


Abstract
We present here a systematic analysis of lymphoma and MM patients recruited into 2 clinical trials or treated with radretumab according to compassionate use, describing the biodistribution, dosimetry, safety, and clinical activity of radretumab. Methods: Uptake in lymphoma lesions, safety, and clinical activity of radretumab radioimmunotherapy (R-RIT) were evaluated in 18 relapsed lymphoma or multiple myeloma patients. Results: In 14 of 18 patients, selective tumor uptake was found; 11 of 15 lymphoma patients, including 9 of 11 with Hodgkin lymphoma (HL), were eligible for R-RIT (a priori criteria–based target-to-bone marrow ratio > 10:1 for EudraCT no. 2005-000545 or > 4:1 for EudraCT no. 2007-007241-12 at dosimetric imaging). Two HL and 1 diffuse large B cell lymphoma patient achieved complete response; 1 HL patient had partial response. Both multiple myeloma patients receiving R-RIT experienced stabilization of disease. Therefore, the overall objective response rate was 40%. Uncomplicated grade 3–4 thrombocytopenia or leukocytopenia was observed in 5 R-RIT patients, lasting 4–129 d. Conclusion: R-RIT showed a favorable benefit and risk profile in advanced relapsed lymphoma patients and induced complete response in 2 heavily pretreated, relapsed HL patients and in 1 diffuse large B cell lymphoma patient. These results warrant further exploration of R-RIT in larger phase II clinical trials.
Radioiodinated L19SIP (radretumab), a fully human antibody in the small immunoprotein format that binds with high affinity to the extradomain-B splice variant of fibronectin (EDB) (1–3), combines the unique feature of pan-tumor targeting with a favorable pharmacokinetic profile (4–7).
Preclinical data have shown its efficient localization in tumoral neovasculature and complete tumor eradication in animal models, using EDB-binding immunocytokines (6). Strong EDB expression in almost all lymphoma subtypes and in the bone marrow (BM) from multiple myeloma (MM) patients, selective uptake of radretumab in lymphoma lesions, and partial response (PR) in 2 Hodgkin lymphoma (HL) patients receiving radioimmunotherapy with radretumab (R-RIT) have also been reported (7). We present here a systematic analysis of lymphoma and MM patients recruited into 2 clinical trials or treated with radretumab according to compassionate use, describing the biodistribution, dosimetry, safety, and clinical activity of radretumab.
MATERIALS AND METHODS
Study Design and Patients
We analyzed a total of 18 patients (HL, n = 11; non-Hodgkin lymphoma [NHL], n = 4; and MM, n = 3) enrolled into 2 sequential prospective multisite trials (EudraCT no. 2005-000545-11, n = 12; EudraCT no. 2007-007241-12, n = 3; the detailed protocol is provided in the supplemental material [available online only at http://jnm.snmjournals.org]) or treated according to the study procedure but under compassionate use. Fifteen patients were men (83%), and median age was 40 y (range, 15–73 y; Supplemental Table 1). Both trials and compassionate uses were approved by national and local authorities.
Provisional Radiation to Target Lesions and Bone Marrow
As a first step, a diagnostic-level activity (185 MBq) of 131I-L19SIP was administered to the patients for dosimetric estimates. Patients who met a priori–defined criteria based on the ratio between adsorbed dose to the most avid tumor lesion and the BM (>10:1 for EudraCT no. 2005-000545 or >4:1 for EudraCT no. 2007-007241-12, supplemental material) were offered R-RIT at an activity of 3.7 or 5.55 GBq (Supplemental Fig. 1). Post-therapy scans were acquired at 1 time point between 7 and 10 d after administration.
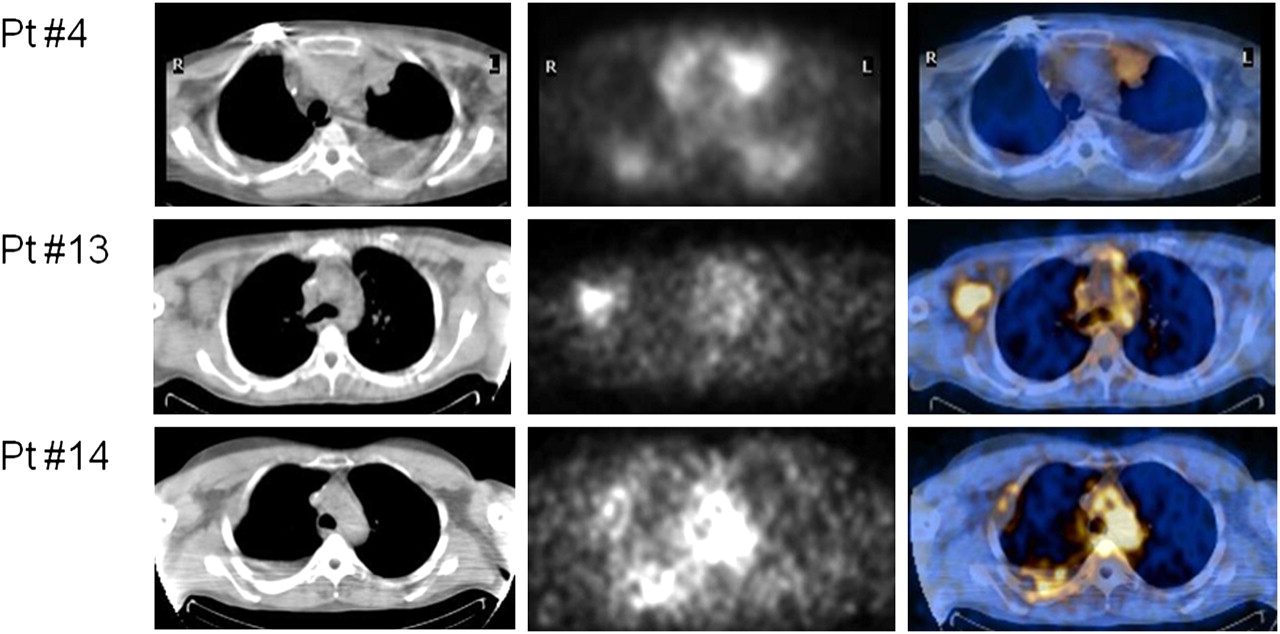
Transaxial CT (left), SPECT (center), and SPECT/CT (right) sections of 3 different patients receiving 131I-L19SIP for dosimetric study. Selective uptake is seen in left paracardial and right pleural (patient 4), right axillary (patient 13), and right thoracal and pleural (patient 14) lymphoma lesions. Pt = patient.
Radiolabeling of L19SIP
L19SIP (Philogen SpA) was radioiodinated at each study center using a modified chloramine-T technique (8), whereby 4 or 5 mg of L19SIP were labeled with 8 nM 131I-iodide (about 25 mg of chloramine-T for 4–5 mg of L19SIP; 3-min reaction time) and purified with a Hiprep 26/10 Desalting Column (GE Healthcare). Radiolabeling efficiency and immunoreactivity were always greater than 95% and greater than 90%, respectively. Administration occurred within 6 h after labeling.
Imaging and Dosimetry
After injection of 131I-L19SIP (185 MBq), sequential whole-body planar images for dosimetric estimates were acquired, as detailed in the supplemental material.
Safety and Efficacy
Toxicity and adverse events were recorded until 30 d after the last 131I-L19SIP administration, graded according to Common Terminology Criteria for Adverse Events, version 3.0, and followed until resolution. 18F-FDG PET/CT was performed 1 mo after R-RIT, and responses were confirmed at 4 wk or more after initial response assessment. Tumor response in lymphoma and MM patients was assessed according to the criteria of Cheson et al. (9) and Durie et al. (10), respectively.
RESULTS
Eligibility for R-RIT
High, selective tumor uptake of radretumab (Fig. 1) was observed in 11 of 15 lymphoma patients, including 9 of 11 HL and 2 of 4 B-cell NHL patients; these patients were therefore considered eligible for R-RIT. Two NHL and 1 HL patients exhibited moderate tumor uptake, and no radretumab uptake was found in only 1 patient (HL). In the MM patients (who had no evidence of extramedullary involvement), diffuse radretumab uptake was exclusively found in the BM, resulting in a BM-to-muscle uptake ratio of 2.5 in 2 MM patients, which was considered sufficient for subsequent R-RIT.
Provisional Organ Exposure Estimated with 185 MBq of 131I-L19SIP
Dosimetric estimates for normal organs and tumor lesions were extrapolated to an activity of 3.7 GBq on the basis of the 185-MBq 131I-L19SIP data (Fig. 2; Table 1; Supplemental Table 2). In all patients except one, the estimated BM and other healthy-organ absorbed radiation doses were within organ safety thresholds. The provisional radiation doses to lymphoma target lesions were quite heterogeneous, ranging between 0.56 and 76 Gy among patients and between 3.7 and 20.7 Gy in a single patient.
Clinical Response of Lymphoma Patients to R-RIT
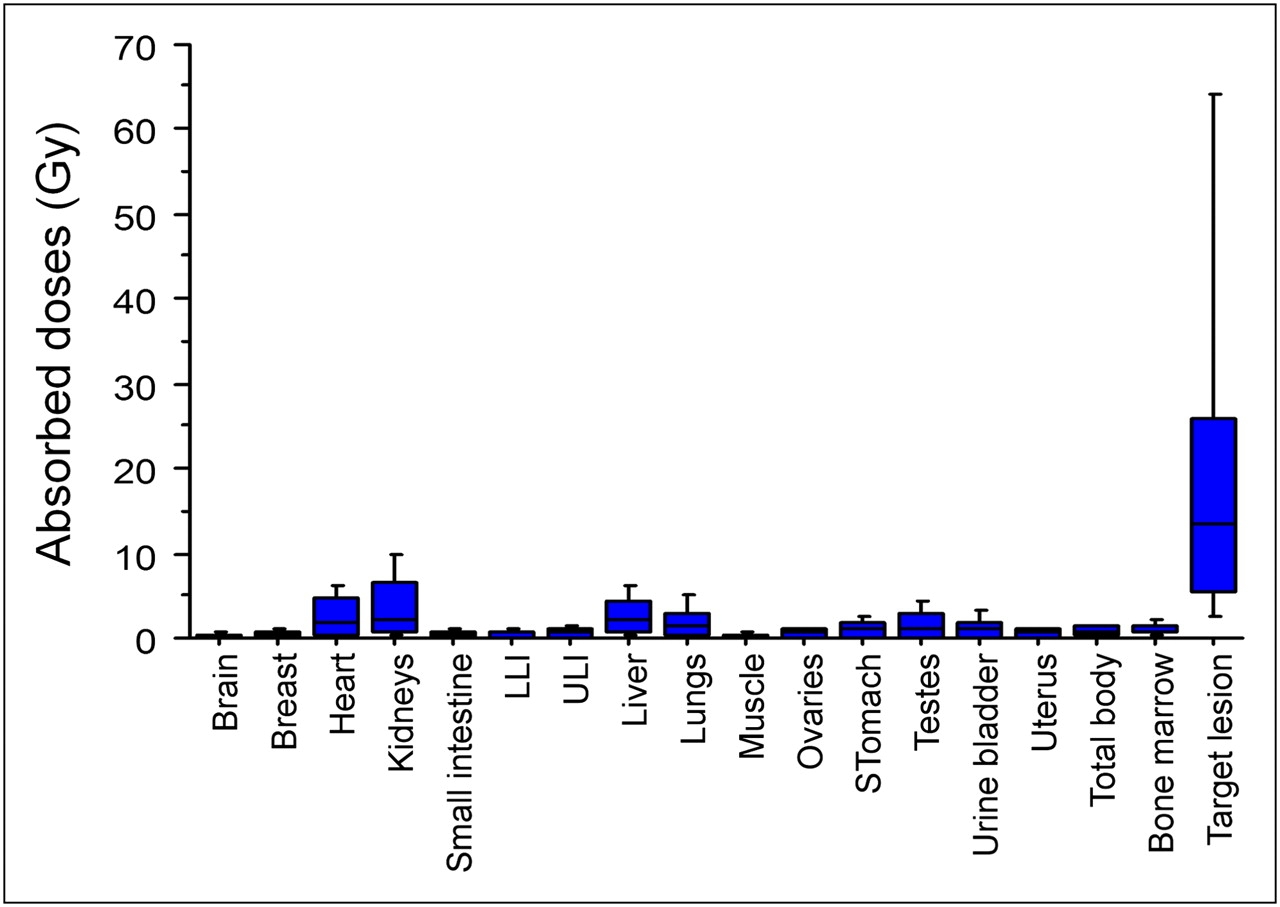
Radiation-absorbed doses (in Gy) estimated for 131I-L19SIP administered at activities intended for R-RIT (minimum and maximum values indicated by bars). LLI = lower large intestine; ULI = upper large intestine.
Efficacy of R-RIT
The 10 eligible lymphoma patients received R-RIT at an activity of 3.7 (n = 7), 5.55 (n = 2), or 1.85 GBq (patient 18, dose reduction for low body weight). Two MM patients were treated with R-RIT at 3.7 GBq and 1.85 GBq (dose reduction for preexisting grade 1 thromboleukopenia), respectively. Eight patients received 1 R-RIT administration, 3 received 2, and 1 received 5 (3.7 GBq in all cases). Repeated treatments were followed by separate efficacy evaluations, thus making a total of 19 R-RIT administrations available for efficacy assessment.
Patients’ response to R-RIT is reported in Table 2. R-RIT induced complete response (CR) after the first administration in the diffuse large B cell lymphoma (DLBCL) patient, after both the first and the second administrations in HL patient 5, and only after the second administration in HL patient 12. In all 3 patients, CR was ascertained by complete disappearance of 18F-FDG–avid disease (Fig. 3). Two rapidly progressive patients experienced a PR 1 mo after R-RIT; however, progressive disease (PD) recurred 4–6 wk thereafter.
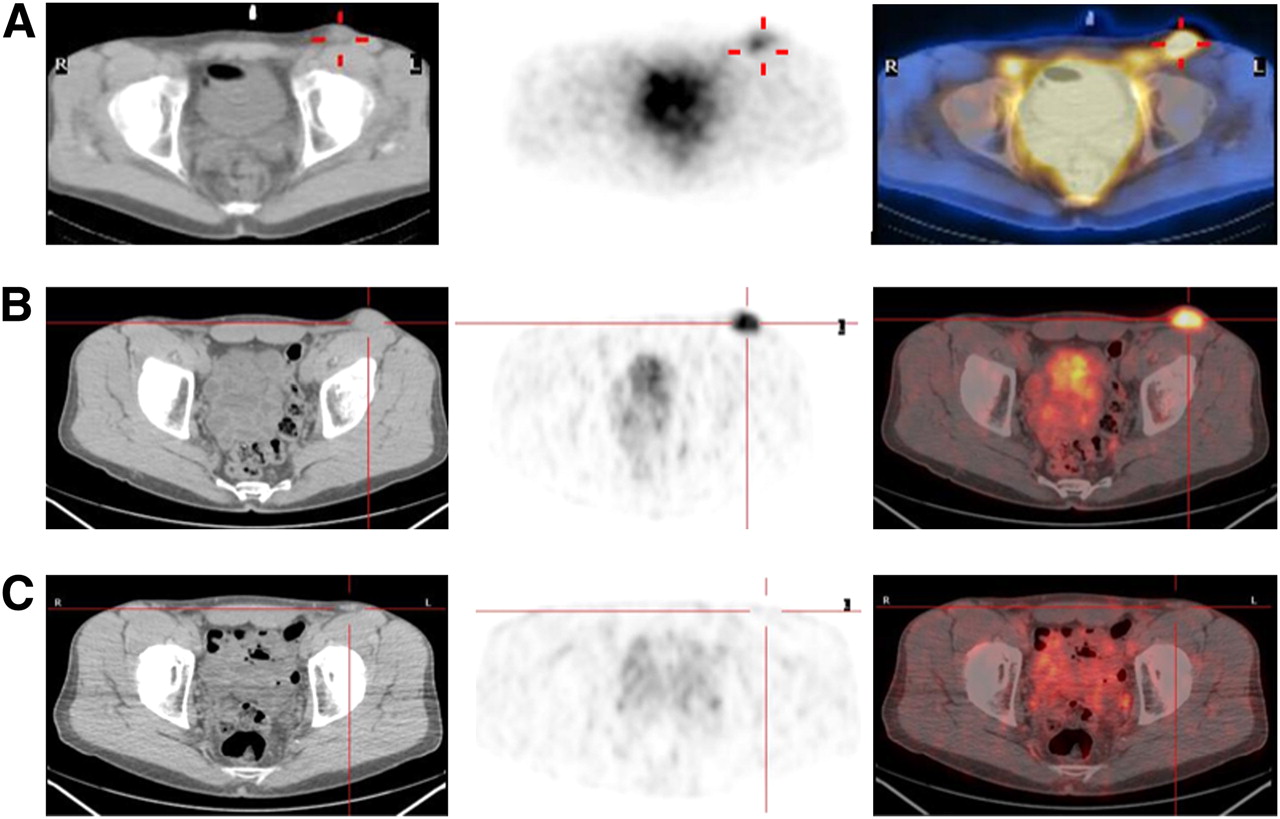
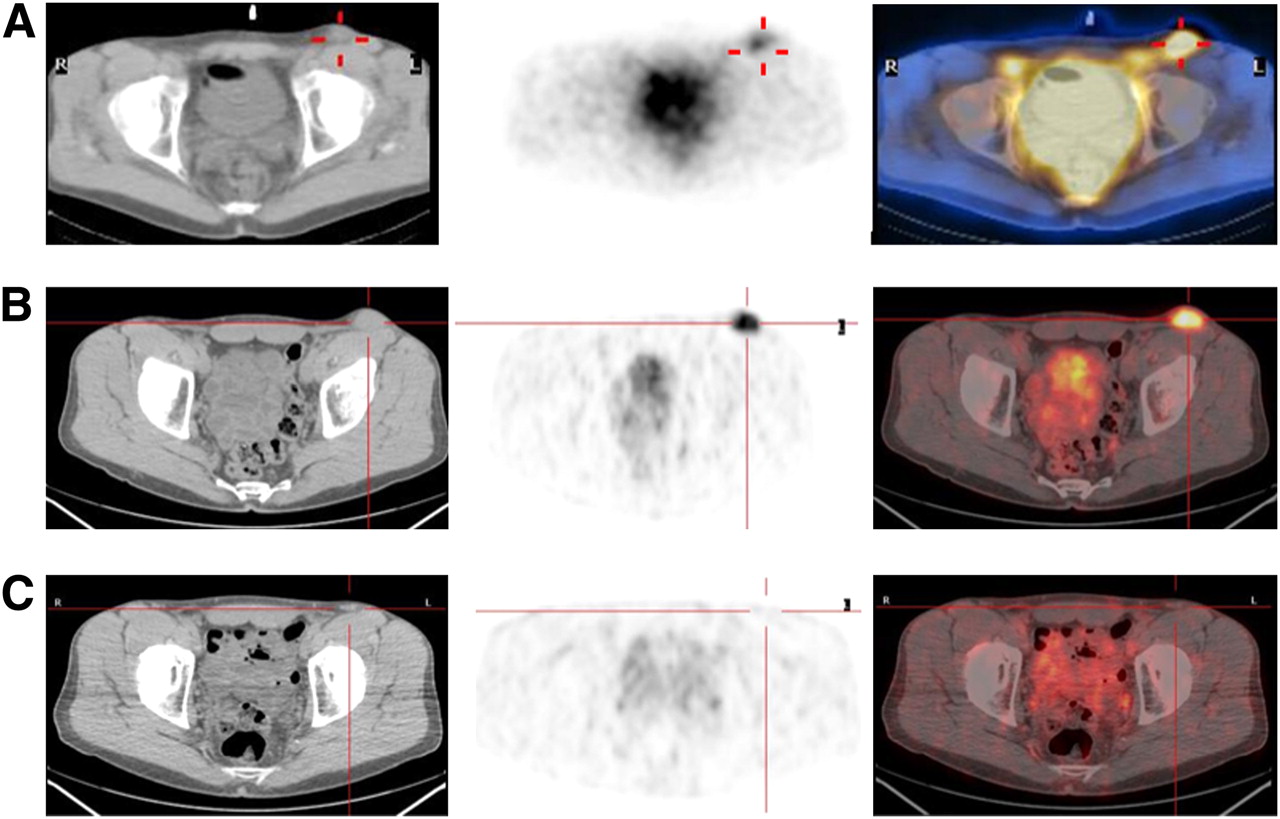
CT (left), SPECT (A center) and PET (B and C center), and SPECT/CT (A right) and PET/CT (B and C right) transaxial 131I-L19SIP and 18F-FDG PET/CT sections of DLBCL patient 17: high 131I-L19SIP uptake in left inguinal lymphoma after R-RIT (A) and at site of hypermetabolic lesion (B) and complete disappearance of 18F-FDG–avid disease after R-RIT (C).
Objective responses after R-RIT were observed in lymphoma patients with provisional doses to the target lesions exceeding 10 Gy (Table 1). In patients with CR or PR, a high provisional radiation dose to target lesions was found (20.7–76.7 Gy; Table 1). The largest completely disappearing lymphoma lesion after R-RIT was 55 mm in the longest diameter. Objective responses in bone lymphoma lesions were not observed, although transient reduction of 18F-FDG uptake was detected, associated with symptom relief. Patients progressing after R-RIT still had tumoral uptake of radretumab in subsequent scans, and the level of response to repeated R-RIT was not inferior to that observed after the first administration, except when bone was involved.
The duration of R-RIT–induced responses was 2–7 mo, although CR in the DLBCL patient has been ongoing for 15 mo (Table 2; Fig. 3). Repeated R-RIT administrations extended the clinical benefit, and in 1 HL patient the disease could be controlled for 24 mo with 5 R-RIT administrations (Fig. 4). Both MM patients treated with R-RIT achieved stable disease lasting for 5 and 2 mo (13% and 23% reductions in paraprotein serum levels, respectively).
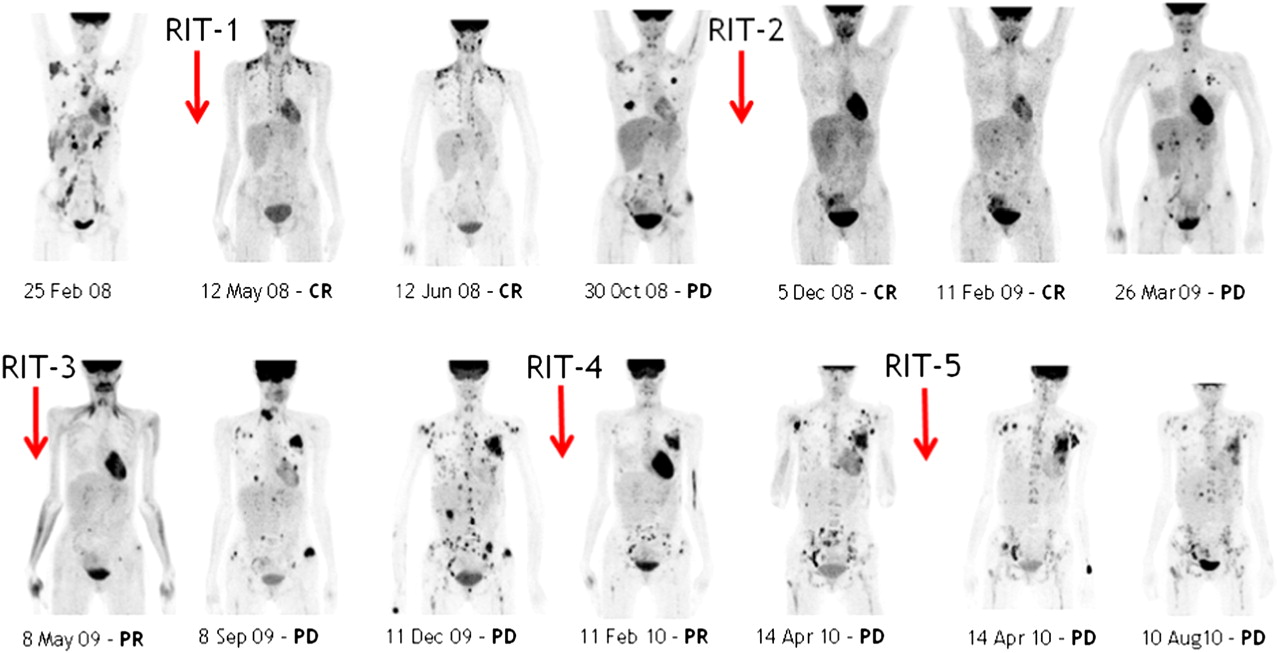
Series of 18F-FDG PET maximum-intensity-projection images taken from HL patient 5 before and after each of 5 subsequent R-RIT administrations (RIT-1 to -5) at activity of 3.7 GBq. CR was achieved after RIT-1 and RIT-2, PR was achieved after RIT-3 and RIT-4, and PD was achieved after RIT-5 (new lesions) associated with some local response.
Safety and Tolerability
After radretumab at 185 MBq, in 1 patient a grade 3 increase in alanine aminotransferase serum levels related to septic fever–induced rhabdomyolysis and in another patient a grade 3 hypopotassemia caused by prolonged grade 1 diarrhea were recorded. Both events were considered unrelated to radretumab.
R-RIT was well tolerated, even when given repeatedly. Grades 3–4 thrombocytopenia occurred in 5 patients after the first R-RIT, starting between day 22 and 41 after radioimmunotherapy and lasting for 4–21 d. Median time to platelet (<100 × 109/L) and neutrophil nadirs was 43 d (range, 25–56 d) and 44 d (range, 43–54 d), respectively (Supplemental Fig. 2). One HL patient had grades 3–4 thrombocytopenia after 5.55 GBq of R-RIT, lasting for 129 d. However, no platelet transfusions were required. Another HL patient had prolonged thrombocytopenia after repeated R-RIT at 3.7 GBq. She eventually developed secondary leukemia and died shortly thereafter. No correlation between hematologic toxicity and BM or whole-body radiation-absorbed dose was found (data not shown).
Although we did not analyze human serum for formation of humoral responses against radretumab, none of the patients receiving repeated R-RIT administrations experienced clinical adverse events possibly caused by the formation of antiradretumab antibodies.
DISCUSSION
Patients with advanced lymphoma or MM received a diagnostic dose of 131I-L19SIP for dosimetry; if tumor uptake was sufficient, they were subsequently treated with R-RIT. Safety and antitumor activity were analyzed. Selective uptake of radretumab in tumor lesions was found in most lymphoma patients, whereas diffuse BM uptake was detected in MM patients, thus corroborating earlier observations of selective EDB tumor targeting in both lymphoma and solid cancers (7,11).
R-RIT (3.7 GBq) induced CR in 2 relapsed HL and 1 DLBCL patient, whereas PR or stable disease consistent with substantial symptom relief was observed in other patients, and only 2 HL patients continued to have PD. Therefore, the combined best objective response rate of R-RIT in advanced relapsed lymphoma patients was 40%. In 1 HL patient, the antilymphoma response was stronger after the second (CR) than after the first R-RIT (PR), an observation possibly resulting from an increased EDB expression consequent to tissue damage (e.g., inflammatory response to radiation), involving angiogenic sprouting (12).
In patients who achieved a CR after R-RIT, the response duration was relatively shorter (7 mo for HL and >15 mo for DLBCL) than the 45.8 or 29.3 mo reported after RIT with tositumomab (Bexxar; GlaxoSmithKline) or with ibritumomab tiuxetan (Zevalin; Spectrum Pharmaceuticals), respectively (13,14). However, the latter longer-lasting responses were observed in patients with relapsed non-Hodgkin follicular lymphoma, one of the most radiosensitive cancers. Furthermore, contrary to our HL patients, patients treated with tositumomab or ibritumomab tiuxetan have usually not received prior high-dose chemotherapy with hematopoietic stem cell support. On the other hand, the response duration observed after R-RIT in 2 of our HL patients (5 and 7 mo, respectively) is well in line with that observed in a pretreated HL patient who achieved CR lasting for 6 mo after ibritumomab tiuxetan (15). Finally, we consider it encouraging that the CR in the DLBCL patient is still ongoing 15 mo after R-RIT.
Nevertheless, even repeated R-RIT was not sufficient for maintaining long-term disease control in advanced lymphoma patients. Therefore, R-RIT combined with concurrent chemotherapy moderately affecting the hematopoietic system (e.g., bendamustine) should be explored in advanced relapsed HL or B cell NHL patients. Because of its plasma clearance (half-life, ~30 h) and its highly selective tumor-binding properties, R-RIT seems to be well suited for this purpose. R-RIT achieved disease stabilization lasting for a few months in 2 MM patients. Clearly, more patients need to be studied before conclusions are drawn about the antitumor activity of R-RIT in this disease.
As expected, toxicity after R-RIT was mainly hematologic. Although higher activities were administered with R-RIT than with, for example, 131I-tositumomab (3 GBq) (16), hematologic toxicity was in the same range as that of the radioimmunotherapy agents approved for follicular lymphoma (17). The severity of acute hematologic toxicity could not be predicted by the BM provisional dose, in particular in patients with a compromised marrow reserve. This finding is in line with earlier reports on noncorrelation of dosimetry results with hematologic toxicity after 131I-tositumomab and 90Y-ibritumomab tiuxetan radioimmunotherapy (18,19), irrespective of the dosimetric approach used. With these agents, elapsed time after the last chemotherapy was the only factor that predicted hematologic toxicity after radioimmunotherapy (20). Long-term toxicity, such as an increased risk of secondary malignancies in the heavily pretreated patients, cannot be ruled out.
CONCLUSION
R-RIT at an activity of 3.7 GBq could be safely and repeatedly administered to relapsed lymphoma patients. It induced clinically meaningful objective responses including a CR in HL and DLBCL patients, thus constituting clinical proof of concept and a favorable benefit or risk profile in advanced relapsed lymphoma patients.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
We thank Southern Europe New Drug Organization, particularly Monica Miani for the management and support. We are grateful to Adele Longanella for monitoring the study and assistance in providing the raw data for the manuscript. No potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online May 10, 2012.
- © 2012 by the Society of Nuclear Medicine, Inc.
REFERENCES
- Received for publication November 18, 2011.
- Accepted for publication March 14, 2012.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- An IL-7 fusion protein targeting EDA fibronectin upregulates TCF1 on CD8+ T-cells, preferentially accumulates to neoplastic lesions, and boosts PD-1 blockade
- Targeted Delivery of IL2 to the Tumor Stroma Potentiates the Action of Immune Checkpoint Inhibitors by Preferential Activation of NK and CD8+ T Cells
- Antibody-Cytokine Fusions: Versatile Products for the Modulation of Anticancer Immunity
- TGF-{beta} induces oncofetal fibronectin that, in turn, modulates TGF-{beta} superfamily signaling in endothelial cells
- Targeting Interleukin-2 to the Bone Marrow Stroma for Therapy of Acute Myeloid Leukemia Relapsing after Allogeneic Hematopoietic Stem Cell Transplantation
- Therapeutic vaccination targeting the tumour vasculature
- Curative Properties of Noninternalizing Antibody-Drug Conjugates Based on Maytansinoids
- Radretumab Radioimmunotherapy in Patients with Brain Metastasis: A 124I-L19SIP Dosimetric PET Study