


Article Figures & Data
Figures
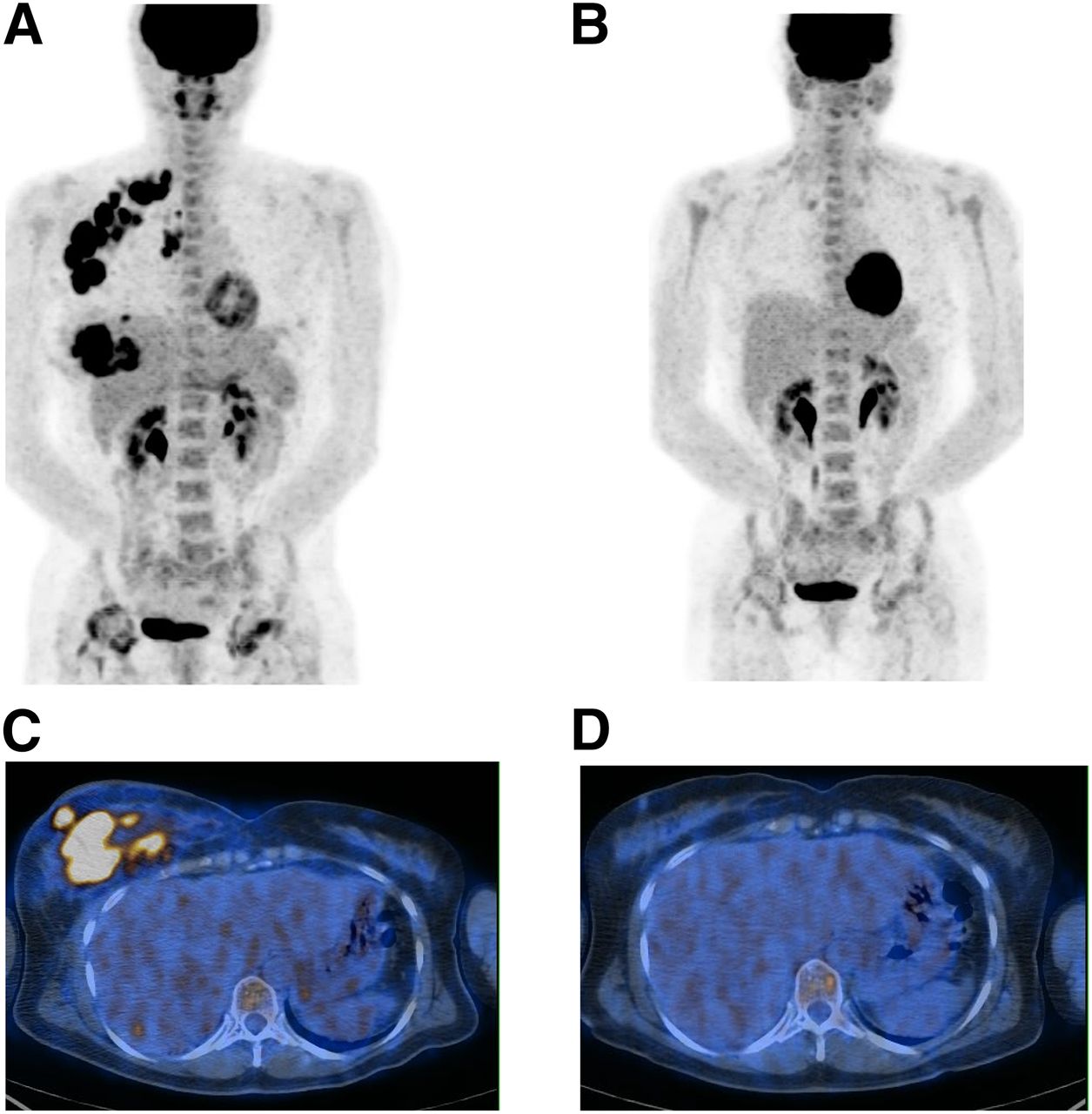
- FIGURE 1.
A 51-y-old woman with primary right IBC, axillary lymph node involvement, and pulmonary infection. IBC was grade 3 HR-negative/HER2-positive, with Ki-67 of 67.8%. (A and C) PET1 maximum-intensity projection image (A) and axial slice at level of breast (C). (B and D) PET2 maximum-intensity projection image (B) and axial slice at level of breast (D). ΔSUV1–2 and ΔSUV1–3 were −95%. Patient received 4 courses of anthracycline-based chemotherapy and 4 courses of taxane and trastuzumab. Pathologic complete response was found at surgery.
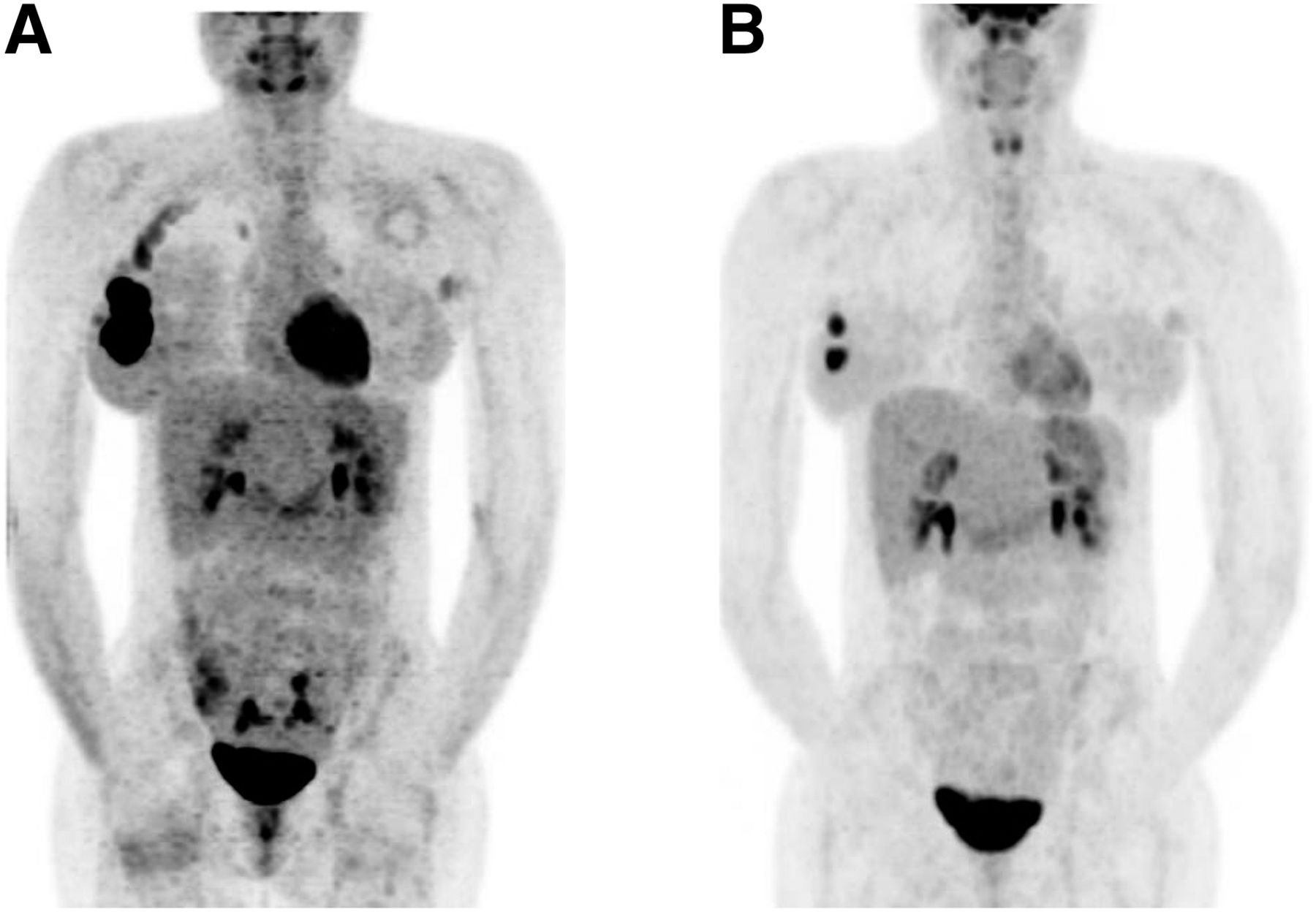
- FIGURE 2.
A 35-y-old woman with primary right IBC and affected axillary lymph node: PET1 (A) and PET3 (B) maximum-intensity projections. ΔSUV1–3 was −16.7%. IBC was grade 3 triple-negative, with Ki-67 of 30%. Patient received 6 courses of anthracycline-based chemotherapy. Nonpathologic complete response was found at surgery.
- FIGURE 3.
Capacity of ΔSUV 1–3 to predict residual tumor at surgery after completion of NACT, derived by area under receiver-operating-characteristic curve (0.75).


Tables
Characteristic Overall population pCR group Non-pCR group Patients (n) 23 5 (22%) 18 (78%) Age (y) Mean ± SD 51 ± 12.7 50.6 ± 9.9 52.2 ± 13.3 Range 34−78 37–60 34–78 Histology Invasive ductal carcinoma 22 (95%) 4 (80%) 18 (100%) Metaplastic carcinoma 1 (5%) 1 (20%) Elston–Ellis grade I 2 (9%) 2 (11%) II 7 (30%) 7 (39%) III 14 (61%) 5 (100%) 9 (50%) HR status Positive 11 (43%) 1 (20%) 10 (55%) Negative 12 (57%) 4 (80%) 8 (45%) HER2 receptor status Positive 5 (22%) 2 (40%) 3 (17%) Negative 18 (78%) 3 (60%) 15 (83%) Triple-negative cancer 7 (30%) 2 (40%) 5 (28%) Ki-67 <25% 7 (30%) 1 (20%) 6 (33%) ≥25% 14 (61%) 4 (80%) 10 (55%) Unknown 2 (9%) 2 (12%) NACT Anthracycline alone 14 (61%) 4 (80%) 10 (55%) Anthracycline and docetaxel 9 (39%) 1 (20%) 8 (45%) Clinical response Complete response 5 (22%) 3 (60%) 2 (11%) Partial response 15 (65%) 2 (40%) 13 (72%) Stable disease 3 (13%) 3 (17%) Survival parameters (mo) DMFS (distant metastasis-free survival) 52.6 46 54 Overall survival 73.9 79.5 72.4 Patient no. Grade HR status HER2 status Treatment SUV1 ΔSUV1–2 ΔSUV1–3 Clinical response Pathologic response 1 3 Neg Neg Anthracycline-based × 6 25 −62.8% −70% PR Non-pCR 2 3 Neg Neg Anthracycline-based × 4, docetaxel × 4 3.9 −43.6% −41% PR Non-pCR 3 1 Pos Neg Anthracycline-based × 6 4.3 −72% −72% PR Non-pCR 4 2 Pos Neg Anthracycline-based × 6 14 −50% −64.3% PR Non-pCR 5 1 Pos Neg Anthracycline-based × 6 14 −2.1% −88.6% PR Non-pCR 6 2 Neg Pos Anthracycline-based × 6 4.9 −81.6% −89.8% CR Non-pCR 7 3 Neg Pos Anthracycline-based × 6 16 −84.4% −93.8% PR Non-pCR 8 2 Pos Neg Anthracycline-based × 6 8 −50% −68.8% PR Non-pCR 9 2 Neg Pos Anthracycline-based × 4, docetaxel × 4 3.4 −61.5% −61.8% PR Non-pCR 10 3 Neg Neg Anthracycline-based × 6 6 −16.7% −16.7% SD Non-pCR 11 3 Pos Neg Anthracycline-based × 6 10 −40% −70% PR Non-pCR 12 2 Pos Neg Anthracycline-based × 6 5.4 −61.1% −64.8% PR Non-pCR 13 3 Pos Neg Anthracycline-based × 6 10.9 −72.5% −86.2% CR Non-pCR 14 2 Pos Neg Anthracycline-based × 3, docetaxel × 3 11.9 −65.5% −71% PR Non-pCR 15 3 Pos Neg Anthracycline-based × 6 3.2 0% −43.8% SD Non-pCR 16 2 Neg Neg Anthracycline-based × 4, docetaxel × 4 13.2 −63.6% −78.8% SD Non-pCR 17 3 Neg Neg Anthracycline-based × 3, docetaxel × 3 12 −79.2% −90.8% PR Non-pCR 18 3 Pos Neg Anthracycline-based × 4, docetaxel × 4 4.1 −78% −87.8% PR Non-pCR 19 3 Pos Neg Anthracycline-based × 6 12.1 −71.1% −91.7% PR pCR 20 3 Neg Pos Anthracycline-based × 3, docetaxel-trastuzumab × 4 22 −95.5% −95.5% CR pCR 21 3 Neg Neg Anthracycline-based × 6 16 −70% −87.5% CR pCR 22 3 Neg Pos Anthracycline-based × 3, docetaxel-trastuzumab × 3 6.6 −50% −66.7% PR pCR 23 3 Neg Neg Anthracycline-based × 4, docetaxel × 4 12 −25% −81% CR pCR Neg = negative; Pos = positive; PR = partial response; CR = complete response; SD = stable disease.
Variable P ΔSUV1–3 0.0128 Clinical response 0.0280 Histologic grade 0.0384 Age 0.1078 Pathologic response 0.1321 Hormone receptor status 0.2270 HER2 status 0.6391 Pathologic response Survival (mo) Molecular subtype n pCR Non-pCR SUVmax, PET1 ΔSUV1–3 DMFS OS HR-positive/HER2-negative 11 1 10 9.5 ± 3.8 −69% ± 18 70.2 94.3 HR-negative/HER2-positive 5 2 3 16.7 ± 5.3 −94% ± 17 45.8 78.7 Triple-negative 7 2 5 12.5 ± 7 −85% ± 27 36.7 63.7 DMFS = distant metastasis-free-survival; OS = overall survival.





{kind=link}
{kind=link}
{kind=link}