


Article Figures & Data
Figures
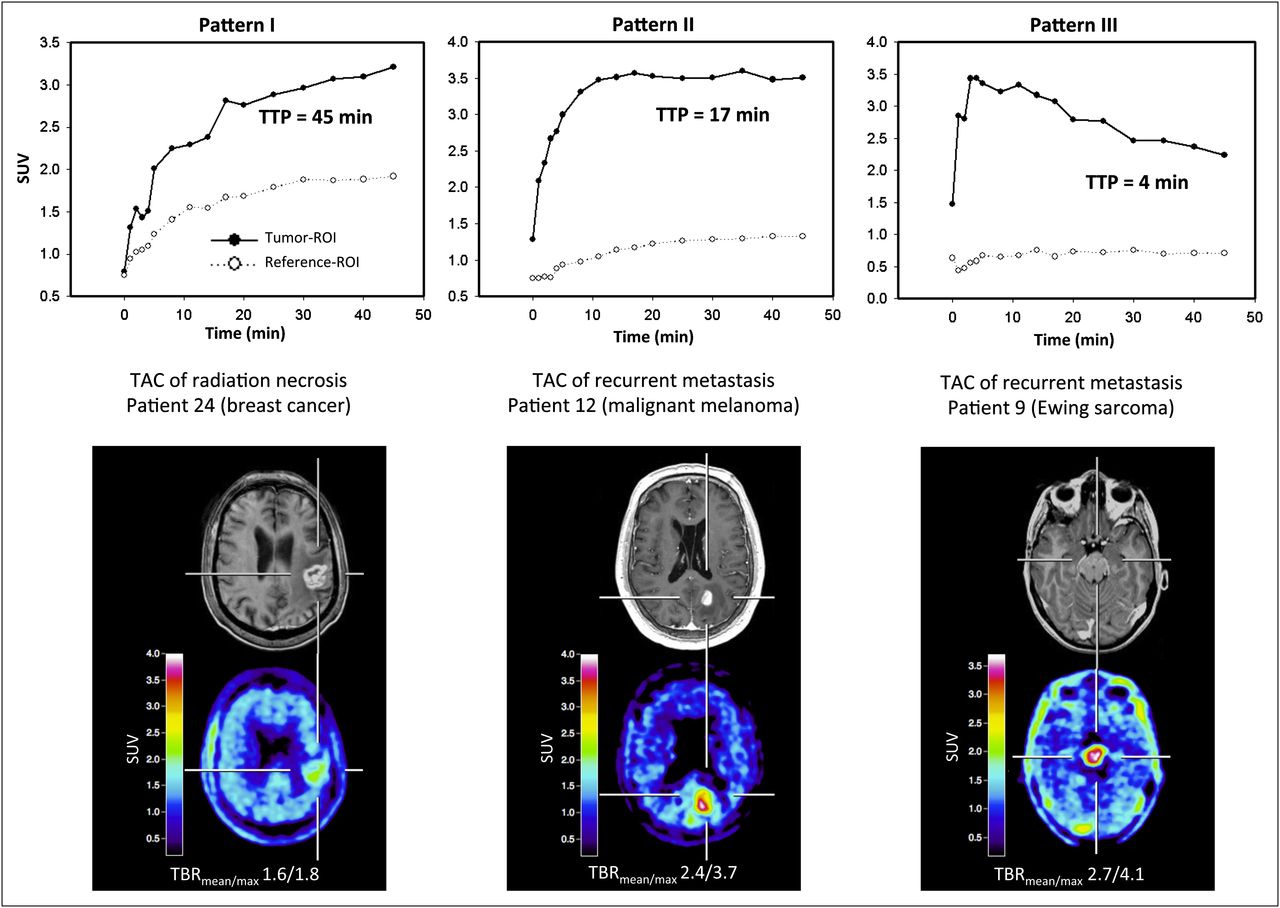
- FIGURE 1.
Examples of kinetics of radiation necrosis (pattern I) and recurrent brain metastasis (patterns II and III). All studies show pathologic contrast enhancement on T1-weighted MRI (minimal enhancement in patient 9) and corresponding increased 18F-FET uptake (TBRmean and TBRmax values are given below PET images). Dynamic evaluation of patient 24 (58-y-old woman 32 mo after SRS [brain metastasis of breast cancer, ductal carcinoma]) shows constantly increasing 18F-FET uptake until end of acquisition. TTP is 45 min. Diagnosis of radiation necrosis was based on clinical course. Dynamic evaluation of patient 12 (50-y-old man 16 mo after SRS [brain metastasis of malignant melanoma]) shows early peak of 18F-FET uptake (TTP = 17 min) followed by stable uptake until end of acquisition. Diagnosis of brain metastasis was based on clinical course. Dynamic evaluation of patient 9 (17-y-old girl, MRI findings and clinical course suggestive of first manifestation of metastatic brain tumor) shows early peak of 18F-FET uptake after 4 min followed by constant decline of uptake until end of acquisition. Diagnosis of brain metastasis was confirmed histopathologically (Ewing sarcoma). TAC = time–activity curve.
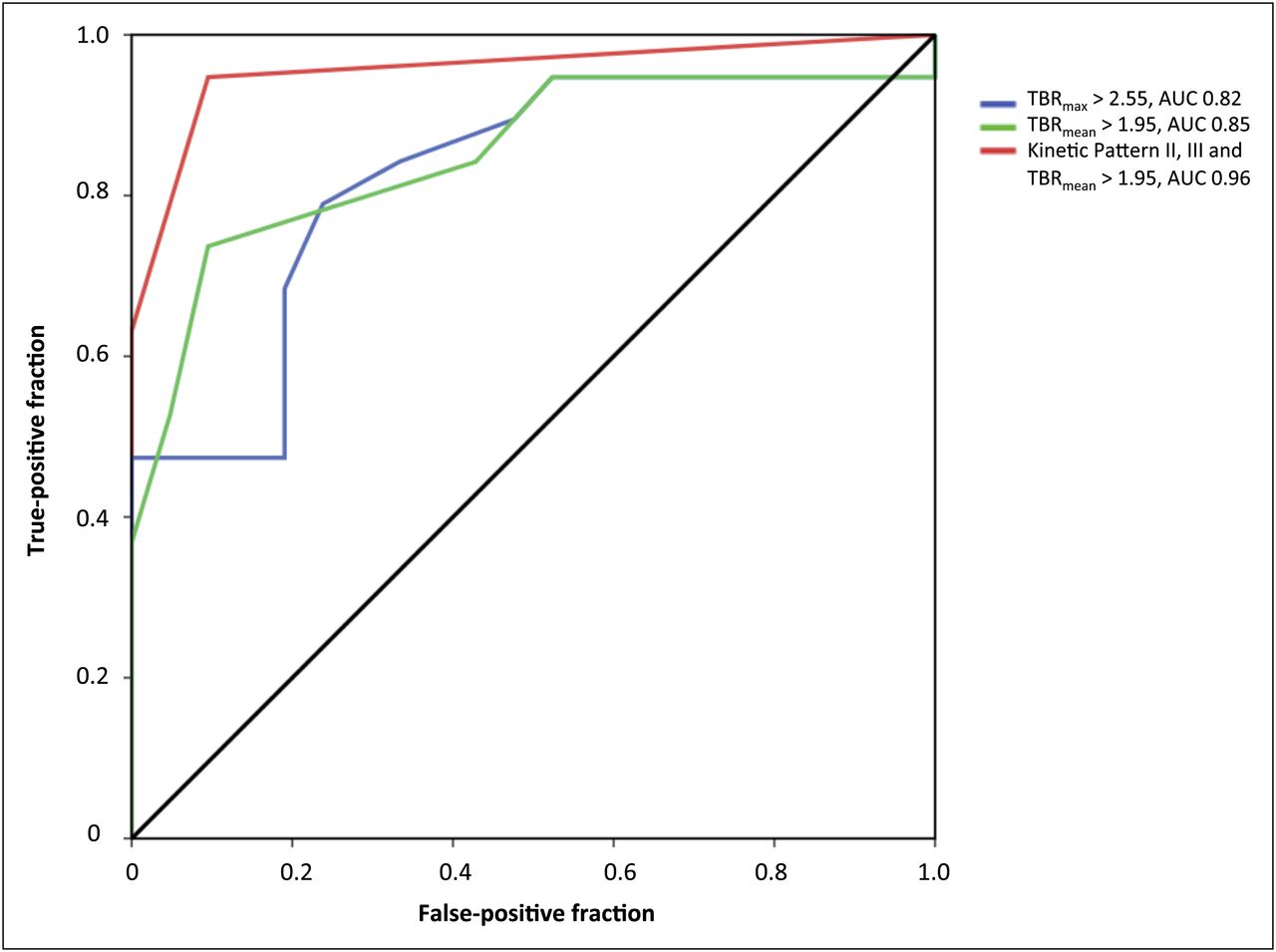
- FIGURE 2.
ROC curves for TBRmax, TBRmean, and combined use of TBRmean and curve pattern for metastatic brain tumors. AUC was 0.82 for TBRmax (blue line; optimal threshold > 2.55), 0.85 for TBRmean (green line; optimal threshold > 1.95), and 0.96 for combination of kinetic patterns II and III and TBRmean > 1.95 (red line).
- FIGURE 3.
In patient 19, with lung cancer, γ-knife SRS of left parietal metastasis induced change in kinetic pattern of 18F-FET uptake. Before SRS, values of TBRmean and TBRmax were 2.0 and 2.8, respectively, and 18F-FET uptake peaked early after 11 min and then stabilized (kinetic pattern II; top). Eleven months after SRS, values of TBRmean and TBRmax declined (1.6 and 1.8, respectively), and 18F-FET uptake pattern constantly increased (pattern I; bottom), indicating treatment response. TTP is 45 min. Sixteen months later, patient was still alive and without clinical signs of tumor recurrence. TAC = time–activity curve.


Tables
Time (mos)… Patient no. Sex Age (y) Tumor origin Histologic diagnosis Previous treatment of brain metastasis No. of PET lesions Localization TBRmax TBRmean Pattern of 18F-FET kinetic TTP (min) Histologic diagnosis after PET Between RT and PET Of follow-up after PET Final diagnosis 1 F 45 Breast DC WBRT, SRS, OP 1 Left frontal 2.7 1.9 II 20 Yes 10 ND Met 2 M 58 Lung NSCLC OP, SRS 1 L temporal 3.0 1.9 I 25 Yes 19 ND N 3 F 63 Lung NSCLC, adenocarcinoma OP, SRS 1 L frontal 2.5 1.9 I 35 Yes 19 ND N 4 F 61 Lung NSCLC WBRT, SRS 1 L parietal 1.7 1.6 I 30 Yes 9 ND N 5 F 45 Breast DC WBRT, SRS 1 L temporal 2.4 1.7 I 35 Yes 6 ND N 6 F 69 Breast DC SRS 1 L parietal occipital 2.5 1.9 I 35 Yes 60 ND N 7 F 50 Breast DC OP, WBRT, SRS 1 L temporal 3.5 2.1 I 35 Yes 6 ND Met 8 F 51 Breast DC OP, WBRT, SRS 1 R parietal 3.5 2.1 II 20 Yes 10 ND Met 9 F 17 Bone (pelvis) Ewing sarcoma SRS 1 BS 4.1 2.7 III 4 Yes 11 ND Met 10 F 57 Lung NSCLC, adenocarcinoma OP, SRS 1 L parietal 1.5 1.2 I 40 Yes 13 ND Met 11 F 48 Lung NSCLC, adenocarcinoma WBRT 1 L frontal 2.7 2.1 II 20 Yes 11 ND Met 12 M 50 Skin MM SRS 1 L occipital 3.7 2.4 II 17 No 16 Rec Met 13 F 47 Lung NSCLC, adenocarcinoma OP, WBRT, SRS 1 L occipital 3.2 2.1 I 25 No 12 38 N 14 F 69 Lung NSCLC SRS 1 R parietal 2.2 1.7 I 40 No 11 7 N 15 F 53 Colon Adenocarcinoma OP, WBRT, SRS 1 R parietal 2.2 1.7 I 45 No 10 6 N 16 F 54 Breast DC WBRT, SRS 2 L cerebellar (1) 3.5 2.0 II 20 No 11 Rec Met L cerebellar (2) 3.6 2.2 II 20 17 F 64 Lung SCLC WBRT, SRS 2 L frontal 2.5 1.9 III 14 No 7 Rec Met BS 2.3 1.8 II 14 18 F 58 Lung NSCLC, adenocarcinoma SRS 1 R parietal 2.2 1.8 I 35 No 18 S N 19 F 43 Lung NSCLC, adenocarcinoma OP, SRS 1 L parietal 2.8 2.0 II 11 No 23 Rec Met 20 F 44 Lung NSCLC, adenocarcinoma OP, SRS 1 L parietal 1.8 1.6 I 45 No 11 16 N 21 F 44 Lung SCLC WBRT, SRS 1 L parietal occipital 2.4 1.9 I 40 No 23 S N 22 F 58 Lung NSCLC WBRT, SRS 2 R parietal occipital 2.8 2.0 I 35 No 16 Rec Met L temporal 2.4 1.8 II 17 23 M 49 Lung NSCLC, adenocarcinoma WBRT, SRS 4 R cerebellar 3.1 1.9 I 40 No 12 S N L frontal 1.9 1.7 I 40 R parietal occipital 1.8 1.6 I 40 L parietal occipital 1.6 1.5 I 30 24 F 58 Breast DC SRS 1 L parietal 1.8 1.6 I 45 No 32 12 N 25 F 56 Lung NSCLC SRS 1 R occipital 2.6 1.8 I 25 No 7 36 N 26 F 58 Lung SCLC WBRT, SRS 1 L temporal 2.1 1.9 I 45 No 5 5 N 27 M 33 Skin MM OP, WBRT, SRS 3 R parietal occipital 3.7 2.4 III 17 No 4 2* Met BS 2.6 2.0 II 17 R parietal 2.6 2.2 II 17 28 F 55 Breast DC SRS 1 L parietal 5.8 3.1 II 17 No NA 1* Met 29 F 70 Breast DC SRS 1 R occipital 3.6 2.5 II 20 No 15 Rec Met 30 F 53 Lung NSCLC, adenocarcinoma SRS 1 L frontal 2.4 1.9 I 35 No 12 S N 31 M 53 Kidney RCC OP, SRS 2 L occipital 3.0 2.0 I 30 No 15 S N L frontal 2.3 1.7 I 30 ↵* Patient died during follow-up.
RT = radiation therapy; DC = ductal carcinoma; OP = resection; ND = not determined; Met = metastasis; NSCLC = non small-cell lung cancer; N = necrosis; BS = brain stem; MM = malignant melanoma; Rec = at time of 18F-FET PET clinical signs or MRI findings consistent with recurrent metastatic tumor; S = at time of 18F-FET PET patient stable without new symptoms or MRI findings without signs of tumor progression; SCLC = small cell lung cancer; NA = not available; RCC = renal cell carcinoma;
Identification of recurrent metastatic brain tumor TBRmax > 2.55 TBRmean > 1.95 18F-FET kinetic patterns II and III 18F-FET kinetic patterns II and III in combination with TBRmean > 1.95 Sensitivity 79% 74% 84% 95% Specificity 76% 90% 100% 91% Accuracy 78% 83% 92% 93% AUC ± SE 0.822 ± 0.07 0.851 ± 0.07 — 0.959 ± 0.03 P 0.001 <0.001 <0.0001 <0.001





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- [18F]-fluoroethyl-L-tyrosine (FET) in glioblastoma (FIG) TROG 18.06 study: protocol for a prospective, multicentre PET/CT trial
- Amino Acid PET in Neurooncology
- Utility of Amino Acid PET in the Differential Diagnosis of Recurrent Brain Metastases and Treatment-Related Changes: A Meta-analysis
- Hybrid 18F-Fluoroethyltyrosine PET and MRI with Perfusion to Distinguish Disease Progression from Treatment-Related Change in Malignant Brain Tumors: The Quest to Beat the Toughest Cases
- Amino Acid PET in Neurooncology
- Treatment Monitoring of Immunotherapy and Targeted Therapy Using 18F-FET PET in Patients with Melanoma and Lung Cancer Brain Metastases: Initial Experiences
- Diagnostic Accuracy of Amino Acid and FDG-PET in Differentiating Brain Metastasis Recurrence from Radionecrosis after Radiotherapy: A Systematic Review and Meta-Analysis
- Differentiation between Treatment-Induced Necrosis and Recurrent Tumors in Patients with Metastatic Brain Tumors: Comparison among 11C-Methionine-PET, FDG-PET, MR Permeability Imaging, and MRI-ADC--Preliminary Results
- Influence of Bevacizumab on Blood-Brain Barrier Permeability and O-(2-18F-Fluoroethyl)-L-Tyrosine Uptake in Rat Gliomas
- 18F-FET PET Uptake Characteristics in Patients with Newly Diagnosed and Untreated Brain Metastasis
- Although Non-diagnostic Between Necrosis and Recurrence, FDG PET/CT Assists Management of Brain Tumours After Radiosurgery
- Pituitary Incidentaloma Found on O-(2-18F-Fluoroethyl)-L-Tyrosine PET
- 18F-FDOPA PET for Differentiating Recurrent or Progressive Brain Metastatic Tumors from Late or Delayed Radiation Injury After Radiation Treatment
- Radiolabeled Amino Acids for Oncologic Imaging
- Being Sensitive: to Specify When Amino Acid Tracers Accumulate in a Brain Lesion