


Abstract
The Centers for Medicare and Medicaid Services recently ruled that only 3 posttherapy follow-up 18F-FDG PET/CT scans are funded for a tumor type per patient and any additional follow-up PET/CT scans will be funded at the discretion of the local Medicare administrator. The purpose of this study was to evaluate the added value of 4 or more follow-up PET/CT scans to clinical assessment and impact on patient management. Methods: This was an institutional review board–approved, retrospective study. A total of 1,171 patients with biopsy-proven lung cancer who had undergone 18F-FDG PET/CT at a single tertiary center from 2001 to 2013 were identified. Among these, 85 patients (7.3%) had undergone 4 or more follow-up PET/CT scans, for a total of 285 fourth and subsequent follow-up PET/CT scans. Median follow-up from the fourth follow-up PET/CT scan was 31.4 mo (range, 0–155.2 mo). The follow-up PET/CT scan results were correlated with clinical assessment and treatment changes. Results: Of the 285 fourth and subsequent follow-up PET/CT scans, 149 (52.28%) were interpreted as positive and 136 (47.7%) as negative for recurrence or metastasis. A total of 47 patients (55.3%) died during the study period. PET/CT identified recurrence or metastasis in 44.3% of scans performed without prior clinical suspicion and ruled out recurrence or metastasis in 24.2% of scans performed with prior clinical suspicion. The PET/CT scan resulted in a treatment change in 28.1% (80/285) of the patients. New treatment was initiated for 20.4% (58/285) of the scans, treatment was changed in 5.6% (16/285), and ongoing treatment was stopped in 2.1% (6/285). Conclusion: The fourth and subsequent 18F-FDG PET/CT scans performed during follow-up after completion of primary treatment added value to clinical assessment and changed management 28.1% of the time.
In the era of modern oncology, lung cancer has been challenging to manage, accounting for 27% of all cancer-related deaths. Lung cancer is also the leading cause of cancer-related mortality in men and women. The American Cancer Society’s estimates for lung cancer in the United States for 2014 are about 224,210 new cases and 159,260 deaths (1). The 5-y relative survival rate for lung cancer varies markedly depending on the stage at diagnosis: 49%, 16%, and 2% for patients with local, regional, and distant disease, respectively (2). A study by Gupta et al. (3) has shown that lung cancer patients with resectable disease, medically inoperable disease, and unresectable advanced disease had, respectively, a 7%, 100%, and 53% incidence of adverse events.
The National Comprehensive Cancer Network recommends chest CT with or without a contrast agent every 6–12 mo for 2 y, followed by annual unenhanced chest CT for surveillance of lung cancer (4). 18F-FDG PET/CT is a valuable investigation for many oncology patients for staging, therapy assessment, management, and prognosis (5–9). Toba et al. (10) evaluated the role of 18F-FDG PET/CT in postoperative follow-up of asymptomatic non–small cell lung cancer patients and showed that the PET/CT studies correctly identified disease in 94% of the patients with disease recurrence, yielding high diagnostic accuracy. Similar results were obtained by other studies (11,12). Although there have been many studies demonstrating the impact of 18F-FDG PET/CT on the management plan at staging (13) and in patients with suspected disease recurrence (14,15), there is no substantial literature evaluating this clinical question in follow-up PET/CT studies. Our previous study evaluating the value of 18F-FDG PET/CT performed 6 mo after completion of treatment demonstrated that these scans are valuable in predicting survival outcomes and add value to clinical judgment, regardless of the timing of the follow-up scan (16).
Recently, the Centers for Medicare and Medicaid Services has determined that “three FDG PET scans are covered under § 1862(a)(1)(A) when used to guide subsequent management of anti-tumor treatment strategy after completion of initial anticancer therapy. Coverage of any additional FDG PET scans (that is, beyond three) used to guide subsequent management of anti-tumor treatment strategy after completion of initial anti-tumor therapy will be determined by local Medicare Administrative Contractors” (17). The objective of this study was to establish the value of fourth and subsequent posttherapy follow-up 18F-FDG PET/CT scans in the management of patients with lung cancer.
MATERIALS AND METHODS
Eligible Patients and Follow-up
This was a retrospective study performed under a waiver of informed consent as approved by the Institutional Review Board. The guidelines of the Health Insurance Portability and Accountability Act were followed. All patients treated for biopsy-proven lung cancer with more than 3 follow-up 18F-FDG PET/CT scans obtained after completion of primary treatment were included in the study. All 18F-FDG PET/CT scans after the third follow-up scan were included in the study. Patients with 2 concurrent primary cancers or with a second primary cancer were excluded from the study. Between January 2001 and October 2013, a total of 1,171 lung cancer patients who had been evaluated with 18F-FDG PET/CT were identified from our PET center database, of whom 85 patients met our study inclusion criteria, providing a total of 285 follow-up PET/CT scans (range, 4–28 per patient). Only the fourth follow-up PET/CT scan and the scans performed after the fourth scan were included in the study. These scans were performed as part of routine clinical follow-up or at the time that recurrence or metastasis was clinically suspected. All patients were followed till death or their last day of clinical follow-up at our center. The median follow-up time among these patients was 31.4 mo (range, 0–155.2 mo) from the fourth follow-up PET/CT scan.
Image Analysis
Board-certified nuclear medicine physicians interpreted the 18F-FDG PET/CT images at the time they were obtained per the routine imaging review protocol in the hospital. The scan reports were retrospectively interpreted and categorized as positive, indeterminate, or negative by a nuclear medicine postdoctoral fellow and a radiology resident. Positive reports clearly identified disease recurrence or metastases related to the primary lung cancer. Indeterminate reports did not clearly identify or deny disease, and the report impression included terminology such as “indeterminate” or “cannot exclude recurrence.” Negative scan reports clearly excluded the possibility of disease. The scan results were dichotomized into positive for disease (positive interpretations) or negative for disease (negative and indeterminate interpretations). From our previous work in other cancers such as head and neck cancer, it was anticipated that most of the indeterminate scan results are true-negative for tumor and about 5% of the indeterminate scan results eventually become false-negative when these scans are classified as negative (18). Follow-up scans were further grouped as having been performed for routine surveillance or secondary to clinical suspicion of disease recurrence or metastases. This was established from the last clinical note of the treating physician requesting the study and from the indication of the study as stated in the scan request. An 18F-FDG PET/CT scan was established as having been obtained for routine surveillance if no concerns about lung cancer recurrence or metastasis were suspected.
Change in Management Measures
Treatment details immediately before and after each scan were collected from electronic medical records to establish the change in management. The impact of each 18F-FDG PET/CT follow-up scan result on the treatment strategy for each patient was assessed and categorized. First, the status of the patients before the PET/CT study was categorized as being followed up with treatment or without treatment. Then, patients who were being followed up without treatment were categorized as receiving initiation of new treatment after the PET/CT study or continuing on follow-up without treatment. Patients who were being followed up with treatment were categorized as continuing on the same treatment after the PET/CT study, changing to new treatment, or discontinuing treatment. The final category included patients for whom not enough information was available for a judgment on any treatment change before and after the PET/CT scan. Thus, there were 6 categories in total.
Statistical Analysis
We present central tendencies as mean ± SD or as median followed by range in parentheses when data were skewed, or as frequency and percentage for categoric variables. Between groups, analyses were performed using independent-samples t testing, but when data were skewed, the Mann–Whitney U test was used. Our analysis was undertaken to determine whether there was an association between follow-up PET/CT scan result and management change. Statistical significance was set at a 2-tailed P value of 0.05 for all tests. For impact on change in management, all scans were included, as the change in management was established after each scan. All statistical analysis was performed using the JMP (version 11.0; SAS Institute Inc.) statistical package.
RESULTS
Patient Characteristics
We identified 1,171 patients diagnosed with lung cancer who had undergone an 18F-FDG PET/CT study. Of these patients, 85 (7.3%) had 4 or more follow-up scans. Patient demographics, histology, pretreatment stage, therapy details, and PET/CT results are summarized in Table 1. In total, 285 scans were obtained from the 85 lung cancer patients. The number of follow-up scans per patient ranged from 4 to 28. Sixty one patients (71.8%) had 4–6 follow-up scans, 17 (20.0%) had 7–10 follow-up scans, and 9 (10.6%) had more than 10 follow-up scans. There were a total of 112 scans that were then performed as the seventh follow-up scan or later. Of these, 54 (48.2%) were performed for routine follow-up; 24 (21.4%) for posttreatment assessment of either chemotherapy, radiation therapy, surgical resection, or radiofrequency ablation instituted for disease recurrence; 7 (6.3%) as part of mid-chemotherapy response assessment; 14 (12.5%) as follow-up of previously PET-positive findings; 9 (8.0%) as follow-up of previously PET-indeterminate findings; 2 (1.8%) for evaluation of a paraneoplastic syndrome; and 2 (1.8%) for evaluation of clinically identified disease recurrence.
Characteristics of the 85 Patients
Categorization of PET/CT Result
For clinical utility purposes, the negative and indeterminate reports were grouped as “negative for tumor recurrence or metastases” and positive reports were grouped as “positive for tumor recurrence or metastases.” PET/CT scans were negative for recurrence or metastasis 47.7% (136/285) of the time. Of the negative scans, 31.6% (43/136) were obtained within 24 mo after completion of primary treatment and 68.4% (93/136) were obtained more than 24 mo after completion of primary treatment. Of the positive scans, 30.9% (46/149) were obtained within 24 mo after completion of primary treatment and 69.1% (103/149) were obtained more than 24 mo after completion of primary treatment (Fig. 1). Among the 149 positive scans, 71 (47.7%) were positive for locoregional disease, 36 (24.2%) were positive for distant disease, and 42 (28.2%) were positive for both locoregional and distant disease.
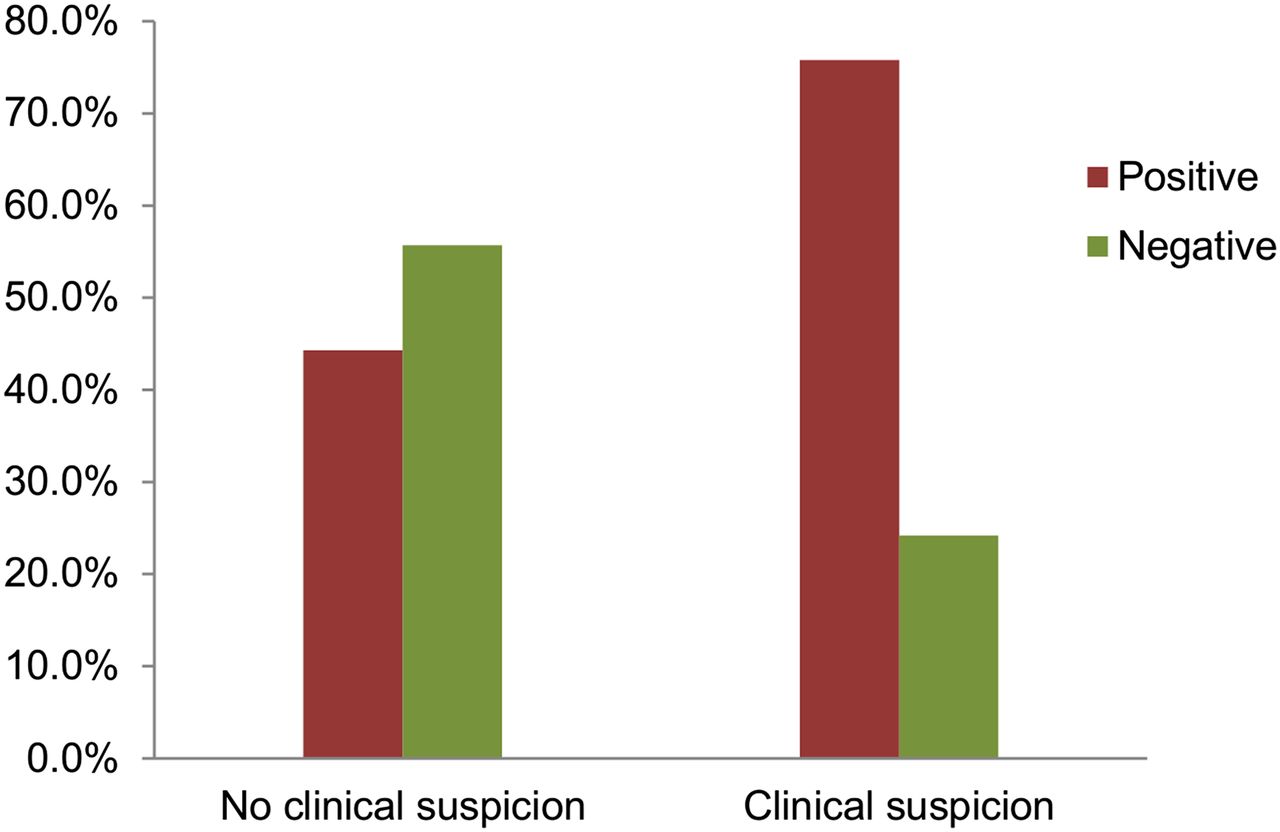
Added value of PET/CT in clinical assessment. PET/CT was helpful in excluding tumor in 24.2% (16/66) of PET/CT scans performed with clinical suspicion of recurrence or metastasis and in identifying recurrence or metastasis in 44.3% (97/219) of PET/CT scan performed with no prior clinical suspicion.
Impact on Clinical Assessment
We evaluated the impact of 18F-FDG PET/CT on clinical assessment in follow-up at the time of the PET/CT scan. Of the 285 scans, 219 (76.8%) were obtained for routine follow-up without clinical suspicion of recurrent disease or metastasis and 66 (23.2%) were obtained to evaluate for suspected disease. In the context of clinical assessment, PET/CT identified recurrence or metastasis in 44.3% (97/219) of scans performed without prior clinical suspicion and ruled out recurrence or metastasis in 24.2% (16/66) of scans performed with prior clinical suspicion (Fig. 1; Table 2). Of the 219 scans that were done without prior clinical suspicion of disease, 117 (53.2%) had a previous positive scan after treatment completion and 102 (46.8%) had either a negative scan or treatment-related changes before the scan during the posttreatment period. Of the 66 scans that were performed with prior clinical suspicion of disease, 20 (30.8%) were performed while patients either were on treatment or had recently completed treatment and for therapy assessment in addition to restaging; for the other 46 scans (69.2%), the patients were not on any treatment (Figs. 2–4).
Numbers of PET/CT Scans with Positive and Negative Results

Axial fused PET/CT images of 39-y-old man with stage III adenocarcinoma of right upper lobe of lung, treated primarily with lobectomy and adjuvant chemoradiation. Recent chest imaging performed almost 10 y after completion of primary treatment for evaluation of pneumonia showed nodular thickening in left upper lobe, and a fifth follow-up 18F-FDG PET/CT study was requested because of clinical suspicion of lung cancer recurrence. PET/CT study demonstrates intensely 18F-FDG–avid nodular soft tissue in left upper lobe (arrow) with metabolically active mediastinal lymph nodes (arrow). Histopathologic examination of mass revealed adenocarcinoma. This finding could be suggestive of either disease recurrence or metachronous primary disease. After the study, patient underwent left upper lobectomy.
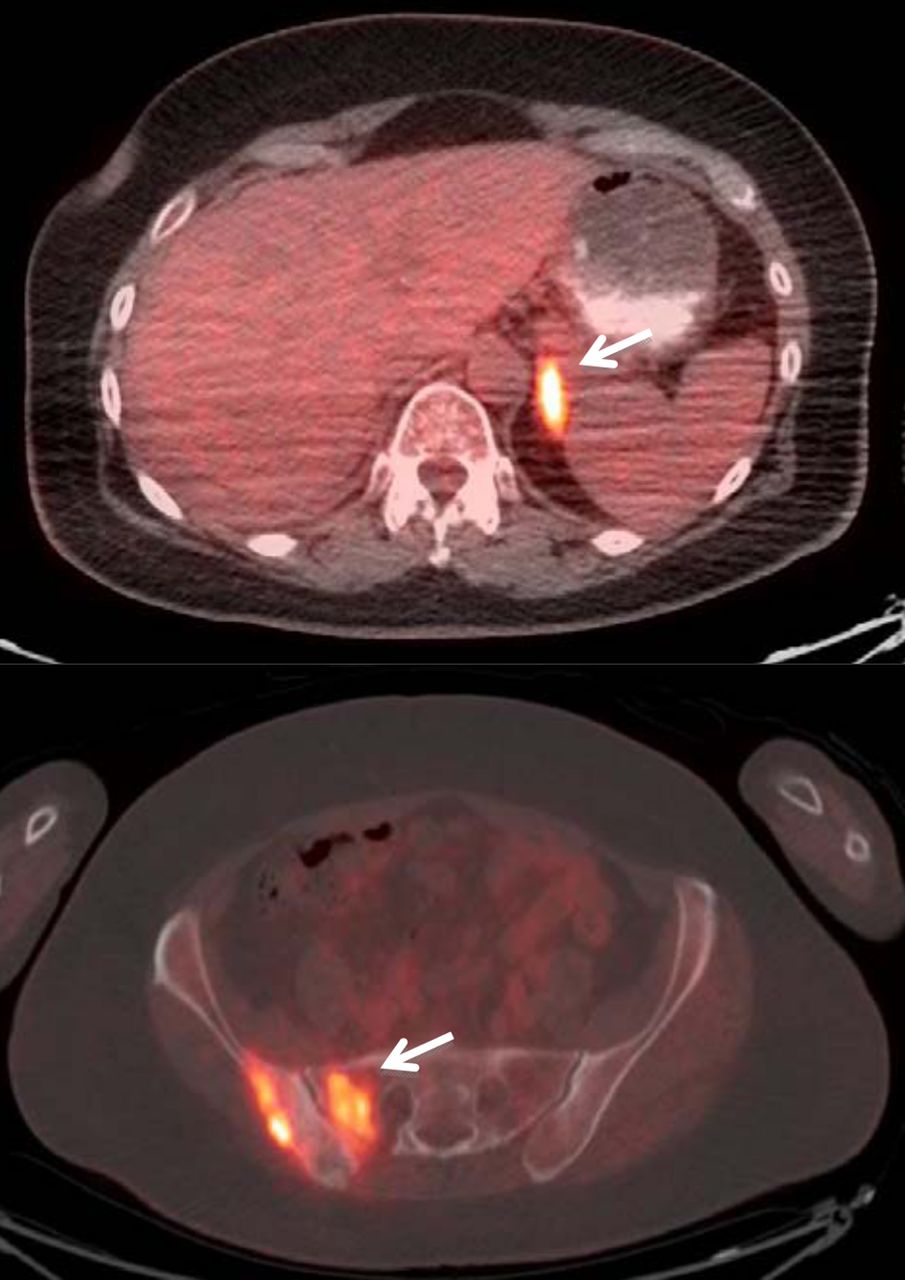
Axial fused PET/CT images of 60-y-old woman with stage 2b (T3N0M0) adenocarcinoma of right upper lobe of lung, treated primarily with lobectomy, lymph node dissection, and chemotherapy. A routine fifth follow-up scan was requested without prior clinical suspicion of lung cancer recurrence, 1 y after completion of primary treatment. PET/CT study demonstrates hypermetabolic, metastatic multiple osseous (arrow) and left adrenal lesions (arrow). Patient was started on new chemotherapy regimen after study.

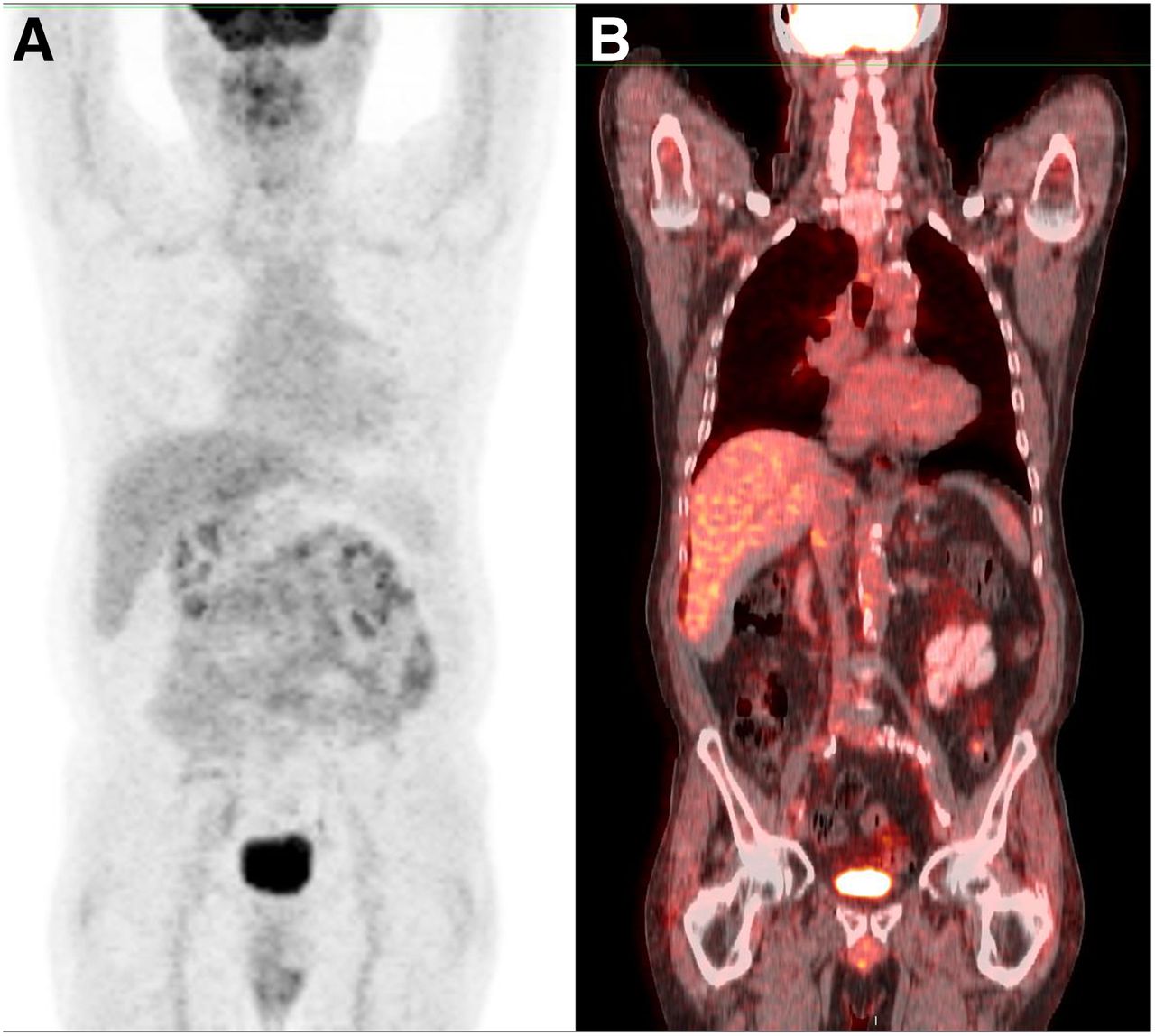
Anterior maximum-intensity projection (A) and coronal (B) fused PET/CT images of 70-y-old man with stage II adenocarcinoma of left lung, treated primarily with lobectomy and adjuvant chemotherapy. Recent CT scan had revealed suggestive nodular thickening of left adrenal gland. An eighth follow-up scan was requested to evaluate this finding, 3 y after completion of primary treatment. PET/CT study was negative for active disease, consistent with complete remission.
Impact on Change in Management Strategy
The impact of each of the follow-up PET/CT studies on the treatment planning was also evaluated by careful review of the electronic medical records before and after the studies. Of the 285 scans, 157 (55.1%) were performed on patients who were not on treatment before the scan. Of those 157 scans, 99 (63.1%) led to no change in treatment and the patients continued to be followed up, whereas 58 (36.9%) led to initiation of new treatment. Of the 75 scans that were performed on patients who were on treatment before the scan, 53 (70.7%) led to no change in treatment and the treatment plan was continued as before (PET/CT showed a good response to the treatment, and the treatment regime was not altered), 16 (21.3%) led to a change in treatment, and treatment was stopped after 6 (8.0%). In 53 scans (18.6%), the treatment impact of the scan was not known. The treatment impact of the follow-up PET/CT studies is summarized in Table 3.
Follow-up 18F-FDG PET/CT and Impact on Treatment
DISCUSSION
The objective of the study was to evaluate the value of the fourth and subsequent 18F-FDG PET/CT studies in the follow-up or surveillance of patients with lung cancer, performed after completion of primary treatment with or without clinical suspicion of recurrence of metastases. Our study showed that the results of the follow-up PET/CT studies can affect the treatment plan, resulting in a change in treatment strategy in up to one third (30.21%) of the patients. Hicks et al. (15) evaluated the impact of follow-up PET scans in patients with lung cancer and found that the PET findings induced a major management change in 40 of the 63 patients (63%). Unlike our study, this study included all follow-up scans obtained 6 mo after definitive treatment. Similarly, in a study by Jimenez-Bonilla et al., the PET findings resulted in a treatment change in 30.91% (17/55) of lung cancer patients (19). All follow-up PET studies performed on lung cancer patients with suspected recurrence were included in this study as well.
We have also observed from our study that the fourth and subsequent follow-up 18F-FDG PET/CT scans can add value to clinical assessment. PET/CT identified recurrence in 44.3% of scans performed without prior clinical suspicion of recurrence and ruled out recurrence in 24.2% of scans performed with prior clinical suspicion. The majority (77%) of the fourth and subsequent follow-up scans were performed without prior clinical suspicion as routine follow-up scans (a behavior pattern). In both groups, the fourth and subsequent follow-up PET/CT scans added value to the clinical assessment. This added value of PET/CT in the context of clinical assessment has been established by Hicks et al. (15), who showed good diagnostic accuracy of 18F-FDG PET in identifying disease on scans performed with prior clinical suspicion of active disease. Similar performance was noted by Keidar et al., who evaluated the diagnostic value of 18F-FDG PET/CT in suspected lung cancer recurrence (14). Both the above-mentioned studies have been executed only on lung cancer patients with suspected recurrence or relapse, and these studies include all follow-up scans performed on these patients, irrespective of the number of scans. In addition to the value of follow-up PET/CT in patients with clinical suspicion of disease, our study shows that PET/CT adds value to the clinical assessment when performed in the absence of prior clinical suspicion. However, we did not investigate the frequency of the follow-up scan (time interval in follow-up) in the context of no prior suspicion of disease. Though a behavior pattern of routinely requesting follow-up scans is strongly discouraged, the time interval of such scans for adding value to clinical assessment needs to established.
We acknowledge multiple limitations to our study. The study was retrospective and may have the inherent errors of confounding when the exposure is not controlled. Indeterminate scan results were included in the study and the exact cause of such a result was not evaluated. The treatment plan was not clearly mentioned for 18.6% of the patients. The clinical indication of the study was retrospectively examined from electronic medical records and the PET/CT requisitions. The exact perspective of the clinician ordering the study was not known, and we may have underestimated the clinical suspicion before the scans.
CONCLUSION
Our study showed that the fourth and subsequent follow-up 18F-FDG PET/CT study adds value to clinical assessment and the treatment planning strategy. Though a behavior pattern of requesting routine follow-up scans is strongly discouraged, this study supports the suggestion that the number of follow-up scans performed for each patient should be planned on the basis of the individual-patient clinical context and cannot be generalized for the whole subset of lung cancer patients.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 22, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication August 27, 2014.
- Accepted for publication December 26, 2014.





{kind=link}
{kind=link}
{kind=link}
{kind=link}