


Abstract
The purpose of this study was to evaluate the added value of a fourth and subsequent follow-up PET/CT scans to clinical assessment and impact on patient management in patients with colorectal cancer. Methods: This was an institutional review board–approved, retrospective study. Eight hundred twenty-two patients with biopsy-proven colorectal cancer, who underwent 18F-FDG PET/CT, were identified from 2000 to 2012. Among these, 73 (8.9%) patients underwent 4 or more follow-up PET/CT scans, with a total of 313 fourth and subsequent follow-up PET/CT scans. Median follow-up from the fourth follow-up PET/CT scan was 41.7 mo. The added value of each follow-up PET/CT scan, for clinical assessment and the treatment changes subsequent to each follow-up PET/CT scan, was established. Overall survival prediction was established using Kaplan–Meier plots with a Mantel–Cox log-rank test. Results: Of the 313 fourth and subsequent follow-up PET/CT scans, 174 (55.6%) were interpreted as positive and 139 (44.4%) were interpreted as negative for recurrence or metastases. Thirty-four (46.6%) patients died during the study period. PET/CT identified recurrence or metastasis in 40.0% of scans obtained without prior clinical suspicion and ruled out disease in 23.6% of scans obtained with prior clinical suspicion. The PET/CT scan resulted in treatment change after 34.2% (107/313) of the scans. New treatment was initiated after 24.0% (75/313) of the scans, and treatment was changed after 8.0% (25/313) scans. There was a statistically significant difference in the overall survival between patients with a positive and all negative fourth and subsequent follow-up PET/CT scans at the patient level (log-rank, P = 0.001). Conclusion: The fourth and subsequent 18F-FDG PET/CT scans obtained after primary treatment completion add value to clinical assessment and the management plan and provide prognostic information in patients with colorectal cancer.
Colorectal cancer is the third most common cancer in both men and women, accounting for 8% of all the cancers diagnosed. It is also the second leading cause of cancer death in men and women combined. The American Cancer Society has estimated that there will be 93,090 new cases of colon cancer and 39,610 new cases of rectal cancer diagnosed in the year 2015 in the United States. When the disease is localized, the 5-y survival is 90%, which decreases to 71% when there is locoregional spread of disease and decreases further to 13% in patients with distant disease (1).
The National Comprehensive Cancer Network guidelines for colorectal cancer (version 1.2014) recommends chest/abdomen/pelvic CT annually for patients at high risk of recurrence with colorectal tumors for up to 5 y as part of surveillance. PET/CT has not been recommended for routine surveillance (2). In recent years, 18F-FDG PET/CT has gained special importance in the evaluation of many human solid tumors. In the follow-up of colorectal cancers, 18F-FDG PET/CT has been shown to have good diagnostic accuracy, has an impact in patient management, and predicts prognosis (3–8). Although 18F-FDG PET/CT has not been recommended in the routine follow-up of colorectal cancer, studies have shown that PET/CT is superior to conventional imaging methods in the follow-up (9–11).
Recently the Center for Medicare and Medicaid Services declared that three 18F-FDG PET scans are covered under § 1862(a) (1) (A) when used to guide subsequent management of antitumor treatment strategy after completion of initial anticancer therapy. Coverage of any additional 18F-FDG PET/CT scans will be determined by local Medicare administrative contractors (12). Our previous studies have demonstrated that the follow-up 18F-FDG PET/CT studies performed 6 mo or more after treatment completion add value to clinical judgment and are a prognostic marker for overall survival (OS) and that the fourth and subsequent follow-up 18F-FDG PET/CT scans obtained after treatment completion added value to the clinical assessment and management plan in patients with lung cancer (13,14). The objective of this study was to evaluate the value of the fourth and subsequent posttherapy follow-up 18F-FDG PET/CT scans in the clinical assessment and management of patients with colorectal cancers.
MATERIALS AND METHODS
Eligible Patients and Follow-up
This was a retrospective study performed under a waiver of informed consent as approved by the Institutional Review Board. The guidelines of the Health Insurance and Portability and Accountability Act were followed. Patients with biopsy-proven colorectal cancers with more than 3 follow-up 18F-FDG PET/CT studies after completion of primary treatment between January 2000 and June 2012 were included in the study. All 18F-FDG PET/CT studies performed after the third follow-up scan were included in the study. Patients with concurrent primary tumors or a second primary cancer were excluded from the study. Eight hundred twenty-two colorectal cancer patients who had undergone 18F-FDG PET/CT as part of the evaluation of the cancer were identified from our PET/CT database. Of these, 73 patients met our inclusion criteria, providing 313 fourth and subsequent follow-up PET/CT scans (range, 4–24 follow-up scans per patient). Only the fourth follow-up PET/CT scan and the scans obtained after the fourth scan were included in the study. The scans were either acquired at the time of clinical suspicion of disease recurrence or metastasis or as part of routine follow-up. All patients included in the study were followed until death. Patients who are alive were censored to the last date of follow-up at our institution. The median follow-up period of patients included in the study from the fourth follow-up PET/CT study was 41.7 mo (range, 0–125 mo).
Image Analysis
Board-certified nuclear medicine physicians interpreted the 18F-FDG PET/CT images at the time of the imaging as per the routine imaging review protocol in the hospital. The scan reports were retrospectively read and categorized as positive, indeterminate, or negative by a nuclear medicine postdoctoral fellow, a radiology resident, and surgical intern. Positive reports clearly identified disease recurrence or metastases related to the primary colorectal cancer. Indeterminate reports did not clearly identify or deny disease, and their scan report impression included terminology such as indeterminate or cannot exclude recurrence. Negative scan reports clearly excluded the possibility of disease. For clinical utility and analysis purposes, the indeterminate scans were categorized as negative for disease recurrence or metastasis. Follow-up scans were further grouped as having been obtained for routine follow-up without prior clinical suspicion of disease or secondary to clinical suspicion of disease recurrence or metastases. This categorization of scans based on clinical suspicion was established from the last clinical note of the treating physician requesting the study and from the indication of the study as stated in the scan request.
Change in Management Measures
Treatment details immediately before and after each scan were collected from electronic medical records to establish the change in management. The impact of each of the 18F-FDG PET/CT follow-up scan results on the treatment strategy for each individual patient was assessed. The treatment impact was assessed and categorized into 6 groups. The first step dichotomized the treatment stage of the patient before the PET/CT study as patients who were on treatment and patients who were followed up without treatment. The second step categorized patients, who were currently on follow-up with no active ongoing treatment, into whether there was initiation of new treatment or continued follow-up without treatment, after the PET/CT study. The second step also categorized patients on treatment into whether there was continuation of the same treatment, change to new treatment, or cessation of ongoing treatment, after the PET/CT study. The final category included patients in whom the treatment details were not clearly known to make a judgment on the treatment change before and after the PET/CT scan.
Outcome Measures
OS was defined as the time (mo) interval between the date of the fourth or subsequent follow-up PET/CT scan and the date of death. The date of the scan was recorded from the electronic medical record of each patient, and the date of death was extracted from a review of medical records and a public registry of death (15). The survival data for patients who were alive were censored at the last follow-up date at our institution.
Statistical Analysis
Descriptive features of variables were presented using mean ± SD, or median, if data were not in normal distribution. This study focused on the evaluation of the relationship between the fourth and subsequent follow-up 18F-FDG PET/CT scans and OS as well as on the impact of these scans on treatment of patients with colorectal cancer. The impact of scan results (positive or negative) on treatment of colorectal cancer (6 classified categories) was evaluated using χ2 analysis. Kaplan–Meier survival curves at the patient level were plotted with patients with at least 1 positive fourth and subsequent follow-up scan versus patients with all negative fourth and subsequent follow-up scans. Statistical significance was set at a 2-tailed P value of less than 0.05 for all tests. All statistical analyses were performed using the SPSS (version 15.0; SPSS Inc.) statistical software.
RESULTS
Patient Characteristics
We identified 822 patients diagnosed with colorectal cancer who had undergone at least one 18F-FDG PET/CT for the evaluation of the cancer. Of these, 73 (8.9%) patients had 4 or more follow-up PET/CT scans. Patient demographics, tumor histology, tumor location, tumor stage, treatment details, and the PET/CT results have been summarized in Table 1. Three hundred thirteen fourth and subsequent follow-up scans were obtained for these 73 patients with colorectal cancer. The number of follow-up scans per patient ranged from 4 to 24 scans. Forty-one (56.2%) patients underwent 4–6 follow-up scans, 20 (27.4%) patients underwent 7–10 follow-up scans, and 12 (16.4%) patients underwent 11 or more follow-up scans.
Characteristics of 73 Patients Included in Study
Categorization of PET/CT Results
For clinical utility purpose, the negative and indeterminate scan results were grouped as negative for tumor recurrence or metastases. Twenty of 313 (6.4%) scans were categorized as indeterminate for disease recurrence or metastasis and thus were grouped with negative scans. PET/CT scans were negative for recurrence or metastasis in 44.4% (139/313) scans. Of the negative scans, 36.7% (51/139) were obtained within 24 mo after completion of primary treatment, and 63.3% (88/139) scans were obtained more than 24 mo after completion of primary treatment. The median follow-up for patients with a negative PET/CT scan was 48.6 mo. Of the positive scans, 35.6% (62/174) were obtained within 24 mo of completion of primary treatment, and 64.4% (112/174) were obtained more than 24 mo after completion of treatment. Among the 174 positive scans, 8 (4.6%) scans were positive for locoregional disease and 166 (95.4%) scans were positive for distant disease or both locoregional and distant disease. Of the positive scans, 14 (8.0%) were after all negative PET/CT scans during the follow-up period. The median follow-up for patients with a positive PET/CT scan was 22.5 mo. Forty-seven (27.0%) of the positive scans were confirmed to be positive by histopathology, and 120 (69.0%) were confirmed by further imaging or by 6-mo clinical follow-up.
Impact on Clinical Assessment
The impact of 18F-FDG PET/CT on the clinical assessment in the follow-up period at the time of the PET/CT scan was evaluated. Of the 313 scans, 165 (52.7%) were obtained for routine follow-up without prior clinical suspicion of disease and 148 (47.3%) were obtained with prior suspicion of disease. In the context of clinical assessment, PET/CT identified recurrence or metastasis in 40.0% (61/165) of scans obtained without prior clinical suspicion and ruled out disease in 23.6% (35/148) of scans obtained with prior clinical suspicion of disease (Figs. 1–3; Table 2). Of the 165 scans that were acquired without prior clinical suspicion of disease, 111 (67.3%) scans were previously positive before the fourth follow-up scan after treatment completion and 54 (32.7%) scans were previously all negative before the fourth follow-up scan. Of the 165 scans that were obtained without prior clinical suspicion of disease, 43 (26.1%) were done as part of therapy assessment after treatment for disease recurrence or metastasis and 122 (73.9%) scans were obtained for routine follow-up.
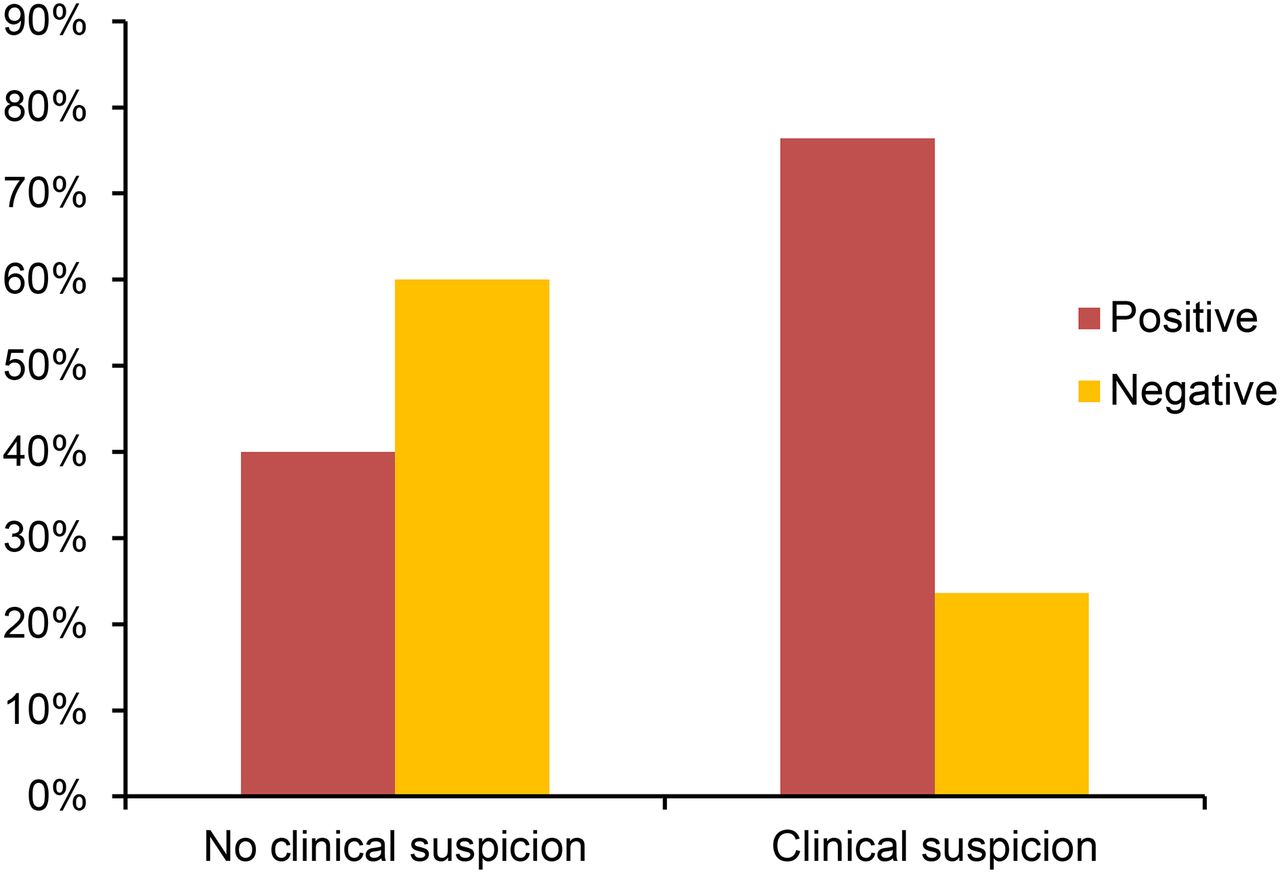
Added value of PET/CT in clinical assessment. PET/CT was helpful in excluding tumor in 23.6% (35/148) of the times PET/CT scan with clinical suspicion of recurrence or metastasis was obtained and identifying recurrence or metastasis in 40.0% (61/165) of times PET/CT scan with no prior clinical suspicion was obtained.
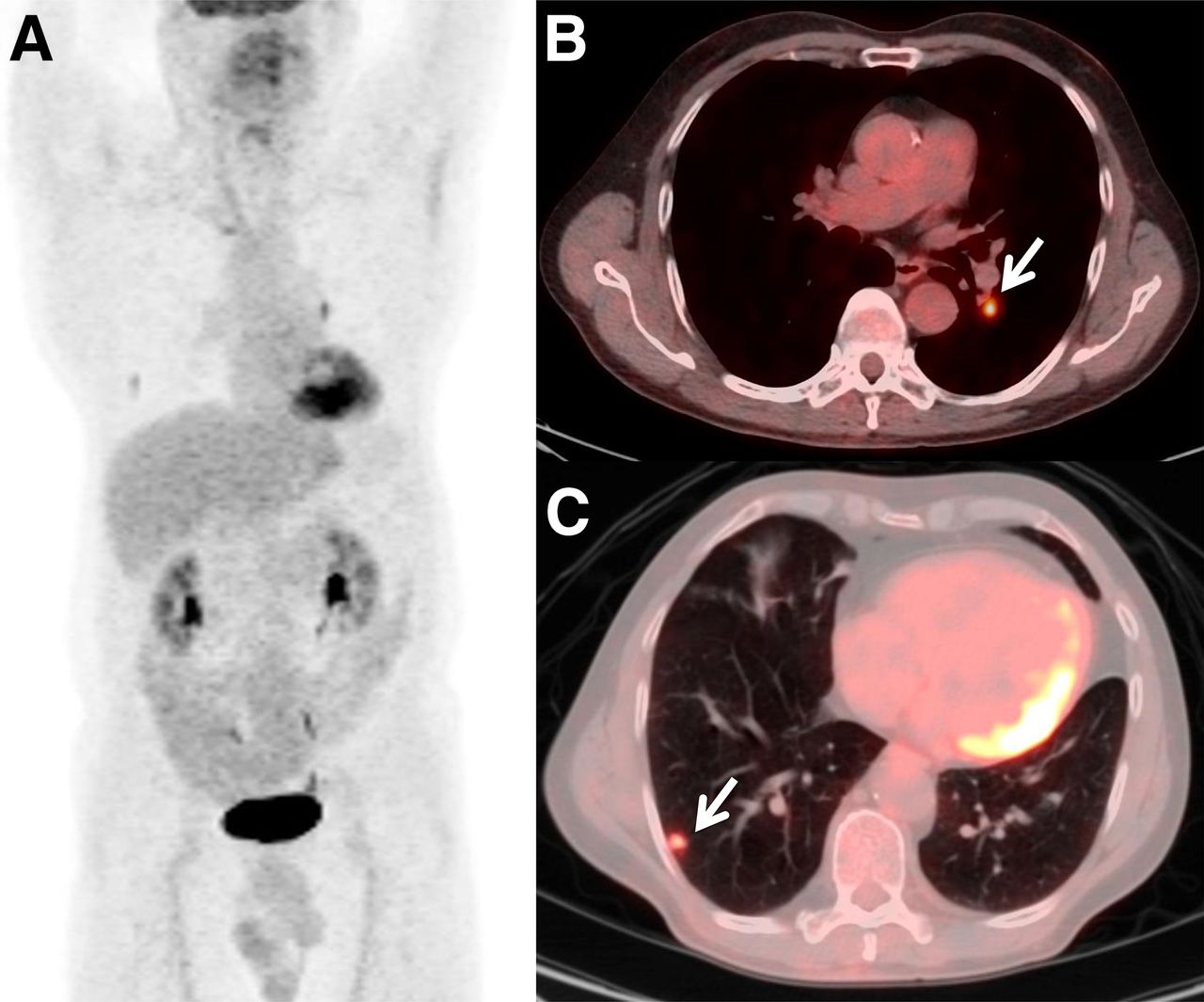
Positive follow-up scan obtained for routine follow-up. Anterior maximum-intensity-projection (A) and axial fused PET/CT (B and C) images of a 59-y-old man with history of rectal adenocarcinoma metastatic to liver, status after low anterior resection and adjuvant chemotherapy, who underwent a fourth follow-up PET/CT study for routine follow-up. PET/CT study demonstrated metabolically active (maximum standardized uptake value, 4.11) left hilar node (B; arrow) and hypermetabolic (maximum standardized uptake value, 2.4) right pulmonary nodule (C; arrow), consistent with metastatic disease. After study, he underwent chemotherapy with 3 cycles of 5-fluorouracil, oxaliplatin, folinic acid and bevacizumab.
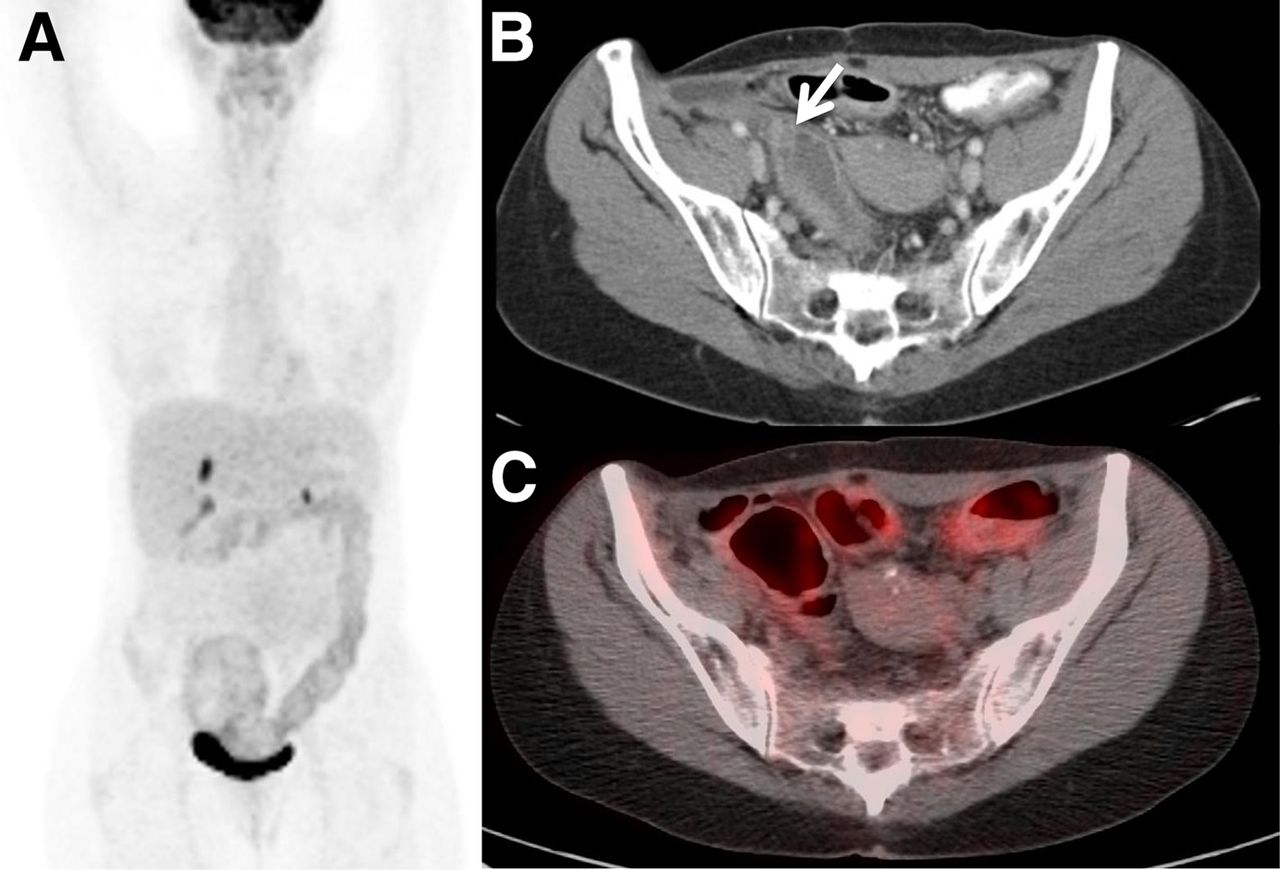
Negative follow-up scan obtained with clinical suspicion. Anterior maximum-intensity-projection (A), axial contrast-enhanced CT (B), and axial fused PET/CT (C) images of a 52-y-old woman with history of adenocarcinoma of colon, status after right hemicolectomy and chemotherapy, who was on follow-up. She was treated for local recurrence 2 y after diagnosis. Follow-up CT (B) performed 4 y after diagnosis revealed hypodense area in right lower quadrant, suggestive of local recurrence in rectosigmoid colon (arrow). Fourth follow-up PET/CT was ordered for further evaluation, which demonstrated no specific increase in metabolic activity to suggest disease recurrence, and patient has been on regular follow-up since.
Clinical Suspicion PET/CT Results
Tumor Characteristics and PET/CT Results
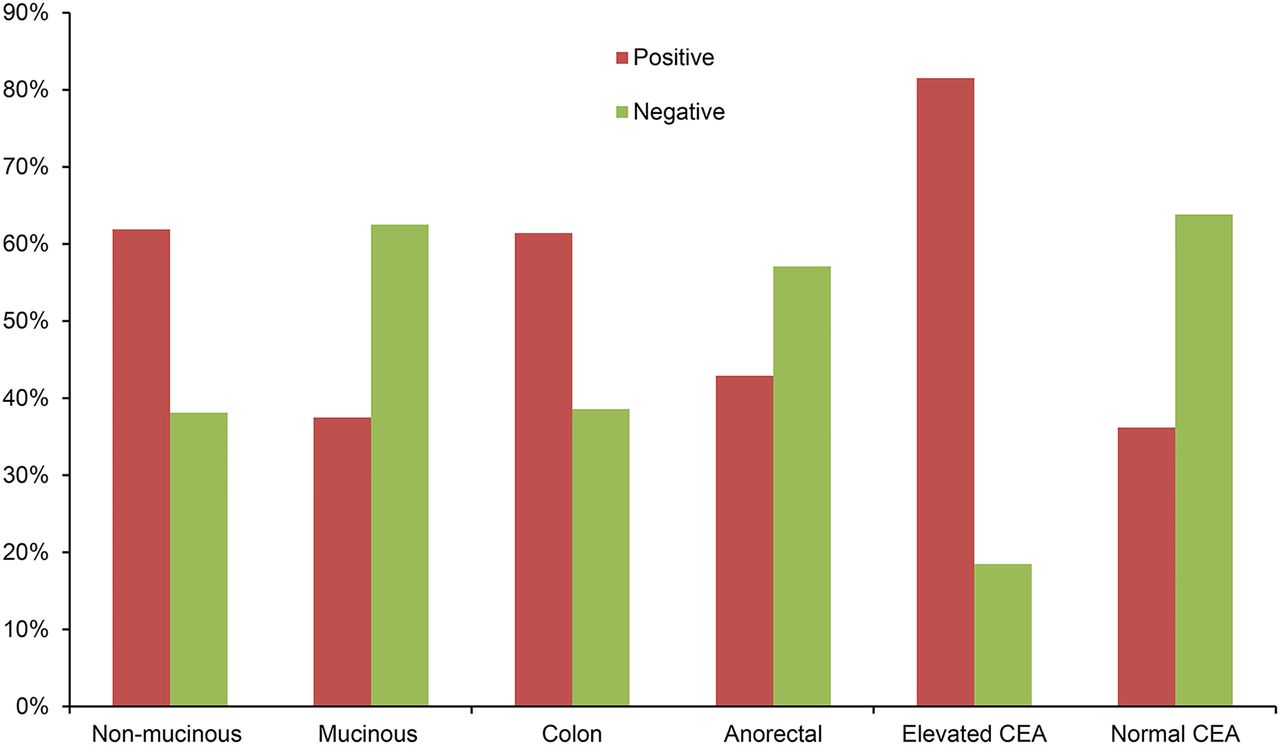
Of the 313 scans, 255 (81.5%) were obtained for patients with colorectal adenocarcinomas. Of these 255 scans, 247 (96.9%) were acquired from patients with nonmucinous adenocarcinoma and 8 (3.1%) from patients with mucinous adenocarcinoma by histopathology. Among patients with nonmucinous adenocarcinoma, 153 (61.9%) follow-up PET/CT scans were categorized as positive and 94 (38.1%) scans were categorized as negative. Among patients with mucinous adenocarcinoma, 3 (37.5%) scans were categorized as positive and 5 (62.5%) scans were categorized as negative.
On the basis of tumor location, 215 (68.7%) scans were obtained for patients with a colon primary malignancy and 98 (31.3%) scans were obtained for patients with a primary anorectal malignancy. Among patients with a colon primary, 132 (61.4%) scans were categorized as positive and 83 (38.6%) scans were categorized as negative. Among patients with an anorectal malignancy, 42 (42.9%) scans were categorized as positive and 56 (57.1%) scans were categorized as negative.
Of the 313 follow-up scans, carcinoembryonic antigen (CEA) levels were available before the scan for 139 (44.4%) scans. Of these, 92 (66.2%) had elevated CEA levels and 47 (33.8%) had normal CEA levels. Of the scans with a prior elevated CEA level, 75 (81.5%) were categorized as positive and 17 (18.5%) scans were categorized as negative. Of the scans with a prior normal CEA level, 17 (36.2%) were categorized as positive and 30 (63.8%) were categorized as negative (Fig. 4).
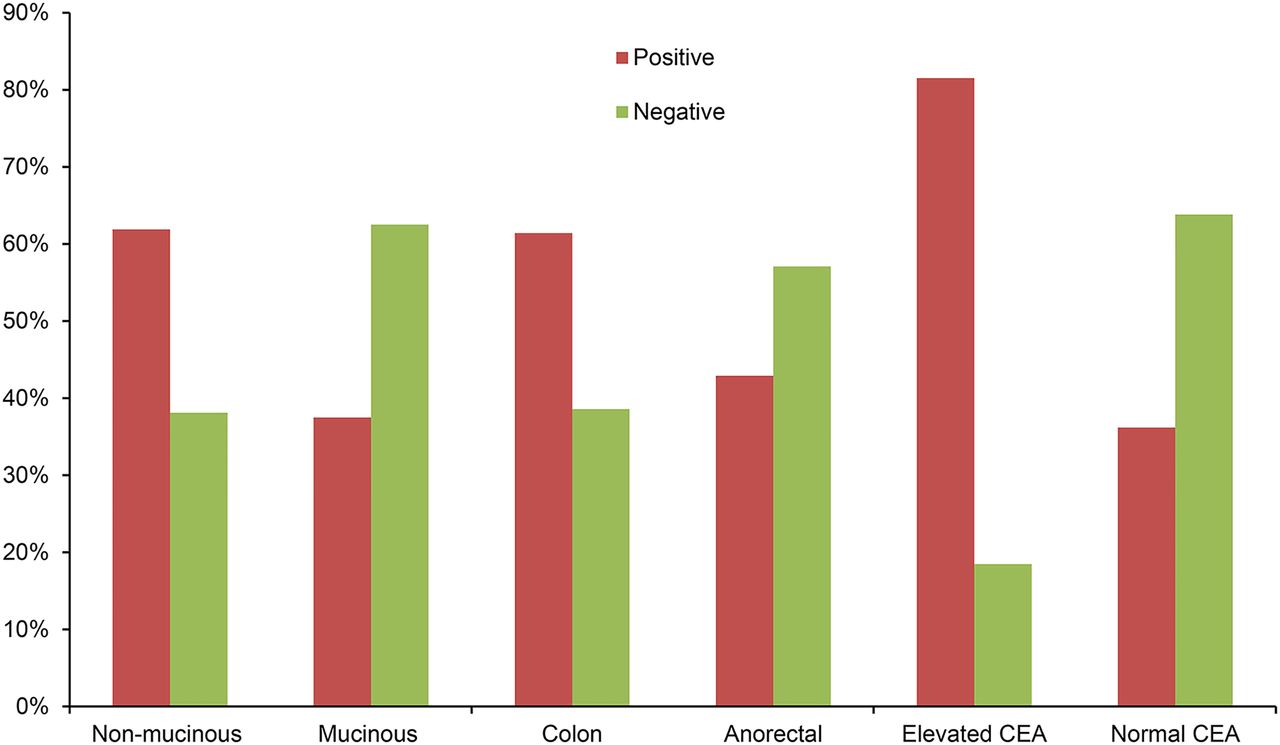
Tumor characteristics and PET/CT results. Among patients with nonmucinous adenocarcinoma, 61.9% PET/CT scans were positive and 38.1% scans were negative. Among patients with mucinous adenocarcinoma, 37.5% scans were positive and 62.5% scans were negative. Among patients with a colon primary, 61.4% scans were positive and 38.6% scans were negative. Among patients with an anorectal malignancy, 42.9% scans were positive and 57.1% scans were negative. Of scans with prior elevated CEA level, 81.5% scans were positive and 18.5% scans were negative. Of scans with prior normal CEA level, 36.2% scans were positive and 63.8% scans were negative.
Impact on Change in Management Strategy
The impact of each of the follow-up PET/CT studies on the treatment planning was also evaluated by careful review of the electronic medical records before and after the studies. Of the 313 scans, 213 (68.1%) were obtained for patients who were not on treatment before the scan. Of the 213 scans that were acquired for patients who were not on treatment before the scan, 138 (64.8%) led to no change in treatment and the patients continued to be on follow-up without treatment, and 75 (35.2%) led to initiation of new treatment. Of the 83 scans that were obtained for patients who were on treatment before the scan, 51 (61.4%) led to no change in treatment and the treatment plan was continued as before (PET/CT showed good response to the treatment and the treatment regime was not altered), and 25 (30.1%) led to change in treatment and treatment was stopped after 7 (8.4%) scans. In 17 (5.4%) scans, the treatment impact of the scan was not known. The treatment impact of the follow-up PET/CT studies has been summarized in Table 3. Tumor location (colon vs. anorectal) (P = 0.023), tumor histology (P = 0.014), tumor differentiation (P = 0.007), and PET/CT scan result (P < 0.0001) were significantly associated with management change. Sex (P = 0.162), CEA status (elevated CEA vs. normal CEA) (P = 0.079), age (P = 0.139), CEA level (P = 0.176), and time from primary treatment completion (P = 0.114) were not significantly associated with management change.
Follow-up 18F-FDG PET/CT and Impact on Treatment
PET/CT Results and Kaplan–Meier Survival Analysis
Of the 73 patients included in the study, 53 had at least 1 positive PET/CT fourth or subsequent scan for recurrence and 20 had all negative scans. Thirty-four patients died during the study period, of which 32 (94.1%) had at least 1 positive PET/CT scan and 2 (5.9%) had all negative scans. The Kaplan–Meier analyses based on the PET/CT scan results showed there was significant difference in OS between patients who had a positive PET/CT scan (median OS, 24.3 mo) and those who had all negative PET/CT scans (median OS, 37.9 mo) (log-rank, P = 0.001) at the patient level (Fig. 5).
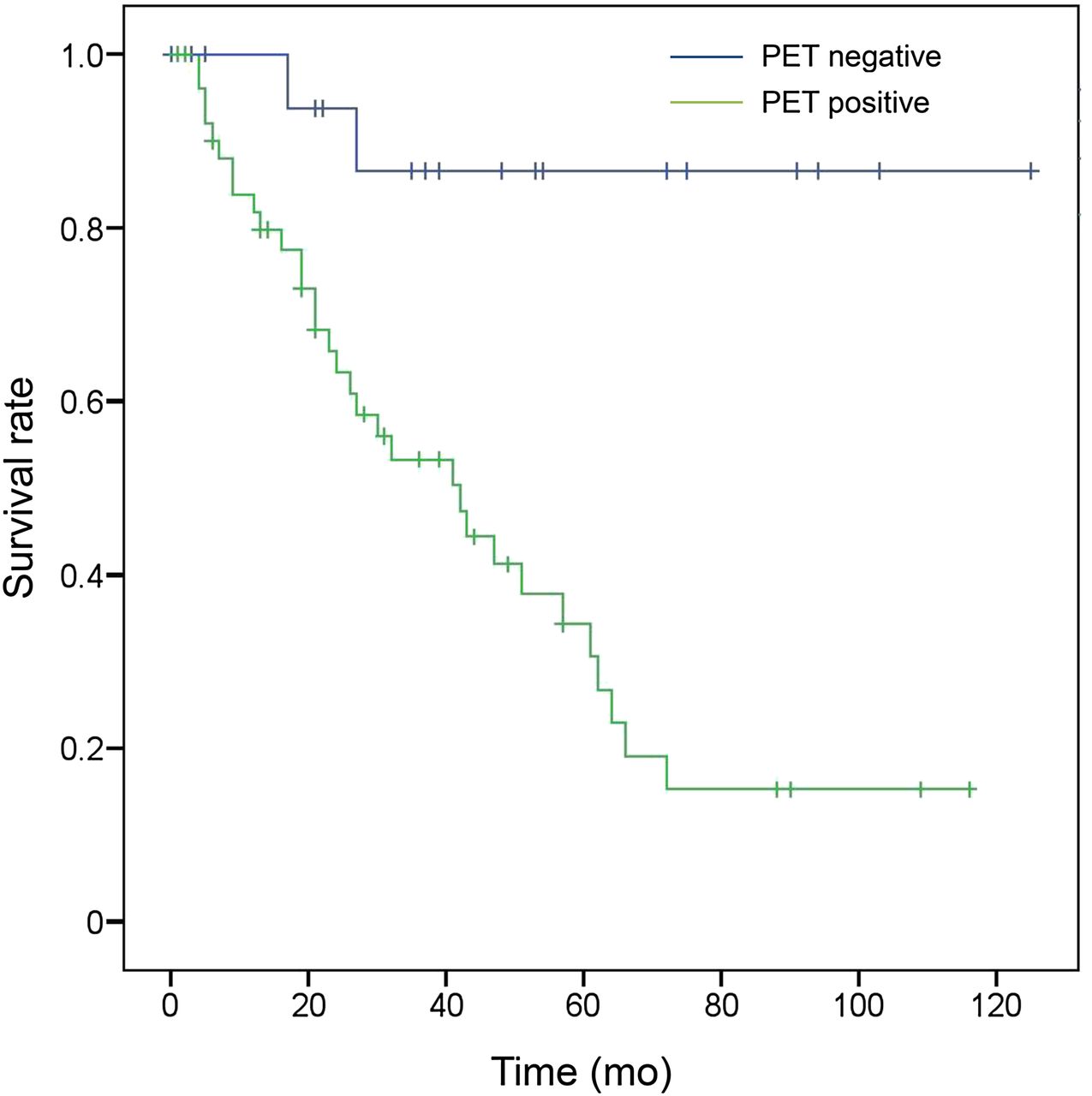
Kaplan–Meier survival plot by PET/CT result (patient level). OS (mo) between patients who had at least 1 positive (green line) and all negative (blue line) fourth and subsequent follow-up PET/CT scans for colorectal cancer differed significantly (log-rank, P = 0.001).
DISCUSSION
The objective of the study was to evaluate the value of the fourth and subsequent 18F-FDG PET/CT studies in the follow-up or surveillance of patients with colorectal cancer, performed after completion of primary treatment with or without clinical suspicion of disease recurrence or metastases. In a systematic review of studies between 1996 and 2012 by Patel et al., 2 studies evaluating the role of PET/CT in the surveillance of patients with colorectal cancer were included and the authors concluded that there was insufficient evidence for the use of PET/CT for surveillance in these patients (16). After a systematic review and meta-analysis of 11 studies, yielding a total of 510 patients, Lu et al. concluded that 18F-FDG PET and PET/CT were valuable in the assessment of colorectal cancer patients with suspected disease recurrence based on elevated CEA levels (17). Ozkan et al. also showed that PET/CT was useful in the detection of colorectal recurrence in patients with elevated CEA, irrespective of the CEA level (18). In a study of 235 colorectal cancer patients, Sanli et al. observed that 18F-FDG PET/CT can detect tumor recurrence in patients with suspected colorectal cancer recurrence, even with normal CEA levels (19). Our study demonstrated that the fourth and subsequent follow-up 18F-FDG PET/CT scans can add value to clinical assessment. The follow-up PET/CT studies identified recurrence in 40.0% scans obtained without prior clinical suspicion of disease and ruled out recurrence in 23.6% scans obtained with prior clinical suspicion. These findings provide valuable and important information to the treating physicians in making their decisions how patients are managed after the PET/CT.
In the context of adding value to clinical management, the National Oncologic PET Registry has demonstrated that physicians often change their intended management based on PET scan results in 36.5% of patients (20). However, the true percentage of change in management was not known in the National Oncologic PET Registry. Tural et al. retrospectively evaluated 122 patients with suspected recurrent colorectal cancer and determined the impact of PET/CT on the management plan of these patients. The authors demonstrated that PET/CT changed the treatment plan to curative intent in 37% patients, and there was a statistically significant (P = 0.004) difference in the median progression-free survival and OS (P = 0.045) between patients planned to receive curative treatment before and after the PET/CT study (5). In a study by Moulton et al. of 263 patients with colorectal cancer treated by surgical resection and who had resectable colorectal liver metastasis, there was change in management in 8.0% patients who underwent a PET/CT study (21). In our study, there was change in management after 34.2% of the fourth and subsequent follow-up PET/CT scans. New treatment was started after 24.0% of the scans, treatment was changed after 8.0% of the scans, and ongoing treatment was stopped after 2.2% of the scans. These findings show that the PET/CT results play an important role in the treatment plan in about one third of the patients in their longitudinal follow-up. Identification of treatable disease recurrence can also improve the survival of these patients (22).
The value of 18F-FDG PET/CT in the prediction of prognosis in patients with colorectal cancer has been demonstrated by former studies. In a recent study by Wasserberg et al. of 91 colorectal cancer patients and postsurgical resection, the authors demonstrated that the 5-y survival rate was significantly higher in patients with a negative scan than in patients with a positive scan (70% vs. 42%, P < 0.0006) (23). Our study further extends the evidence by demonstrating that fourth and subsequent follow-up PET/CT scan results can predict OS. This finding adds evidence that the follow-up PET/CT scans provide survival prediction value in the intermediate to long-term follow-up of these patients.
We acknowledge a few limitations to our study. The study was retrospective and can have the possibility of inherent errors of confounding when the exposure is not controlled. Indeterminate scan results were included in the study, and the exact cause of such a result was not evaluated. The clinical indication of the study was retrospectively examined from electronic medical records and the PET/CT requisitions. The exact perspective of the clinician ordering the study was not collected prospectively, and we may have underestimated the clinical suspicion before the scans, which may have overestimated the number of studies we classified as routine follow-up scans. The survival data were obtained from a public registry and the patient records at our hospital. There may be a time lag between death and the public registry update.
CONCLUSION
Our study showed that the fourth and subsequent follow-up 18F-FDG PET/CT studies add value to clinical assessment, have an impact on treatment planning, and predict prognosis in patients with colorectal cancer patients. This study supports that the number of follow-up scans obtained for each patient should be planned on the basis of the individual patient and cannot be generalized for the whole subset of colorectal cancer patients.
Footnotes
Published online May 7, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication February 20, 2015.
- Accepted for publication April 25, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}