


Abstract
RGD (arginylglycylaspartic acid)–based imaging tracers allow specific imaging of integrin αvβ3 expression, proteins overexpressed during angiogenesis; however, few studies have investigated the potential of these tracers to monitor responses of antiangiogenic or radiation therapy. In the studies presented here, 111In-RGD2 was assessed for its potential as an imaging tool to monitor such responses to therapies. Methods: DOTA-E-[c(RGDfK)]2 was radiolabeled with 111In (111In-RGD2), and biodistribution studies were performed in mice with subcutaneous FaDu or SK-RC-52 xenografts after treatment with either antiangiogenic therapy (bevacizumab or sorafenib) or tumor irradiation (10 Gy). Micro-SPECT imaging studies and subsequent quantitative analysis were also performed. The effect of bevacizumab, sorafenib, or radiation therapy on tumor growth was determined. Results: The uptake of 111In-RGD2 in tumors, as determined from biodistribution studies, correlated well with that quantified from micro-SPECT images, and both showed that 15 d after irradiation 111In-RGD2 uptake was enhanced. Specific or nonspecific uptake of 111In-RGD2 in FaDu or SK-RC-52 xenografts was not affected after antiangiogenic therapy, except in head and neck squamous cell carcinoma 19 d after the start of sorafenib therapy (P < 0.05). The uptake of 111In-RGD2 followed tumor volume in studies featuring antiangiogenic therapy. However, the uptake of 111In-RGD2 in FaDu xenografts was decreased as early as 4 h after tumor irradiation, despite nonspecific uptake remaining unaltered. Tumor growth was inhibited after antiangiogenic or radiation therapy. Conclusion: Here, it is suggested that 111In-RGD2 could allow in vivo monitoring of angiogenic responses after radiotherapy and may therefore prove a good clinical tool to monitor angiogenic responses early after the start of radiotherapy in patients with head and neck squamous cell carcinoma. Despite clear antitumor efficacy, antiangiogenic therapy did not alter tumor uptake of 111In-RGD2, indicating that integrin expression was not altered.
Radiolabeled RGD (arginylglycylaspartic acid) peptides allow specific and noninvasive in vivo imaging of integrin αvβ3 expression, a receptor overexpressed in the early stages of angiogenesis (1). Angiogenesis describes the formation of new blood vessels from preexisting vessels and is often regarded as one of the hallmarks of cancer (2). The literature encompasses a plethora of papers about the imaging of integrin αvβ3 by both PET and SPECT (3–5). The validation of RGD-based imaging probes often included in vivo tumor xenograft models in which integrin αvβ3 was constitutively overexpressed on tumor cells (6–13). More recently, radiolabeled DOTA-E-[c(RGDfK)]2 was also shown to allow imaging of angiogenesis itself, when used in a tumor model in which integrin αvβ3 was expressed solely on the tumor vasculature (14).
Despite the variety of previously synthesized RGD-based tracers (5) and constant production of newly synthesized, slightly superior, tracers, only a handful of studies have been performed to determine their applicability to the clinic. The first study to suggest that monomeric RGD tracers, namely 18F-galacto-RGD, could monitor the therapeutic efficacy of anticancer therapy targeting integrin αvβ3 was performed in mice bearing M21 human melanoma xenografts (15). More recently, it was also found that monomeric RGD tracers can monitor response to treatment with either antiangiogenic or antimigratory and antiproliferative therapy (16–18). So far, only one publication suggests that dimeric RGD peptide tracers can monitor response to therapy, here the antiangiogenic linifanib (19).
Increased applications of antiangiogenic therapies, such as the anti–vascular endothelial growth factor antibody bevacizumab (Avastin; Roche Pharma), and small-molecule tyrosine kinase inhibitors, such as sorafenib (20), have triggered an interest in specifically imaging angiogenesis using nuclear tracers. Monitoring response to antiangiogenic therapy with radiolabeled tracers, including but not limited to radiolabeled bevacizumab, has had its limitations (5). The focus of imaging angiogenic responses has recently moved toward using radiolabeled RGD peptides to provide specific and early feedback on the effect of antiangiogenic therapy on angiogenesis. These peptides are small with fast clearance from the blood, early imaging possibilities, and few issues regarding perfusion and permeability. If RGD-based tracers prove capable of monitoring angiogenic responses to therapy, they have the potential to select patients who might benefit from treatment with antiangiogenic drugs, beyond short-term tumor control. It is especially important to be able to monitor the efficacy of antiangiogenic therapies early on, considering overall survival is prolonged in only a limited group of patients, yet most patients still encounter side effects such as hand–foot syndrome.
Imaging angiogenesis is also important when considering treatment resistance in head and neck squamous cell carcinoma (HNSCC) patients. There are several ways in which tumors become resistant to treatment, including enhanced angiogenesis in hypoxic tumor areas (21). Being able to noninvasively monitor early on whether patients respond to therapy would allow clinicians to determine whether the treatment should be adjusted.
Here, we use HNSCC xenograft models to determine whether 111In-RGD2 can monitor responses to antiangiogenic or radiation therapy early on. The novelty is the use of tumor models in which integrin αvβ3 is expressed only on angiogenic blood vessels (14). We also investigated the use of 111In-RGD2 as a tool to monitor antiangiogenic therapy in integrin αvβ3–positive tumors (22).
MATERIALS AND METHODS
Cell Culture and In Vivo Studies
FaDu human pharynx squamous cell carcinoma cells, lacking constitutive integrin αvβ3 expression, and SK-RC-52 human renal carcinoma cells, constitutively expressing integrin αvβ3, were cultured in RPMI 1640 medium with 10% (v/v) fetal calf serum and 1% glutamine (Invitrogen). Cells were maintained at 37°C in a humidified 5% CO2 atmosphere and routinely passaged using a 0.25% trypsin/ethylenediaminetetraacetic acid solution (Invitrogen).
In vivo, tumor volumes were measured by caliper. All animal experiments were approved by the local Animal Welfare Committee in accordance with Dutch legislation and performed in accordance to their guidelines. A visual representation of the treatment schedule is presented in Supplemental Figure 1 (supplemental materials are available at http://jnm.snmjournals.org).
Antiangiogenic and Radiation Therapies
FaDu (5 × 106) or SK-RC-52 (2 × 106) cells in RPMI 1640 were injected subcutaneously on the right flank of female BALB/c nu/nu mice (Janvier). When tumors reached 100 or 10 mm3, for FaDu and SK-RC-52 xenografts, respectively, mice were injected intraperitoneally with bevacizumab at 1 or 10 mg/kg in 200 μL of saline or vehicle alone (day 0). Bevacizumab or vehicle was administered on days 0, 4, and 8. In a separate study, mice bearing FaDu xenografts of 100 mm3 were injected daily with sorafenib (0.25–1 mg/mouse) in 4% Cremophor and 3% ethanol in sterile saline or vehicle alone (intraperitoneally).
In irradiation studies, FaDu cells (1 × 106) in RPMI 1640 were injected subcutaneously in the right hind limb of female BALB/c nu/nu mice. When tumors reached 200 mm3, anesthetized mice (isoflurane/air/O2, 5% induction, 3% maintenance) were covered in custom-made lead shielding, to locally irradiate the tumor only, at 10 Gy using a 320 kV X-RAD system (RPS Services Limited) at 3.8 Gy per minute. Control mice were sham-irradiated. A visual representation of the treatment schedule in presented in Supplemental Figure 1.
Radiolabeling
One microgram of DOTA-E-[c(RGDfK)]2 (Peptides International (7)) (E = glutamate, c = cyclic, RGD = arginylglycylaspartic acid, DOTA-E-[c(RGDfK)]2 = RGD2) in 0.1 M 2-(N-morpholino)ethanesulfonic acid, pH 5.5, was incubated with 0.5–20 MBq of 111InCl3 (Malinckrodt Medical) for 20 min at 95°C. Purification and quality control were also performed as described previously to ensure that a radiochemical purity of 95% was achieved (14).
Biodistribution and Micro-SPECT/CT Imaging Studies
In biodistribution studies, mice with FaDu or SK-RC-52 xenografts, treated with or without antiangiogenic or radiation therapy, were injected intravenously with 1 μg of 111In-RGD2 (≤1MBq) in 200 μL of 0.5% bovine serum albumin in phosphate-buffered saline. Mice were euthanized by CO2/O2 1 h after tracer injection. Blood, tumor, organs, and tissues were dissected, weighed, and counted in a γ counter, and the percentage injected dose per gram (%ID/g) within them determined. Non–receptor-mediated localization of the radiolabeled peptide was investigated by determining the biodistribution of 111In-RGD2 in the presence of an excess (50 μg) of unlabeled peptide.
In micro-SPECT imaging studies, mice with FaDu tumor xenografts were injected intravenously with 1 μg of 111In-RGD2 (20 MBq) after local irradiation. One hour after tracer injection, mice were scanned under anesthesia (isoflurane/air/O2, 5% induction, 3% maintenance) using the U-SPECT-II/CT scanner (MILabs) (23). SPECT scans were acquired as 3 frames of 15 min, followed by a CT scan for anatomic reference (SPECT: spatial resolution 160 μm, 65 kV, 615 μA). SPECT scans, all frames combined, were reconstructed with software from MILabs, using an ordered-subset expectation maximization algorithm, with a voxel size of 0.4 mm.
Quantitative SPECT Analysis
Reconstructed micro-SPECT scans were coregistered with CT images using Inveon Research Workplace software (version 3.0; Siemens Preclinical Solutions). The regions of interest were determined using CT scans, and the mean voxel intensity within these was determined from SPECT scans. Mean voxel intensity values were converted to %ID/g using decay correction and a standard curve (mean voxel intensity vs. kBq) acquired by scanning and reconstructing known 111In activities from 3.7 to 370 kBq in 200 μL in a 0.5-mL Eppendorf tube (Eppendorf) under the same conditions as the animal scans.
Immunohistochemistry
Flash-frozen tumor sections (5 μm) also used for the tumor uptake studies were stained for murine integrin β3 (CD61), a marker of angiogenic integrin αvβ3, and 9F1, a marker of murine blood vessels, as described previously (14). In general, staining intensities for CD61 was weak, as target density was low, and strong, respectively. Slides were scored on the basis of the area of the section positively stained, with +, ++, and +++ equaling ≤5%, 6%–10%, and 11%–20%, respectively.
Statistical Analysis
Statistical analysis was performed using a 1-sample t test with GraphPad Prism (version 5.03; GraphPad Software). Statistical significance was represented as P ≤ 0.05, 0.01, and 0.001. Data in tables, biodistribution, and quantitative SPECT studies are average ± SD (n = 2–4 or 3–4/group, respectively). Data in tumor growth studies are average ± SE (n = 3–5/group).
RESULTS
Antiangiogenic Therapy
Bevacizumab therapy proved effective (Fig. 1) as at 10 mg/kg it halted tumor growth of both FaDu and SK-RC-52 tumor xenografts (Fig. 1). As early as 4 d after the start of therapy, growth of SK-RC-52 tumor xenografts was inhibited significantly, with tumor volumes equaling 15 ± 9 and 10 ± 3 mm3 in control and treated mice, respectively (P ≤ 0.05; Fig. 1A). The growth of FaDu tumor xenografts was halted significantly at 11 d after the start of therapy; tumor volumes were 362 ± 129 and 134 ± 121 mm3 in control and treated mice, respectively (Fig. 1B). On the other hand, injection of 1 mg of bevacizumab per kilogram did not affect tumor growth in FaDu tumor xenografts (data not shown).
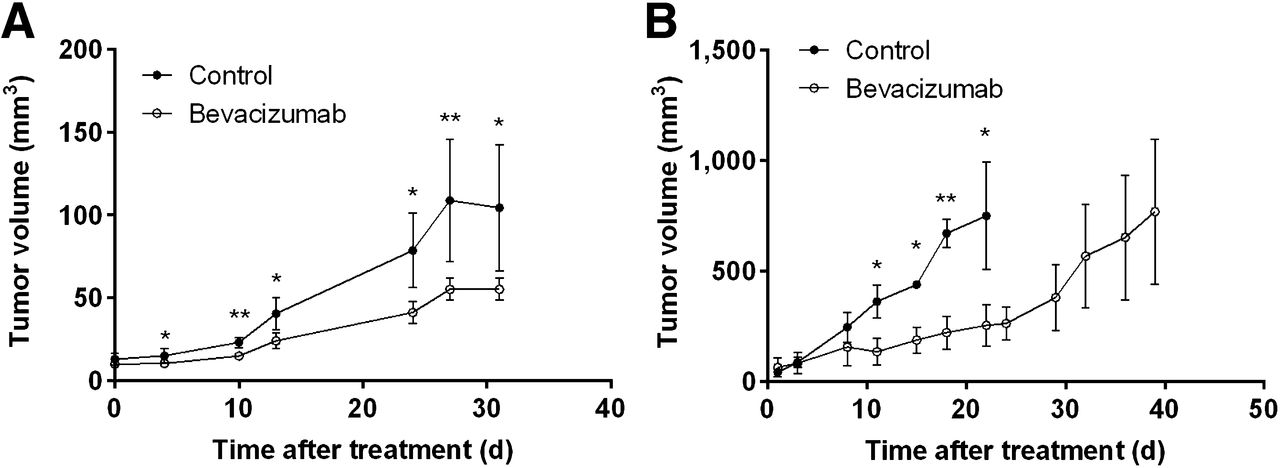
Tumor growth study of mice with SK-RC-52 (A) or FaDu (B) xenografts treated with bevacizumab. *P ≤ 0.05. **P ≤ 0.01.
Tumor uptake of 111In-RGD2 after bevacizumab treatment did not differ significantly from controls (Fig. 2). At 2 d after the start of therapy, uptake of 111In-RGD2 within SK-RC-52 tumors was 4.78 ± 0.26 and 5.18 ± 0.49 %ID/g in control and treated mice, respectively (Fig. 2A). Figure 2B shows similar results for the FaDu tumors, with uptake of 111In-RGD2 equaling 1.28 ± 0.20 and 1.30 ± 0.54 %ID/g in control and treated mice, respectively, at day 3.

Bevacizumab therapy. Uptake of 111In-RGD2 in SK-RC-52 (A) or FaDu (B–D) tumor xenografts in mice treated with bevacizumab. (D) Tumor uptake of 111In-RGD2 in individual tumors plotted against tumor volume. *P ≤ 0.05. **P ≤ 0.01.
Nevertheless, uptake of 111In-RGD2, when expressed as %ID/tumor, did differ for FaDu xenografts (Figs. 2C and 2D). At 10 d after the start of bevacizumab therapy, tumor uptake of 111In-RGD2 was 0.30 ± 0.03 %ID and 0.16 ± 0.03 %ID, in control and treated mice, respectively (P < 0.05). Nonspecific uptake remained unaltered (Table 1).
Uptake (%ID/g) of 111In-RGD2 Plus 50 μg of RGD2 in Mice Treated with Bevacizumab
Sorafenib therapy was not effective at 0.25 mg/mouse but did halt tumor growth at doses of 0.75 mg/mouse or greater as early as 5 d after the start of therapy (data not shown; Fig. 3A), with tumor volumes equaling 172 ± 90 and 84 ± 55 mm3 in control and treated mice, respectively.
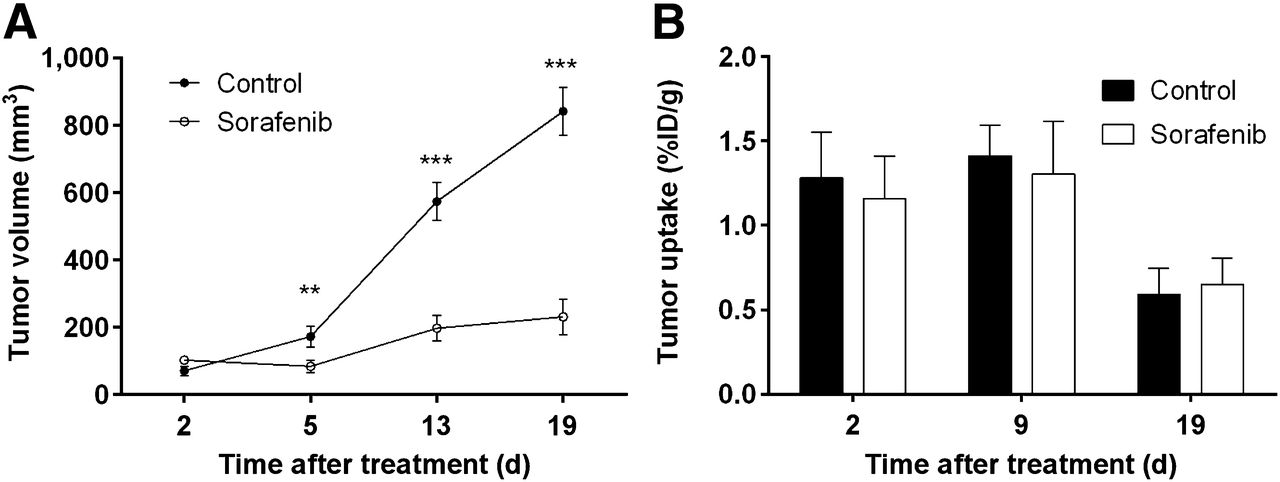
Sorafenib therapy. Tumor growth (A) and biodistribution (B) study in mice with FaDu xenografts treated with sorafenib. **P ≤ 0.01. ***P ≤ 0.001.
The uptake of 111In-RGD2 in FaDu tumor xenografts does not differ between control and sorafenib-treated mice (Fig. 3B). At 9 d after the start of therapy, tumor uptake of 111In-RGD2 equaled 1.41 ± 0.18 and 1.30 ± 0.31 %ID/g for control and sorafenib groups, respectively.
Radiation Therapy
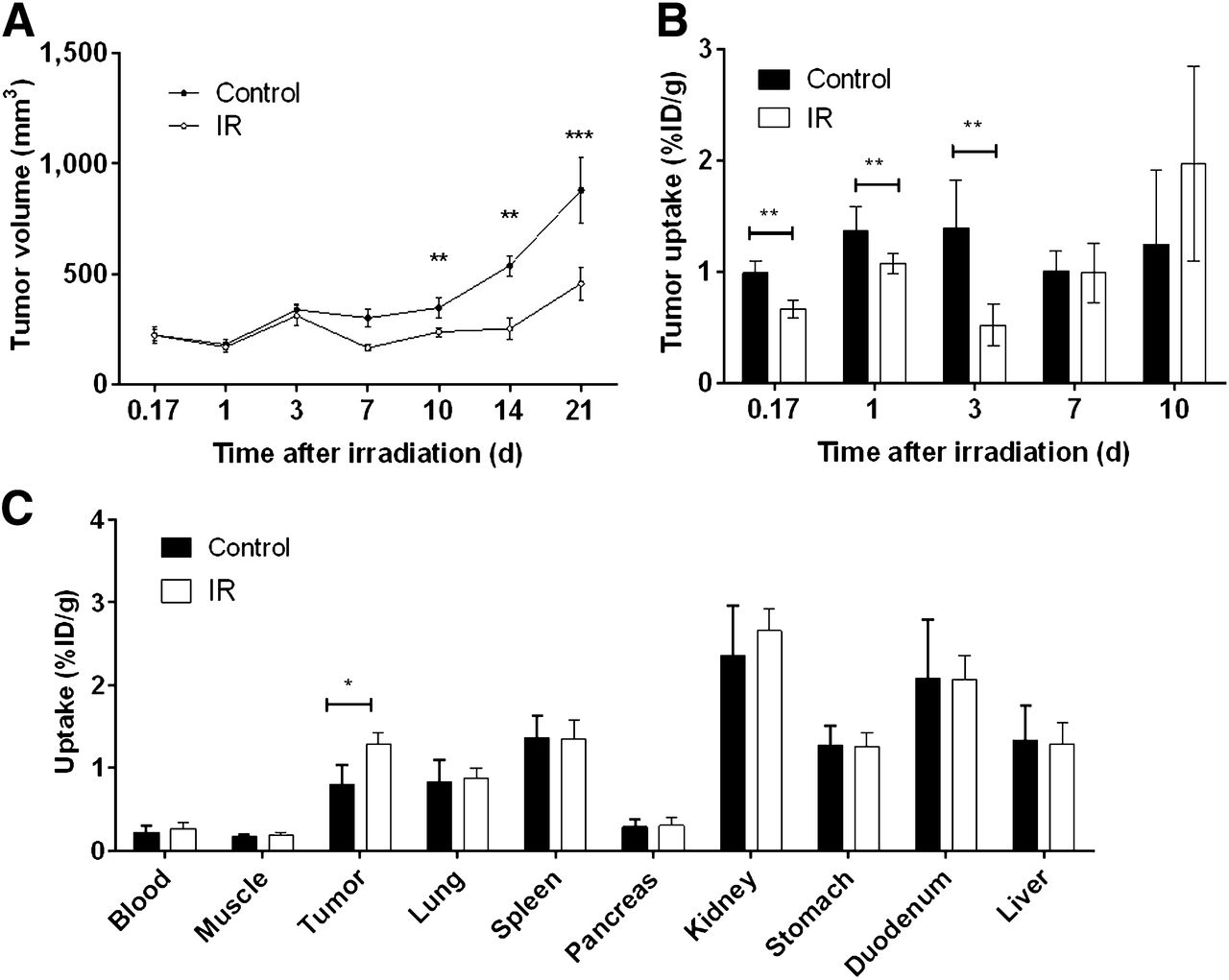
Local irradiation of FaDu tumors was effective in halting tumor growth. Ten days after irradiation, tumor volumes equaled 347 ± 124 and 238 ± 58 mm3 in control and irradiated mice, respectively (Fig. 4A). At day 21 after irradiation, this effect was even more substantial; tumor volumes were 878 ± 414 and 457 ± 212 mm3 in control and locally irradiated mice, respectively.
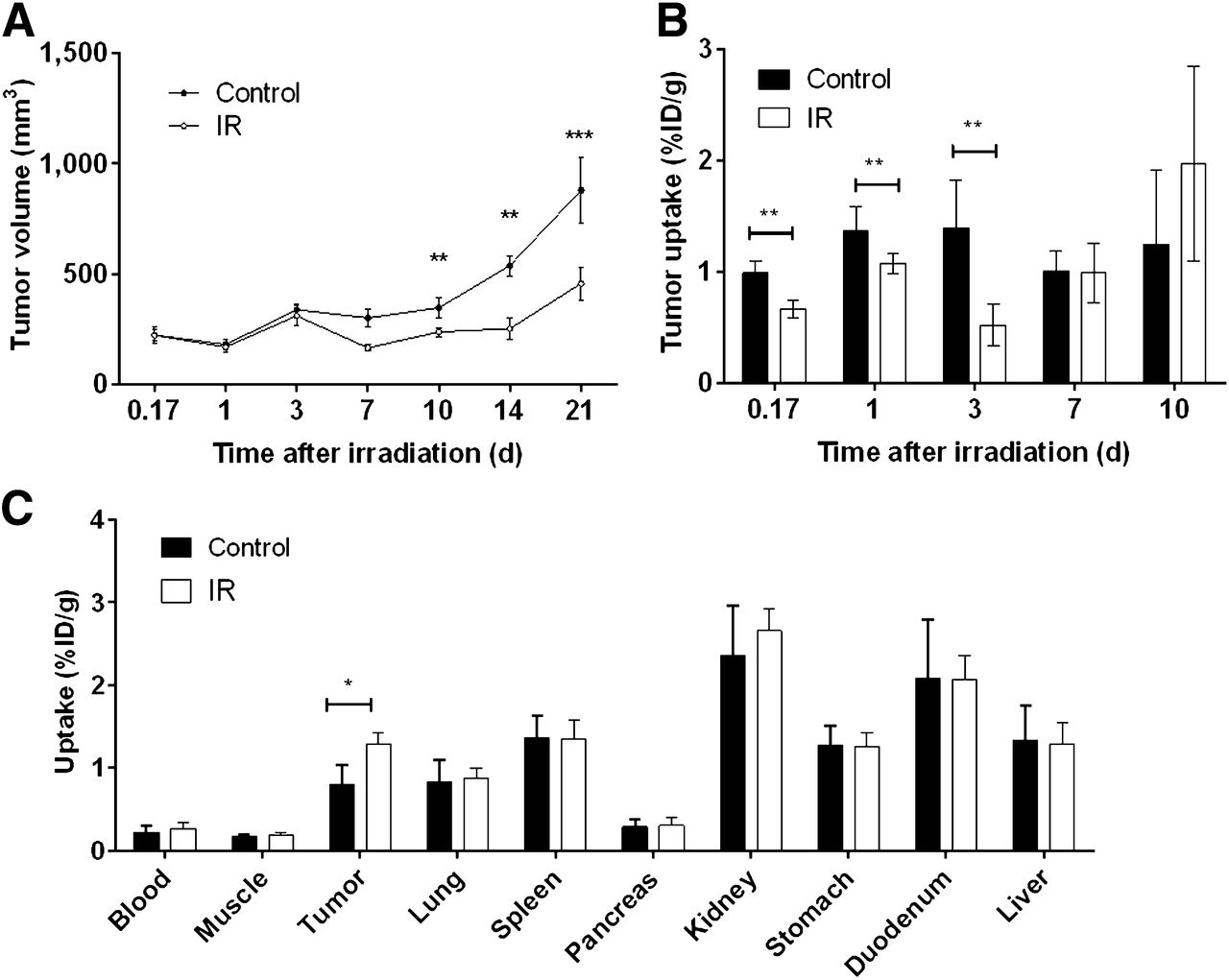
Radiation therapy. Tumor growth (A) and biodistribution (B) studies in irradiated (IR) mice with FaDu xenografts. (C) Tracer uptake in tissues at day 15 after local irradiation. *P ≤ 0.05. **P ≤ 0.01. ***P ≤ 0.001.
In irradiated FaDu tumors, the uptake of 111In-RGD2 altered significantly as early as 4 h (0.17 d) after local irradiation; uptake values were 0.99 ± 0.11 and 0.67 ± 0.08 %ID/g in control and locally irradiated mice, respectively (P < 0.01; Fig. 4B). At 7 d after irradiation, the significant decrease in tracer uptake within FaDu tumor xenografts was absent. At 15 d after irradiation, the opposite trend is observed as tumor uptake of 111In-RGD2 is significantly enhanced after local irradiation (1.28 ± 0.14 %ID/g), compared with nonirradiated mice (0.80 ± 0.23 %ID/g; Fig. 4C).
Non–Target-Mediated Effects
Tables 1 and 2 show that in general, bevacizumab or sorafenib treatment of mice bearing either SK-RC-52 or FaDu tumor xenografts did not affect nonspecific tumor uptake of 111In-RGD2 as determined by the coinjection of an excess of unlabeled RGD2. For example, tumor uptake within SK-RC-52 tumors at 10 d after the start of bevacizumab therapy equaled 0.48 ± 0.05 and 0.48 ± 0.07 %ID/g in control and treated animals, respectively (Table 1). Also, nonspecific uptake of 111In-RGD2 in control and sorafenib-treated mice did not alter until day 19 after the start of therapy, with uptake values ratios equaling 0.19 ± 0.01 and 0.28 ± 0.03 in control and treated mice, respectively (Table 2). Table 3 shows that local tumor irradiation did not affect the uptake of 111In-RGD2 plus an excess of nonlabeled RGD2, as tumor uptake values equaled 0.44 ± 0.06 and 0.59 ± 0.28 %ID/g in control and locally irradiated mice, respectively, at day 7 after irradiation.
Uptake (%ID/g) of 111In-RGD2 Plus 50 μg of RGD2 in FaDu Xenografts in Mice Treated with Sorafenib
Uptake (%ID/g) of 111In-RGD2 Plus 50 μg of RGD2 in Irradiated FaDu Xenografts
Micro-SPECT/CT Imaging and Quantitative SPECT Analysis
In fused SPECT/CT scans, FaDu tumors were visualized with 111In-labeled RGD2. Tumor uptake of 111In-RGD2 mainly localized to the periphery of the tumor (Fig. 5).

Representative 3-dimensional micro-SPECT/CT image of BALB/c nu/nu mouse with subcutaneous FaDu tumor xenograft on its right hind limb (arrow).
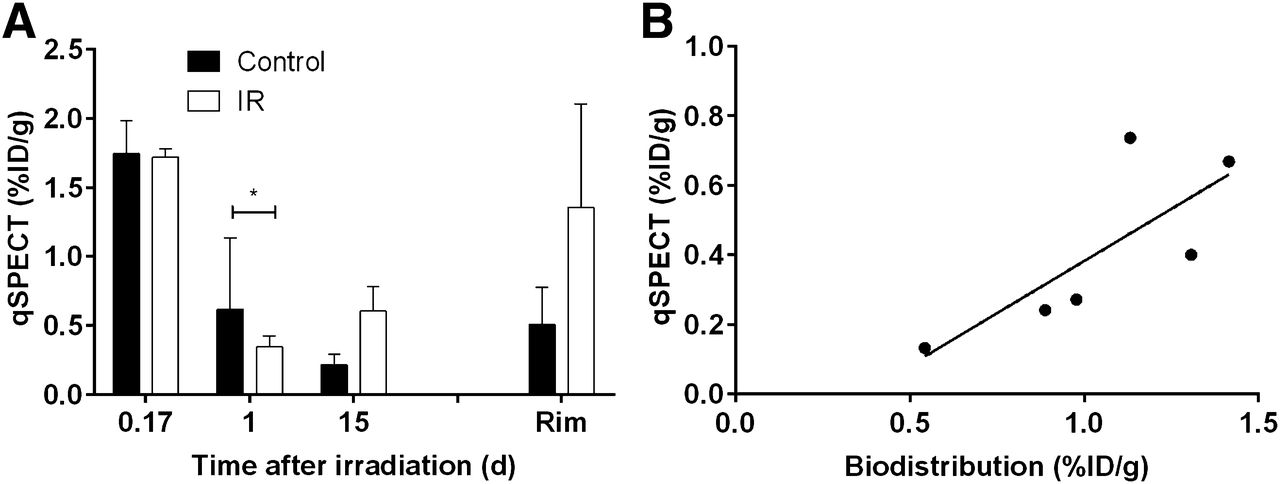
Quantitative analysis of SPECT images showed that uptake of 111In-RGD2 (%ID/g) within the tumor decreased at 1 d after irradiation (0.30 ± 0.07 %ID/g), compared with nonirradiated controls (0.53 ± 0.45 %ID/g) (P < 0.05), yet was enhanced at day 15 in irradiated tumors (0.60 ± 0.18 %ID/g), compared with controls (0.22 ± 0.07 %ID/g) (P = 0.06; Fig. 6A). The uptake in the rim of tumors (0.51 ± 0.27 %ID/g), as measured by quantitative SPECT, was significantly enhanced in tumors of nonirradiated mice, compared with the uptake of 111In-RGD2 in the whole tumor (P = 0.02; Fig. 6A).

(A) Uptake of 111In-RGD2 within tumors or rim of tumors (day 15) as quantified from micro-SPECT images in irradiated (IR) mice (n = 2–3/group). (B) Tumor uptake of 111In-RGD2 at 15 d after tumor irradiation as quantified from micro-SPECT images plotted against values derived from biodistribution studies. *P ≤ 0.05.
Correlation analysis of tumor uptake of 111In-RGD2, measured by quantitative SPECT, and tumor uptake of 111In-RGD2, measured in ex vivo biodistribution studies, confirmed that uptake can be monitored noninvasively by imaging, with a Spearman r value of 0.6 (Fig. 6B).
Immunohistochemistry
The immunohistochemical results for integrin β3 expression on murine vasculature (CD61) in mice treated with antiangiogenic therapy or radiation therapy are summarized in Table 4. No significant changes in either integrin β3 (Table 4) or 9F1 expression (data not shown) were observed at any time point.
Integrin β3 Expression on New Blood Vessels (CD61) of FaDu Xenografts in Control Mice or Mice Treated with Bevacizumab, Sorafenib, or Local Irradiation
DISCUSSION
Here, the potential of 111In-RGD2 to act as a tool to monitor the effect on angiogenesis of antiangiogenic or radiation therapy was investigated. The HNSCC xenografts used in these studies express only integrin αvβ3 on angiogenic blood vessels, making them an ideal model for studies involving RGD tracers and angiogenesis. Some studies also suggested that these tracers could monitor response to antiangiogenic therapy in integrin αvβ3–overexpressing tumor models, which corresponds with monitoring viable tumor mass (16,19); we therefore also studied integrin αvβ3–overexpressing tumors.
The results show that treatment of mice with bevacizumab, sorafenib, or radiotherapy was effective in inhibiting tumor growth (Figs. 1, 3A, and 4A). Interestingly, 29 d after the start of treatment with bevacizumab, growth of FaDu tumor xenografts recovered to the same rate as in nontreated mice, suggesting that the effect of bevacizumab had worn off.
111In-RGD2 proved a good tool to monitor changes, or as in this study the lack of changes, either in angiogenesis (FaDu) or in integrin αvβ3 expression on both vessels and tumor cells (SK-RC-52) after antiangiogenic treatment (Figs. 2 and 3B). As expected, uptake of 111In-RGD2 was higher in SK-RC-52 tumors than in FaDu tumors (Figs. 2A and 2B). Tracer uptake was unaltered after antiangiogenic therapy, even when tumor growth inhibition was apparent. This lack of effect is not due to altered accessibility of the tracer to the tumor, as nonspecific tracer uptake did not change after therapy (Tables 1 and 2). It is therefore likely that these antiangiogenic therapies did not alter integrin β3 (Table 4) expression, or even 9F1 expression, despite a clear antitumor effect. This notion fits with hypotheses in which integrin αvβ3 negatively regulates angiogenesis (24). Also, results may have been influenced by the fact that no mouse surrogate anti–vascular endothelial growth factor antibody was used and bevacizumab is known to alter integrin αvβ5, rather than integrin αvβ3 (25). This would not have affected tumor uptake of divalent RGD radiotracers, which have no affinity for other integrins such as αvβ5, α5β1, or αIIbβ3, with a 50% inhibitory concentration of greater than 10 mM as described previously (26).
Interestingly, treatment with sorafenib affected nonspecific uptake of 111In-RGD2 only at day 19 (Table 2), which might be explained by the fact that sorafenib is a multikinase inhibitor—it inhibits tumor growth directly (early) and affects angiogenesis later. Figures 2C and 2D suggest that 111In-RGD2 is only able to monitor tumor growth after antiangiogenic therapy and it would therefore not give any more specific or earlier information than standard Response Evaluation Criteria in Solid Tumors currently used clinically.
Monitoring angiogenesis is also important when considering HNSCC patients, whose treatment can include surgery, radiotherapy, and chemotherapy, which often have a negative impact on patients’ quality of life. Despite advances in treatment possibilities, more than 50% of patients will relapse because of treatment resistance. Being able to noninvasively monitor early on whether patients respond to therapy would allow clinicians to determine whether the treatment should be adjusted to improve patient outcome as well as quality of life.
In irradiation experiments, 111In-RGD2 proved a good, early, and sensitive tool to monitor changes in angiogenesis (Figs. 4–6). In biodistribution studies (Figs. 4B), it was shown that uptake of 111In-RGD2 in FaDu tumors decreased shortly after irradiation, whereas tumor growth was not yet significantly altered (Fig. 4A) and decreased integrin expression was not yet obvious through immunohistochemical stainings (Table 4).
Tumor uptake of 111In-RGD2 increased beyond that in controls at day 15, as seen in both biodistribution and quantitative micro-SPECT studies (Figs. 4C and 6A). Quantitative micro-SPECT, however, did not pick up the significantly decreased or enhanced uptake of the tracer within the tumor at 4 h and 15 d after irradiation, respectively (Figs. 4B and 4C), suggesting that although 111In-RGD2 can be used as an in vivo imaging tool, its readout might not always be large enough to determine whether an effect is truly negative.
Nonspecific tracer uptake was not affected after irradiation (Table 3), suggesting that at time points up to 10 d after irradiation altered tumor uptake of 111In-RGD2 was due to a change in angiogenesis and not due to general tumor physiologic changes, such as perfusion or vascular permeability. Preliminary data using tumor sections stained for 9F1 (vascularity) and also imaged for Hoechst 33342 (perfusion), which was injected just 60 s before euthanasia, suggest that neither tumor vasculature nor perfusion was diminished in the early days after irradiation (data not shown). The sensitivity of the tracer is highlighted in Table 4, where immunohistochemical analysis of integrin β3 expression remained unaltered after irradiation. Few studies have investigated the expression of integrin αvβ3 after irradiation of tumors; one study also showed that at 3 d after the last radiation fraction, expression of integrin αvβ3 in tumor xenografts was decreased (27). In vitro studies have also previously shown that integrin expression levels on endothelial cells can change within hours after radiotherapy (28,29).
Preliminary data suggest that perfusion is enhanced at day 15 in irradiated tumors by up to 40% when compared with nonirradiated tumors, which explains the enhanced tracer uptake at day 15. This finding could have major implications when planning the treatment schedules of patients for whom both radiotherapy and chemotherapy are used. On the other hand, an increased uptake of 111In-RGD2 at day 15 after irradiation could also be explained by an enhanced, though delayed, expression of integrin αvβ3, as suggested by other in vivo experiments (27,30,31). Nonetheless, the early and late effects of radiation on tumor vascularity, perfusion, and integrin αvβ3 expression require further investigation.
CONCLUSION
Here, it is suggested that 111In-RGD2 could allow in vivo monitoring of angiogenic responses after radiotherapy, but not antiangiogenic therapy, in HNSCC mouse models, indicating that, despite clear antitumor activity, antiangiogenic therapy in these tumor models does not have a mode of action driven by or affecting integrin αvβ3 expression. 111In-RGD2 may monitor both noninvasively and early on whether HNSCC patients respond to radiation therapy.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. Samantha Terry was funded by the Roche Postdoc Fellowship (RPF) Program. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Bianca Lemmers-van de Weem, Iris Lamers-Elemans, Kitty Lemmens-Hermans, and Henk Arnts for biotechnical assistance.
Footnotes
Published online Oct. 27, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication June 13, 2014.
- Accepted for publication September 8, 2014.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- In Vivo Characterization of 4 68Ga-Labeled Multimeric RGD Peptides to Image {alpha}v{beta}3 Integrin Expression in 2 Human Tumor Xenograft Mouse Models
- In Vivo Imaging of Antileukemic Drug Asparaginase Reveals a Rapid Macrophage-Mediated Clearance from the Bone Marrow
- RGD PET: From Lesion Detection to Therapy Response Monitoring