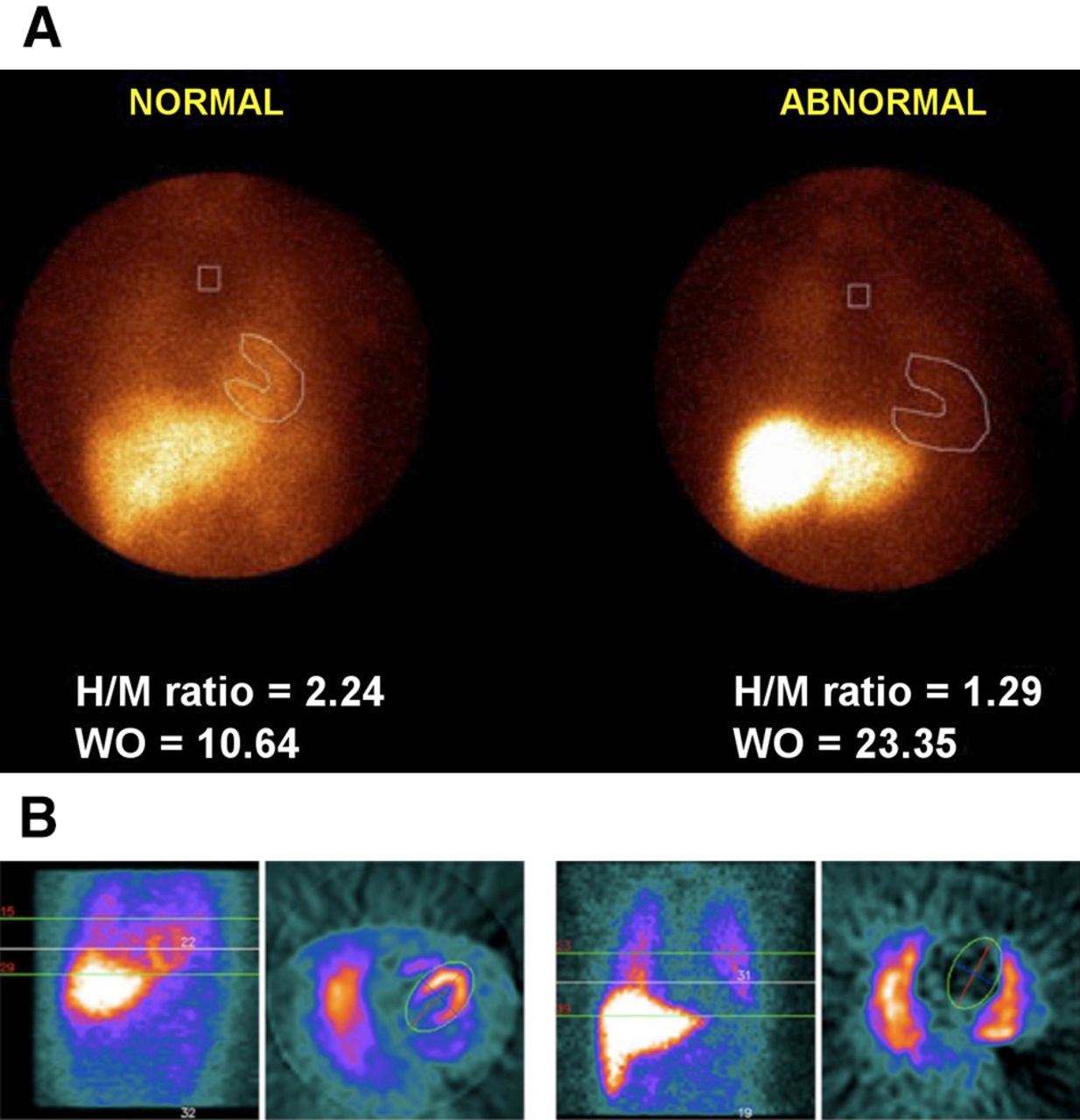
H/M ratio in normal heart (left) and heart with reduced cardiac autonomic innervation (right) imaged by planar 123I-MIBG scanning (A) and volume-based SPECT 123I-MIBG scanning (B). WO = washout. (Reprinted with permission of (47,66).)
Several insightful measures can be obtained from 123I-MIBG SPECT imaging. An assessment of the patient’s segmental 123I-MIBG tracer uptake can be made using the 17 left ventricular segments (48), and each myocardial segment is scored on a 5-point tracer uptake scale from 0, normal tracer uptake, to 4, no tracer uptake. A 123I-MIBG SPECT defect score is then obtained and defined as the summation of all the segmental tracer uptake scores. This score can then be combined with a perfusion technetium SPECT score obtained at the same investigation. By subtracting the perfusion defect score from the 123I-MIBG defect score, a size of mismatch is calculated—that is, myocardium with abnormal 123I-MIBG uptake but normal perfusion uptake. The reason for the mismatch is most likely that sympathetic nerve fibers are more vulnerable to ischemia than cardiomyocytes are; thus, the periinfarct region can be partially denervated, but the myocytes are fully viable. This region may then be particularly susceptible to triggering of ventricular arrhythmias and development of reentrant circuits due to innervation supersensitivity in combination with the damaged nerve fibers (49). Similar measures can be obtained using PET, and abnormal patterns of 11C-hydroxyephedrine retention have been identified in several groups of patients with ventricular tachycardias, including right ventricular arrhythmias (50,51), Brugada syndrome (52), and congenital long QT syndrome (53).
As mentioned previously, the best-studied modality in heart failure patients is 123I-MIBG planar imaging. Recently, a systematic review of 18 studies with a total of 1,755 patients evaluated the prognostic impact of 123I-MIBG imaging findings in patients with heart failure and found that the H/M ratio was indeed useful for predicting clinical outcome (54). Favorable left ventricular remodeling in heart failure patients has also been shown to correlate with improvement in sympathetic innervation by 123I-MIBG imaging; and data support that the changes in innervation are evident before remodeling, which is confirmed by other imaging modalities (55–57). There is also increasing evidence that a reduced H/M ratio correlates with an increased risk of arrhythmias and that it can provide incremental or better value than other risk stratification tools. In a study by Tamaki et al. (58) of patients with heart failure and an LVEF of 40% or less, the 123I-MIBG washout rate was a better predictor of SCD than other measures of autonomic function (QT dispersion or HRV). Other studies have also shown an independent correlation between SCD, spontaneous or induced malignant arrhythmias, and an abnormal H/M ratio (59–62). Other studies that have sought to investigate the physiology of the relationship have been unable to clearly demonstrate a correlation between the inducibility of ventricular arrhythmia during an electrophysiology study and the standard indices of 123I-MIBG imaging (61,63).
In the AdreView Myocardial Imaging for Risk Evaluation in Heart Failure (ADMIRE-HF) study (64), the largest prospective study, 961 heart failure patients had an initial 123I-MIBG scan performed and were then followed for cardiac events during a median of 17 mo. The results showed that an H/M ratio of less than 1.6 was highly predictive of major cardiac adverse events (New York Heart Association functional class progression, potentially life-threatening arrhythmic event, or cardiac death) and ventricular arrhythmia events in a population with symptomatic heart failure and an LVEF of 35% or less (Fig. 3) (64). Notably, the relationship for H/M ratio and mortality was linear, and mortality ranged from 0% in the group with an H/M ratio of 1.80 to 20% or more in the group with an H/M ratio of less than 1.10. In fact, there may be a role for the prediction of ventricular arrhythmias or SCD in patients who qualify for primary prophylactic ICD treatment (65), because the patients included in the study comprised those meeting criteria for primary prophylactic ICD treatment but without an ICD at the time of inclusion into the study. The investigators found that the independent predictors of arrhythmic events were lower systolic blood pressure (hazard ratio, 1.19 for each 10-point decrease), LVEF less than 25% (hazard ratio, 1.97), and 123I-MIBG–derived H/M ratio less than 1.6 (hazard ratio, 3.48). These findings, when incorporated into a risk score, were useful in risk-stratifying patients for serious life-threatening arrhythmias (46). It is evident that imaging the sympathetic nervous system may provide additional insight into the myocardial substrate and its vulnerability to arrhythmias.
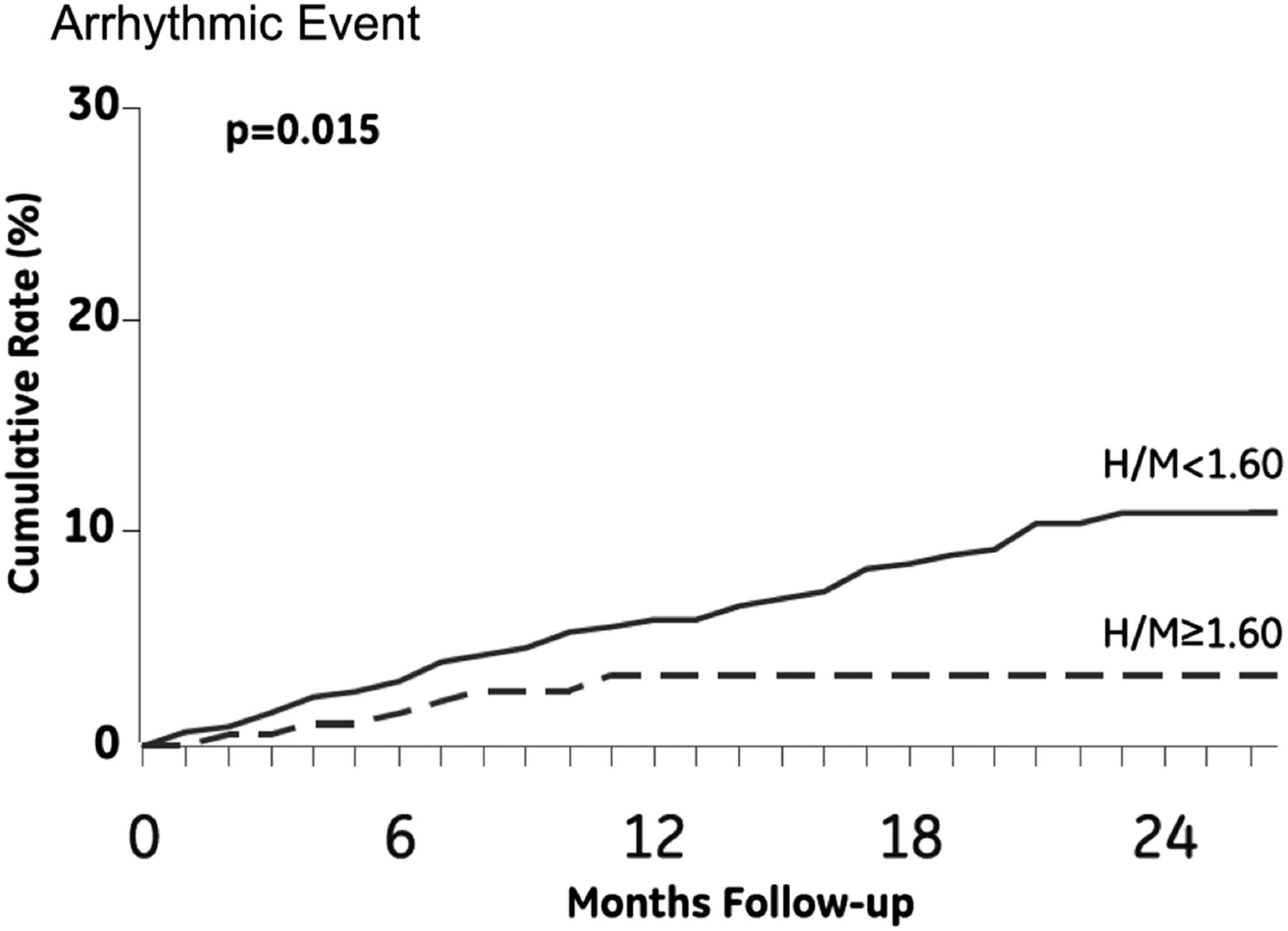
Risk of arrhythmic event stratified for H/M ratio in ADMIRE-HF study. (Reprinted with permission of (64).)
Ideally, data from imaging the autonomic nervous system should be used to complement existing risk-stratification models for SCD and ventricular arrhythmias. By appropriately quantifying the degree of autonomic dysfunction, these data could be incorporated into summative risk scores. This strategy has the potential to fill gaps of knowledge, especially for patients at increased risk of ventricular arrhythmias who currently fall outside guideline recommendations, such as those with moderately reduced ejection fraction. Another challenging category is patients with low ejection fraction but without any other indicators of increased risk.
However, many gaps remain in our understanding of the autonomic tone within an individual and the implications this may have on the occurrence of life-threatening arrhythmias. Although sympathetic nerve imaging may have the potential to better select patients for device therapy, it is probably the interaction between the extent and distribution of myocardial sympathetic denervation with the central autonomic tone that incites the arrhythmic event. The major challenges in the arena of risk stratification for sudden death include the accurate identification of patients with a low ejection fraction who are at a low risk for arrhythmias and who may not need an ICD, while simultaneously providing recognition of high-risk patients with an LVEF of 35% or greater who may benefit from an ICD. Understanding the sympathetic nervous system seems like a good next step in stratifying patient risk, but prospective randomized trials will be required before risk stratification can become a mainstream strategy.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication December 15, 2014.
- Accepted for publication March 4, 2015.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.