


Abstract
Ionizing radiation–induced DNA double-strand breaks (DSBs) can lead to cell death, genome instability, and carcinogenesis. Immunofluorescence detection of phosphorylated histone variant H2AX (γ‐H2AX) is a reliable and sensitive technique to monitor external-beam ionizing radiation–induced DSBs in peripheral blood lymphocytes (PBLs). Here, we investigated whether γ-H2AX could be used as an in vivo marker to assess normal-tissue toxicity after extended internal irradiation with 177Lu-DOTA-octreotate (LuTate) peptide receptor radionuclide therapy (PRRT) of neuroendocrine tumors. Methods: We analyzed the kinetics of γ-H2AX foci in PBLs of 11 patients undergoing PRRT. The number of γ-H2AX foci was determined before and up to 72 h after treatment. These values were compared with the estimated absorbed dose to blood, spleen, bone marrow, and tumor and with subsequent PBL reduction. Results: The decrease in 177Lu activity in blood with time followed a biexponential kinetic pattern, with approximately 90% of circulating activity in blood cleared within 2 h. Absorbed dose to blood, but not to spleen or bone marrow, correlated with the administered 177Lu activity. PRRT increased γ-H2AX foci in lymphocytes in all patients, relative to pretherapy values. The response varied significantly between patients, but the average number of foci indicated a general trend toward an increase at 0.5–4 h with a subsequent decrease by 24–72 h after treatment. The peak number of foci correlated with the absorbed dose to tumor and bone marrow and the extent of PBL reduction. Conclusion: γ-H2AX can be exploited in the LuTate PRRT as a biomarker of PBL cytotoxicity. Long-term follow-up studies investigating whether elevated residual γ-H2AX values are associated with acute myelotoxicity and secondary blood malignancy may be worthwhile.
Peptide receptor radionuclide therapy (PRRT) using radiolabeled somatostatin analogs that bind to somatostatin receptor 2 has proven effective in treating patients with metastatic or inoperable neuroendocrine tumors (1,2). One of the most promising radiolabeled somatostatin analogs for tumor-targeting therapy is 177Lu-DOTA-octreotate (LuTate) (1,3).
PRRT is a safe treatment, but mild hematologic toxicity is frequently observed. Repeated administration of PRRT increases the accumulated dose to normal tissues and thereby increases the risk of accumulation of unrepaired DNA damage that can lead to genetic instability and, potentially, to carcinogenesis. In addition to acute myelotoxicity, myelodysplastic syndrome (MDS) has been reported in 4 of 504 patients in one series (4,5). To estimate the effect of PRRT and limit the toxicity of such treatment, organ dosimetry based on radioisotope biodistribution and kinetics is desirable. However, the image-based dosimetry findings alone have not been very useful for predicting development of blood disorders in individual patients (4). Furthermore, there is no consensus on an appropriate radiobiologic model for short-range, low–dose-rate radiopeptides. Studying DNA damage at the single-cell level could provide additional insight into the mechanisms of PRRT-induced toxicity and be useful in combination with organ dosimetry to determine or predict the biological consequences of radiation dose in vivo.
Phosphorylated histone H2AX (γ-H2AX), a biomarker of radiation-induced DNA double-strand breaks (DSBs) (6), is commonly used to monitor DNA damage and repair in a wide range of applications including radiotherapy (7,8). External ionizing radiation induces γ-H2AX foci in a dose-dependent manner. The maximum size and number of foci are observed at 30 min after ionizing radiation and subsequently decline to pre–ionizing radiation levels within several hours because of DSB repair. The direct response to radiation and the sensitivity of the assay have provided a basis for the adoption of γ-H2AX as a “biodosimeter” to evaluate exposure of peripheral blood lymphocytes (PBLs) after external body irradiation (9–13). Recent publications evaluated the γ-H2AX assay as an attractive functional assay for identification of radiosensitive individuals with early or chronic radiation-induced normal-tissue toxicity and for personalized therapy (7,14,15).
The kinetics of radiopharmaceutical-induced DNA damage are more complex than those induced by external ionizing radiation, reflecting the nature of radionuclide emissions, biodistribution of the agent within cells and organs, and time course of radiation delivery determined by physical decay characteristics of the radionuclide and tissue clearance kinetics. Current data on the use of γ-H2AX as a biomarker of toxicity and as a biodosimeter after systemic administration of radiopharmaceuticals come primarily from studies investigating 131I therapy in patients with thyroid cancer (16,17) and from 18F-FDG PET/CT imaging (18). These studies recommended γ-H2AX as a biomarker of DNA damage after internal irradiation. However, because the spatial distribution of ionization events on a microscopic scale is related to the chemical form of the radiopharmaceutical and the energy of the β particles (affecting the proportion of DNA single-strand breaks and DSBs), the use of γ-H2AX should be validated for specific radiopharmaceuticals.
This study aimed to assess DNA damage in PBLs at multiple time-points after LuTate PRRT and to correlate the number of γ-H2AX foci with the estimated absorbed radiation dose to blood, spleen, bone marrow, and tumor. We assessed the impact of tumor volume and whether nadir lymphocyte counts were related to the level of DSBs. We investigated whether γ-H2AX could be used as a biodosimeter to estimate the absorbed dose or predict normal-tissue toxicity to PRRT.
MATERIALS AND METHODS
Patient Treatment
The 11 patients who were enrolled in the study (5 women and 6 men; mean age, 56 y; range, 32–65 y) had neuroendocrine tumors and underwent one or more PRRT cycles (Table 1). The trial was approved by the Peter MacCallum Cancer Centre Human Ethics Committee. All patients signed a consent form. The standard induction course of PRRT comprised 3–5 cycles of LuTate therapy given every 6 wk to every 9 wk. LuTate was given in combination with an infusion of amino acids (25 g of arginine and 25 g of lysine in 1 L over 4 h) for renal protection. Nine patients received infusions of 5-fluorouracil (5-FU) (200 mg/m2/24 h) 1–3 d before LuTate injection and continuing for a total of 14 d as a radiosensitizing agent (1).
Demographics and Characteristics of Patients
A description of blood collection and processing, dosimetry, and data analysis is found in the supplemental data (available at http://jnm.snmjournals.org).
RESULTS
Dosimetry
Patients received an administered activity of 6,500–10,000 MBq of 177Lu, resulting in a mean cumulative absorbed dose of 42 ± 3.9 mGy to blood (median, 42 mGy; range, 22–57 mGy), 250 ± 21 mGy to bone marrow (median, 210 mGy; range, 170–410 mGy), 3,700 ± 650 mGy to spleen (median, 3,300 mGy; range, 1,700–10,000 mGy), and 22,000 ± 12,000 mGy to tumor (median, 20,000 mGy; range, 6,000–46,000 mGy) (Table 2).
Dosimetry
Initial LuTate uptake, typically seen at 4 h in spleen, kidneys and bladder on SPECT/CT scans, cleared substantially after 24 h (Supplemental Fig. 1). Consequently, primarily the tumor was detectable at 72 h.
The time–activity curve of LuTate in the blood (Fig. 1) for the study series followed a biexponential function. The clearance half-time for the first exponent was 0.72 h, with 89% ± 2.6% of LuTate clearing within 2 h. The remaining radioactivity was then gradually cleared from the blood, reaching less than 1% at 72 h with a clearance half-time of 35.7 h. The high LuTate uptake in kidneys and bladder at early time-points and clearance at 24 h usually indicate that this radiotracer is cleared primarily by renal excretion.

LuTate time–activity curve in blood up to 72 h after treatment. Each point represents single measurement of radioactivity in the blood of 11 patients at indicated times. Solid line is biexponential fit of LuTate disappearance from blood.
Kinetics of LuTate Therapy–Induced γ-H2AX Foci in PBL
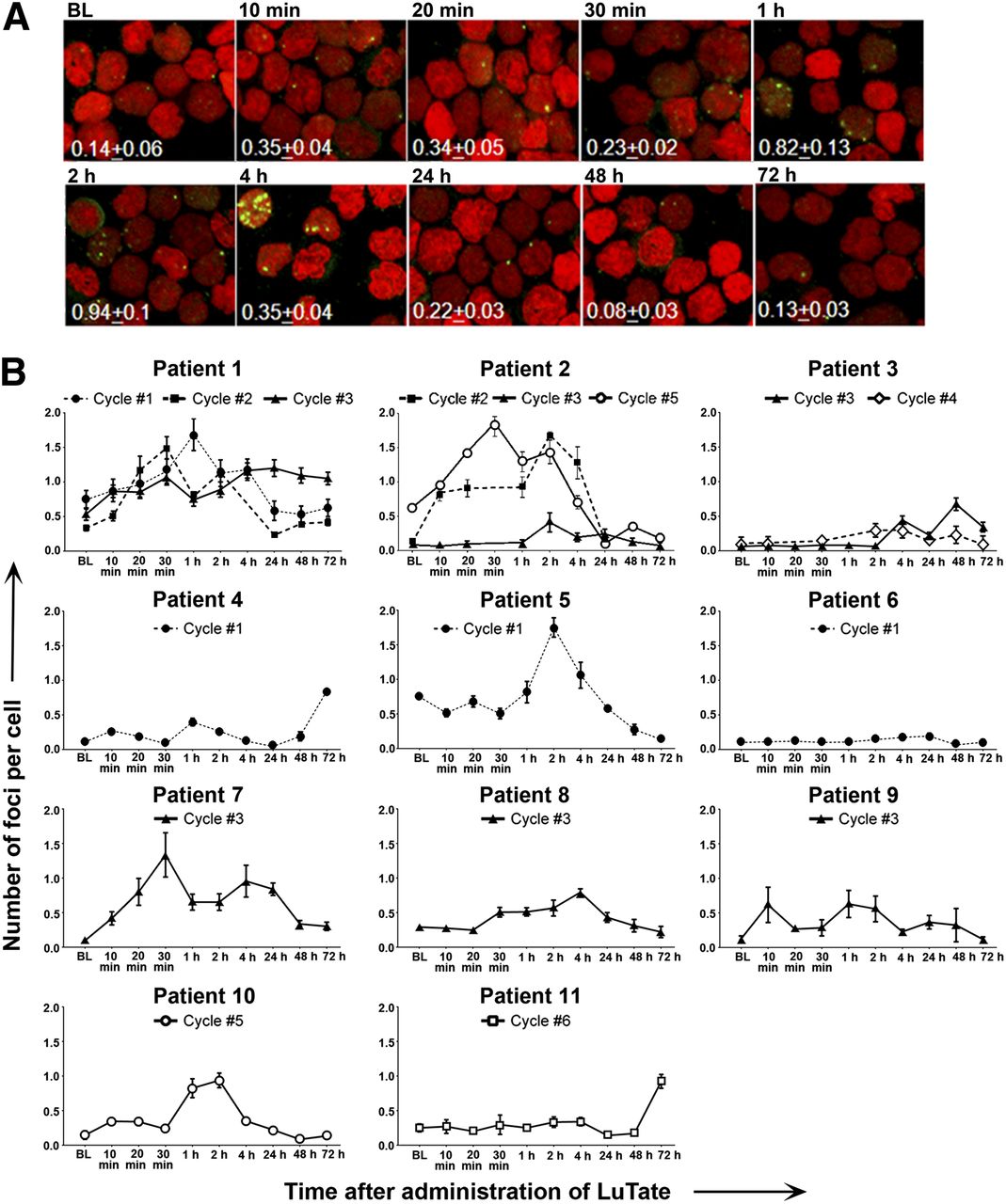
Individual data for each patient revealed that the pattern of γ-H2AX kinetics varied greatly between patients (Fig. 2). Additionally, differences between cycles were observed within the same patients (Fig. 2B). A peak of γ-H2AX foci per cell was observed at different time points in similar PRRT cycles. Conversely, similar patterns of γ-H2AX foci kinetics were seen in some patients who received different numbers of PRRT cycles. In the interval from 10 min to 72 h after therapy, all patients showed an excess of γ-H2AX foci per cell (defined as the number of foci per cell at each time point minus the number of foci per cell at baseline). However, in some cases, the peak number of excess foci per cell was very low, for example, in patients P2.3 (0.3 foci per cell above baseline), P3.4 (0.2 foci per cell above baseline), and P6.1 (0.1 foci per cell above baseline). Interestingly, in patients P4.1 and P11.6 the peak number of excess foci per cell was detected only at 72 h after LuTate administration.
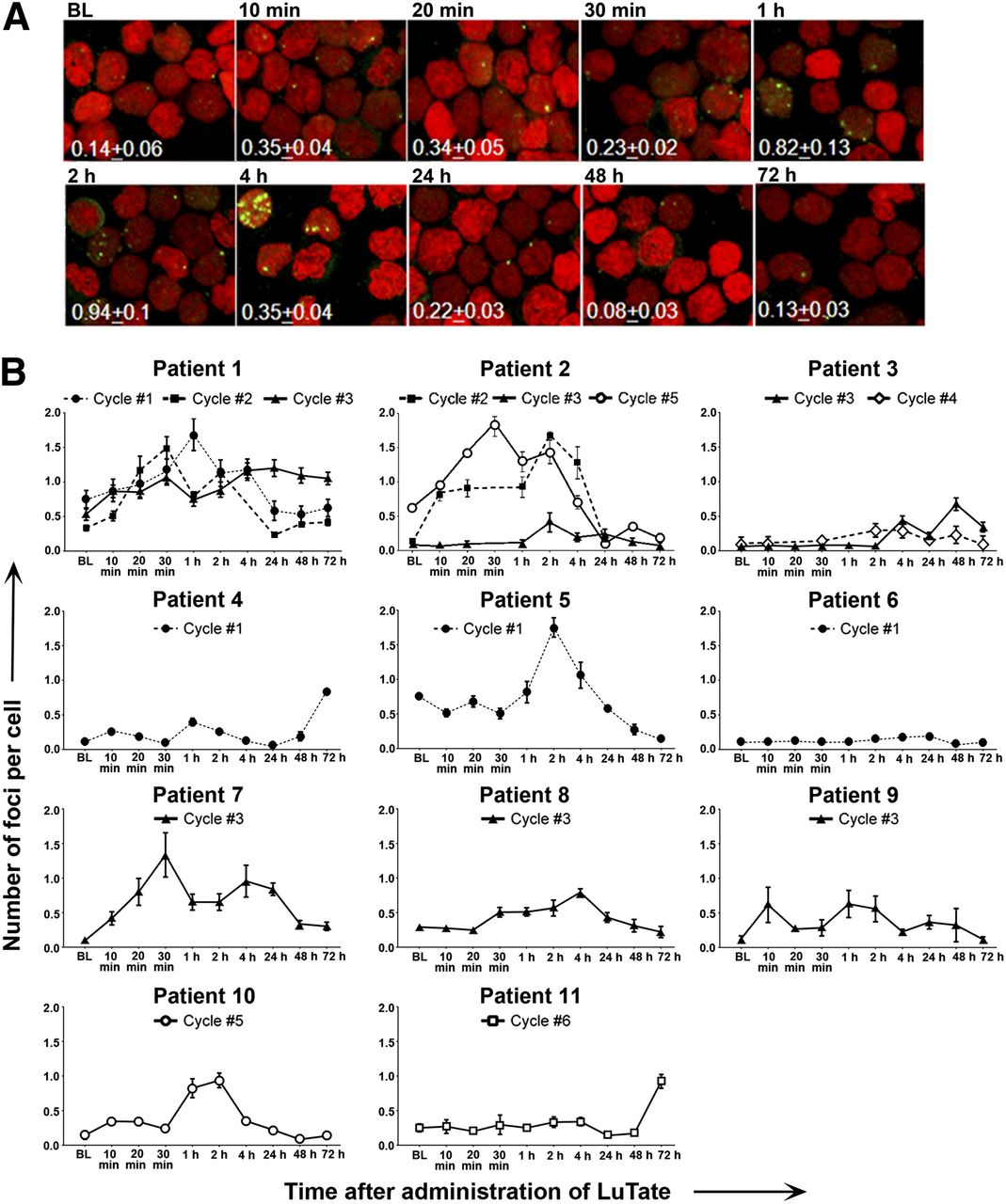
Kinetics of γ-H2AX foci formation in PBLs. (A) Representative confocal images of γ-H2AX foci (green) and nuclei (red, DNA) of patient P10.5 after administration of 8,362 MBq of LuTate. Values correspond to average number of foci per cell ± SEM. (B) Number of foci per cell in individual patients measured at baseline (BL) before therapy and 10, 20, and 30 min and at 1, 2, 4, 24, 48, and 72 h after LuTate administration in one or more cycles of therapy.
The pretreatment level of γ-H2AX foci per cell ranged between 0.06 and 0.75, with an average of 0.28 ± 0.06 foci per cell. Administration of the radiosensitizing agent 5-FU before PRRT (in 12 of 16 analyzed treatment cycles) increased the baseline value 2-fold (0.15 ± 0.04 without 5-FU and 0.33 ± 0.08 with 5-FU, P = 0.049). In patient P2, 5-FU was not given at cycle 2, but this PRRT cycle induced a γ-H2AX response similar to cycle 5, with 5-FU. The lowest γ-H2AX response was observed in patients P4.1, P6.1, and P11.6 without 5-FU administration. However, these events may not be related, since a similar low-level response was observed also in patients P2.3 and P3.3–4, who received 5-FU.
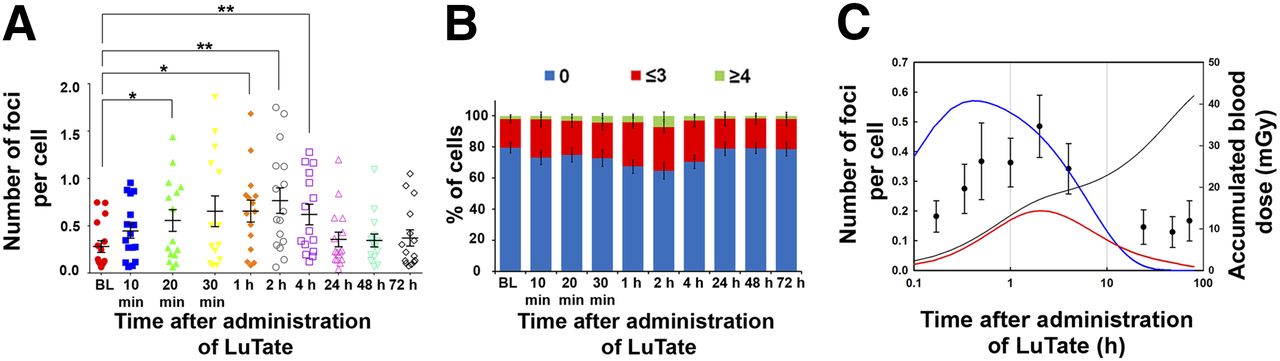
The average numbers of γ-H2AX foci per cell increased rapidly in the first 30 min after LuTate administration (Fig. 3A) and gradually increased in the following 2 h when the average numbers of γ-H2AX foci peaked. Subsequently, the numbers of foci gradually returned close to baseline at 24 h. Similarly, the percentage of cells with multiple foci increased up to 2 h (2 h vs. baseline, P = 0.0103) before decreasing at later time points (Fig. 3B).
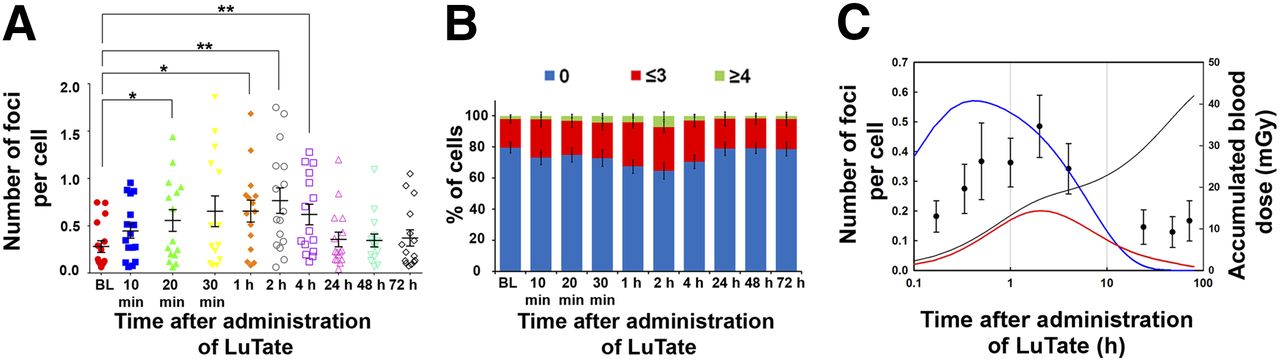
Analysis of γ-H2AX foci formation in PBLs. (A) Number of foci per cell vs. time after PRRT for individual patient. Black horizontal bar and error bars represent mean ± SEM of 14–16 samples. (B) Fraction of cells with no foci (blue bars), ≤3 foci (red bars), and ≥4 foci (green bars) (mean ± SEM, n = 14–16). (C) Simulation of number of foci per cell as function of time after PRRT. Symbols represent average experimental values across all patients ± SD. Simulation was implemented for radiation dose of 42 mGy delivered as pulse (blue line) or accumulated (red line) within 80-h interval. Accumulated dose was calculated according to LuTate kinetics in blood (black line). *P < 0.05, Mann–Whitney test, for baseline vs. other time points. **P < 0.01, Mann–Whitney test, for baseline vs. other time points.
We simulated the γ-H2AX kinetics in PBLs assuming that the major source of DNA damage in PBLs comes from LuTate irradiation in blood (red line in Fig. 3C). The simulated kinetics for gradual accumulation of the dose (black line in Fig. 3C) to a total value of 42 mGy (average blood dose) is based on the course of LuTate elimination from the blood (Fig. 1). For comparison, we included the simulated γ-H2AX kinetics for a single 42-mGy dose at the start of the 80-h period (blue line in Fig. 3C). Compared with a single instantaneous dose, the simulation of the isotope decay scenario with protracted dose delivery better predicts the time course of experimental data for accumulation and decay of γ-H2AX foci. However, the overall predicted level of foci is less than experimental values.
PRRT Toxicity on PBL
The number of total PBLs was assessed before each PRRT cycle and 2 wk after treatment (Table 3). Early toxicity was observed in all patients. The average PBL reduction from pretreatment to 2 wk after the first PRRT cycle was 51% (n = 4; range, 33%–63%). The extent of reduction generally decreased for successive treatment cycles; for example, 42% for the third cycle (n = 6; 20%–56%) down to 12% for 6 cycles (1 case only). However, the 2 cases for the fifth cycle were outliers for this trend (average of 45% reduction). The number of PBLs increased between cycles but did not return to the levels observed before the first treatment, indicating that there was only a partial recovery after each cycle. The overall reduction of PBLs from the start of treatment to 2 wk after completion of multiple cycles of PRRT was 68% (average of 12 patients; 34%–88%).
Lymphocyte Toxicity After PRRT
Relationships Between Foci Count, Dosimetry, and PBL Reduction
We investigated the correlation between various γ-H2AX foci endpoints with absorbed doses in blood at 2 and 72 h or absorbed doses in spleen, bone marrow, and tumor. The endpoints were the peak number of excess foci per cell within either 10 min–4 h or 24–72 h after PRRT, or over the total observation interval. The analysis revealed no clear correlation for most parameters (Supplemental Fig. 2), including the dose in blood at 2 h after LuTate administration (Fig. 4A). Because radioactivity clears rapidly (Fig. 1), this short circulation time would be temporally loaded toward early radiation exposure. Therefore, the absorbed dose to blood was expected to correlate with the peak of damage to lymphocytes around that time. However, no correlation was found. This lack of correlation applies to all data points involved and to correlation for different cycles within an individual patient. The best correlative trend was found between peak number of excess foci per cell and tumor dose (Fig. 4B, with the exception of a single outlier, patient P6.1, who exhibited the lowest γ-H2AX response) and bone marrow dose (Fig. 4C). Again, with the exception of P6.1, a positive correlative trend was observed between peak number of excess foci per cell in the 10-min to 4-h interval and fraction of lymphocyte reduction within the corresponding cycle (Fig. 4D). Absorbed dose to blood but not to spleen or bone marrow correlated with administered 177Lu activity (Supplemental Fig. 2A).

Correlation studies. (A) Peak number of excess foci per cell in 10-min to 4-h interval vs. dose to blood at 2 h. (B) Peak number of excess foci per cell in 24- to 72-h interval vs. tumor dose. (C) Peak number of foci per cell in 10-min to 4-h interval vs. dose to bone marrow. (D) Peak number of excess foci per cell in 10-min to 4-h interval vs. lymphocyte reduction 2 wk after treatment. Data for different treatment cycles of same patient are shown as blue (P1), green (P2), and black (P3) symbols; other data points are shown as red symbols. Red lines represent linear regression for all points.
DISCUSSION
Numerous preclinical and clinical studies have reported the linear radiation dose response of the γ-H2AX assay (9–13,19–22). Clinical studies have demonstrated that the stochastic γ-H2AX foci values after external radiation exposure depend on the dose, exposed area of the body, duration or fractionation of the exposure, and time of analysis. In cancer patients treated with 3-dimensional conformal radiotherapy for a variety of tumor types, a linear correlation was established between the integrated total-body radiation dose and γ-H2AX foci per lymphocyte (13), making it possible to estimate the applied integral body dose. Moreover, the γ-H2AX–based measurements in exposed PBLs were in concordance with the physical dosimetry of IMRT and the 3-dimensional treatment modalities of prostate cancer (23). Therefore, the assay demonstrates the characteristics of a reliable biodosimeter for external-beam radiotherapy (7).
To our knowledge, this study represents the first exploration of the γ‐H2AX assay in PBLs for PRRT with 177Lu-octreotate. Despite some inter- and intraindividual variability, the average number of γ-H2AX foci for the whole study group increased rapidly within the first 30 min after PRRT and more slowly from 30 min to 2 h. Repair mechanisms prevail over DNA DSB formation between 2 and 24 h after treatment, resulting in progressive disappearance of γ-H2AX foci. PRRT-induced lymphopenia has been reported previously (24). Because circulating lymphocytes are traversed by radiation tracks from 177Lu, the absorbed dose to blood would be most likely to correlate with DNA damage to PBLs. Indeed, we found that lymphocyte counts dramatically reduced after the first cycle of LuTate in all patients. Importantly, the peak number of excess foci per cell in the 10-min to 4-h interval correlated with subsequent PBL reduction.
It is unlikely that lymphocyte depletion was due solely to direct irradiation since the absorbed dose in blood is 20- to 50-fold lower (mGy range) than the dose needed to achieve 10%–20% cell death (≥1 Gy). Indeed, no correlation between peak number of excess foci per cell and absorbed dose in blood was found. Moreover, although the kinetics of foci formation followed the trend predicted by the simulation on the basis of gradual accumulation of absorbed dose in blood, the predicted level of γ-H2AX foci was substantially less than the experimental values. These results indicate that the dose in blood only partially accounts for the induction of γ-H2AX foci in lymphocytes. On the basis of the correlation studies, the tumor dose also contributes to foci formation in lymphocytes. This finding is consistent with larger doses to tumors by at least one order of magnitude compared with other organs (Table 2). The peak number of excess foci per cell also correlated with the dose to bone marrow, suggesting its possible contribution to the damage in PBLs.
The residual number of foci in several patients 24–72 h after treatment generally did not decrease as much as predicted by the simulation. Possible explanations include inefficient DNA repair or mobilization of lymphocytes with LuTate-induced DNA damage from high-uptake tissues (spleen, bone marrow, and tumor) into the circulation. It may be possible to improve the correlation between dose in blood and PBL γ-H2AX response by incorporating residence time of these lymphocytes into high-uptake tissues in the calculations. The absorbed dose to bone marrow can affect the genomic stability of progenitor cells and their progeny. Individual radiation sensitivity influences large variability in clinical response to radiotherapy, as well as cellular radiosensitivity measured by the γ-H2AX assay in PBLs (7,14,15). There is also an ongoing debate on the mechanisms of the radiation-induced bystander effect (25), which may contribute to an elevated appearance of dose to circulating lymphocytes through reactive oxygen and nitrogen species and immune response.
Our findings are in line with previous studies showing similar patterns of γ-H2AX foci kinetics after a single dose of 131I therapy in patients with differentiated thyroid cancer (16,17) or after injection of 18F-FDG in patients with various malignant or benign diseases (18). Interestingly, radiopharmaceuticals with different biodistributions, pharmacokinetics, and dose rates showed similar patterns of DNA DSB induction and repair. However, the peak values were found earlier with a diagnostic dose of 18F-FDG (30 min) (18) than with therapeutic doses of LuTate or 131I (2 h for both radiopharmaceuticals) (17). This observation is most likely due to the shorter physical half-life of 18F (109.8 min) than of 177Lu (6.7 d) and 131I (8 d).
One limitation of our study is that patients received varied administered activities of LuTate and some did not receive 5-FU. Administration of 5-FU before PRRT significantly increased the background level of γ-H2AX foci. This finding is consistent with studies showing that 5-FU causes DNA damage in various cancer types (26,27) and in lymphocytes (28). In the latter study, elevated DNA damage remained for 80 d after completion of treatment. Therefore, intrapatient variability in the level of γ-H2AX foci reported here could come from variations in the pharmacokinetic parameters, possibly due to the different administered activities between cycles or to the inclusion of 5-FU in the therapy regimen. Because clinical studies at our and other institutions have shown that adding 5-FU to LuTate may be beneficial to neuroendocrine tumor patients (1,29) and that dosimetry to tumor and normal tissues may relate to tumor burden (3), it may be worthwhile to reassess the utility of γ-H2AX foci in a standardized dosimetry-based trial of LuTate and 5-FU.
Stem and progenitor cells residing in lymphoid tissues (bone marrow, spleen) are also exposed to radiation. The absorbed doses to these organs and induction of DNA damage may be of concern given that MDS has been associated with prior anticancer therapy and abnormal DNA repair (30). In particular, increased γ-H2AX levels in bone marrow have correlated with poor overall survival in MDS patients (31). MDS can progress to acute myeloid leukemia, a genomic instability disorder. In our study, patients were followed up for 1 y. No serious adverse myelotoxic events related to LuTate treatment were recorded, apart from one patient who died from leukemia during the follow-up period. However, this patient had an elevated white blood cell count before PRRT, and review of the peripheral blood film suggested that this condition preceded LuTate PRRT. Whether the kinetics of γ-H2AX induction and repair correlate with the risk of secondary hematologic malignancy in LuTate-treated patients remains to be confirmed with longer-term follow-up studies.
CONCLUSION
The complexity of PRRT precludes a simple correlation between physical dosimetry and clinical endpoints with the γ-H2AX response in PBLs. Nevertheless, a correlation between decrease in PBLs and peak γ-H2AX foci numbers was found. The absorbed dose to blood, bone marrow, and tumor can account for the induction of γ-H2AX foci in PBLs. Overall, our results warrant a larger clinical study of elevated γ-H2AX levels and a risk of lymphopenia, MDS, and secondary malignancy in LuTate-treated patients.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. The study was supported by the Victorian Cancer Agency and by a National Cancer Institute Intramural Research Program, Center for Cancer Research, NIH. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Prof. Roger Martin and Dr. Normand Pouliot for critical reading of this manuscript and Val Johnston for technical assistance.
Footnotes
↵* Contributed equally to this work.
Published online Feb. 26, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication July 14, 2014.
- Accepted for publication December 8, 2014.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Dosimetric Evaluation of the Effect of Receptor Heterogeneity on the Therapeutic Efficacy of Peptide Receptor Radionuclide Therapy: Correlation with DNA Damage Induction and In Vivo Survival
- Dissimilar DNA Damage to Blood Lymphocytes After 177Lu-Labeled DOTATOC or Prostate-Specific Membrane Antigen Therapy
- Peptide Receptor Radionuclide Therapy During the COVID-19 Pandemic: Are There Any Concerns?
- Imaging DNA Damage Repair In Vivo After 177Lu-DOTATATE Therapy
- Identification of brain metastasis genes and therapeutic evaluation of histone deacetylase inhibitors in a clinically relevant model of breast cancer brain metastasis
- The Relevance of Dosimetry in Precision Medicine
- Identification of brain metastasis genes and therapeutic evaluation of histone deacetylase inhibitors in a clinically relevant model of breast cancer brain metastasis
- Localized Synchrotron Irradiation of Mouse Skin Induces Persistent Systemic Genotoxic and Immune Responses
- Radiotherapy for Non-Small Cell Lung Cancer Induces DNA Damage Response in Both Irradiated and Out-of-field Normal Tissues
- Myeloid neoplasms after chemotherapy and PRRT: myth and reality
- DNA Damage in Peripheral Blood Lymphocytes of Thyroid Cancer Patients After Radioiodine Therapy
- Radiopeptides for Imaging and Therapy: A Radiant Future
- {gamma}-H2AX Foci in Peripheral Blood Lymphocytes to Quantify Radiation-Induced DNA Damage After 177Lu-DOTA-Octreotate Peptide Receptor Radionuclide Therapy