


Abstract
We report the effects of treadmill exercise on 18F-FDG uptake in skeletal muscles and image quality of torso PET and compare stress myocardial perfusion imaging patterns with myocardial 18F-FDG uptake. There were 3 groups of patients: 48 patients underwent PET within 8 h after a treadmill test (Ex 8), 45 patients within 48 h after a treadmill test (Ex 48), and 34 patients without prior exercise. Mean workload (8.4 ± 2.3 [Ex 8] vs. 8.9 ± 2.6 metabolic equivalents [Ex 48]) was similar in both exercise groups. Muscle uptake was assessed by standardized uptake value. Myocardial uptake patterns were compared visually. Minor differences between patient groups were noted only for maximum standardized uptake value in quadriceps muscles. There was no correlation between perfusion defects and myocardial 18F-FDG uptake patterns. Thus, treadmill exercise does not affect muscle 18F-FDG uptake or image quality on subsequent PET. Cardiac 18F-FDG uptake on torso PET scans is unrelated to myocardial perfusion status.
Skeletal muscle activity on torso 18F-FDG PET scans is often attributed to exercise or muscle spasm within hours of 18F-FDG injection. Muscle glucose flux is governed by substrate delivery, transport across the cellular membrane by glucose transporters, and the rate of phosphorylation by hexokinase in the cytosol (1). Glucose uptake is stimulated by insulin-activating glucose transporter 4 (GLUT-4) in a phosphatidylinositol-3-kinase (PI-3-K)–dependent manner (2) or by muscle contraction and exercise alone in an insulin-independent and PI-3-K–independent manner (3). The latter involves adenosine monophosphate–activated kinase (2,4), which increases substrate delivery to muscle, fatty acid uptake, β-oxidation, and glucose uptake via GLUT4. Exercise also increases nitric oxide synthase activity, and thereby muscle perfusion and substrate delivery (5), which may persist for 12 h after heavy exercise (6). Finally, exercise stimulates secretion of calcium ions from T tubules, thereby augmenting GLUT4 transcription (7). Increased mitochondrial biogenesis and increases of GLUT4 and hexokinase are detectable within hours to days of initiating an exercise program (8). The resulting increased glucose uptake in muscles can be visualized with 18F-FDG (9,10). Guidelines recommend that patients refrain from physical exercise for at least several hours before 18F-FDG PET (11,12) to improve tumor versus muscle 18F-FDG uptake and overall PET image quality. Because we occasionally encounter patients who have undergone treadmill stress testing and myocardial perfusion imaging (MPI) within hours before PET, we decided to quantify the effect of exercise on 18F-FDG muscle uptake and PET image quality. We also correlated cardiac 18F-FDG uptake with perfusion defects on MPI because some investigators suggested that it may reflect myocardial ischemia (13,14).
MATERIALS AND METHODS
Patients
This retrospective analysis was approved by our institutional review board; patient consent was not required. Between March 2004 and December 2009, approximately 45,600 patients underwent 18F-FDG/CT and approximately 6,800 patients underwent exercise stress testing and MPI in our center. We identified 93 patients who underwent 18F FDG PET/CT within 8 h (n = 48, Ex 8) or 48 h (n = 45, Ex 48) of treadmill testing. Another 34 patients, who also underwent 18F-FDG PET/CT but without a preceding exercise test, were randomly selected to serve as controls (No Ex). Indications for PET included cancer staging, detection of recurrence, and response assessment. MPI studies were performed to detect ischemia or infarction because of symptoms suggestive of active coronary artery disease and heart failure of uncertain etiology or for presurgical risk assessment.
Data Acquisition
All patients fasted for at least 4 h before MPI. 201Tl-chloride (148 MBq [4 mCi]) or 99mTc-tetrofosmin (370 MBq [10 mCi]) was used for the rest study. Treadmill exercise was performed using the Bruce or modified Bruce protocol. At peak exercise, 1,110 MBq (30 mCi) of 99mTc-tetrofosmin were injected through an indwelling venous catheter, and the patient was encouraged to continue exercising for an additional 2 min. Gated SPECT images were obtained at rest and 44 ± 23 min after stress using a dual-head γ-camera (Forte; ADAC). All patients fasted for at least 6 h before 18F-FDG PET/CT. Patients who underwent MPI in the morning hours continued to fast until the PET/CT study. Blood glucose was less than 200 mg/dL in all patients. After an approximately 60- to 90-min uptake period, images were obtained on standard clinical PET/CT scanners for 3–5 min per bed position.
Data Analysis
MPI data were reviewed using the Cedar's Sinai software package on a workstation (Hermes). Location, size, and severity of perfusion defects were recorded. PET/CT was reviewed on a PACS workstation (AW Extension; GE Healthcare). The overall PET image quality was determined using skeletal muscle uptake as a reference: grade 1 (< mediastinal blood pool), 2 (> blood pool but < liver), 3 (equal to liver), or 4 (> liver uptake). Maximum standardized uptake value (SUVmax) and average standardized uptake value (SUVmean) (using a 42% threshold) were measured within volumetric regions of interest placed bilaterally on the gluteal and quadriceps muscles and on the liver and lumbar spine. In the single patient who was imaged below the mid thigh, SUVs for calf muscles were recorded. The pattern of 18F-FDG uptake in the myocardium was described as focal, diffuse, or absent.
Statistical Analysis
Patient characteristics were compared across the 3 groups using the Kruskal–Wallis test for continuous variables and a χ2 test for categoric variables. SUVmax and average SUV were compared across the groups using the Kruskal–Wallis test, separately for quadriceps, gluteal muscles, liver, and lumbar spine. The association involving the time interval between the treadmill test and the PET scan with 18F-FDG uptake was also evaluated by the Kruskal–Wallis test. P values less than 0.05 were considered significant.
RESULTS
Patient Characteristics
There were no differences with regard to age, sex, injected activity, uptake times, or blood glucose levels (Table 1). In Ex 8, 5 of 48 patients were diabetic (1 insulin-dependent); in Ex 48, 2 of 45 patients were diabetic (1 insulin-dependent); and in No Ex, 2 of 34 patients were diabetic (none insulin-dependent). Among patients undergoing treadmill exercise before PET/CT, the exercise capacity was similar (duration, hemodynamics, and metabolic equivalents [METS]; Table 1).
Patient Characteristics and Exercise Performance
Image Quality and Skeletal Muscle Uptake
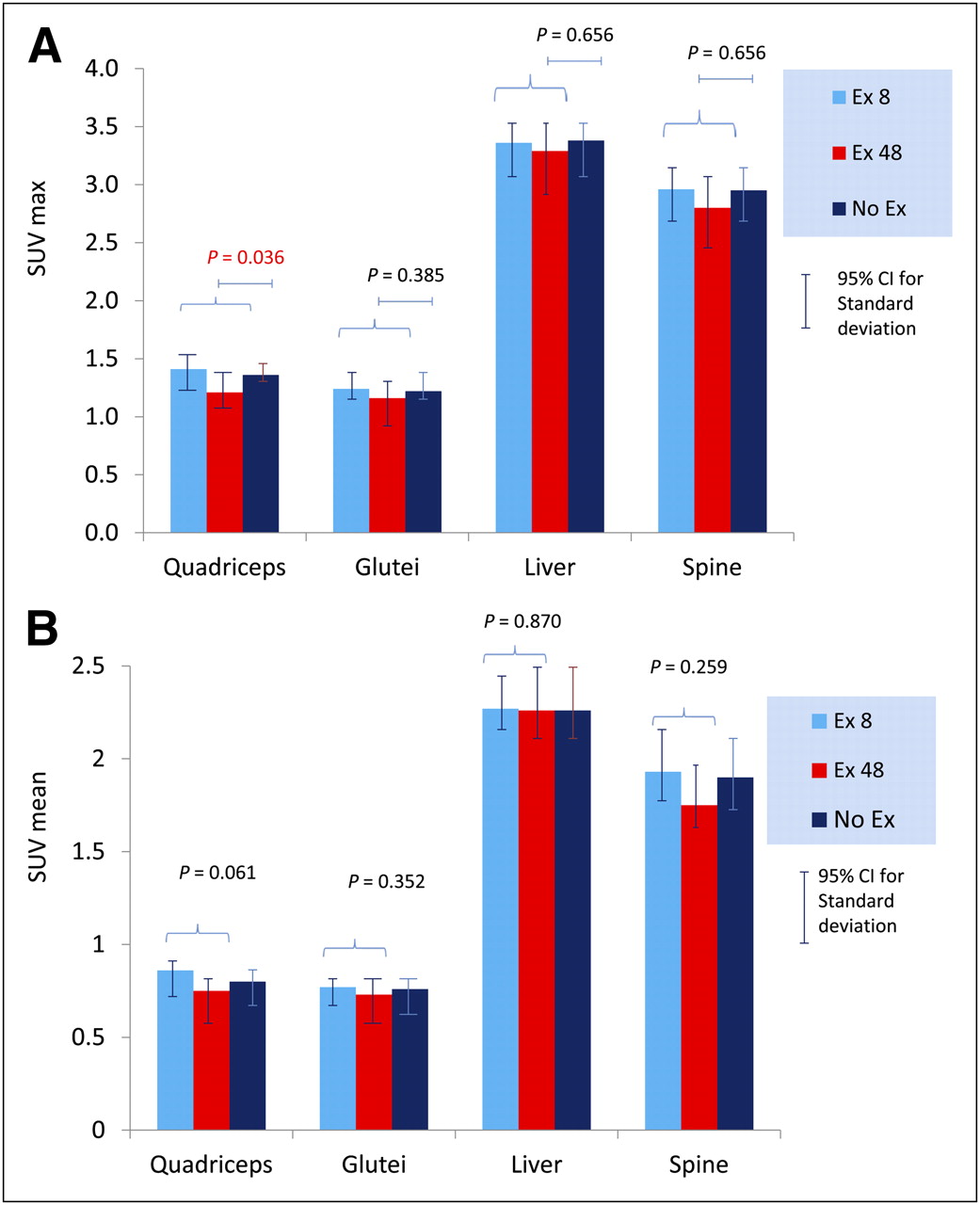
Overall, PET images were graded as 1 in 47 of the 48 Ex 8 patients and in all Ex 48 patients. There were no cases in Ex 8 or Ex 48 with muscle uptake conspicuously greater than muscle uptake in No Ex. SUVs for liver and lumbar spine were similar for all patient groups. SUV in quadriceps and gluteal muscles were slightly higher in No Ex than in Ex 48 but slightly lower than in Ex 8. The only difference was a slightly higher SUVmax in quadriceps muscles in Ex 8 versus Ex 48 (P = 0.036, Fig. 1). SUVmax in No Ex did not differ from that in Ex 8 and Ex 48. In Ex 8 and Ex 48, there was no correlation between muscle 18F-FDG uptake and duration of exercise (P = 0.835), metabolic equivalents achieved (P = 0.417), or the maximum rate–pressure product (P = 0.081). In subgroup analysis, Ex 8 patients who achieved greater than the median number of METS tended to show a higher SUVmax in quadriceps muscles (1.46 ± 0.40 vs. 1.03 ± 0.42, P = 0.058). The time interval between completion of exercise and PET scanning did not affect the 18F-FDG uptake in muscle groups.

SUVmax (A) and average SUV (B) in muscle groups and liver and spine background regions in 3 patient groups. CI = confidence interval.
MPI Findings and Myocardial 18F-FDG Uptake
MPI findings were abnormal in 16 of the 93 patients in Ex 8 and Ex 48. Fixed lesions were seen in 5 subjects and mild or moderate ischemia in 11 patients (Table 2). Myocardial 18F-FDG uptake in these 93 patients was quite variable: diffuse (n = 22), focal (n = 29), or absent (n = 42). In No Ex controls, 15 patients had diffuse myocardial uptake, 9 focal uptake, and 10 no uptake. In Ex 8 and Ex 48, there was no clear correlation between MPI perfusion defects and patterns of myocardial 18F-FDG uptake (Supplemental Table 1 [supplemental materials are available online only at http://jnm.snmjournals.org]; Figs. 2 and 3).
Patients with Ischemia on MPI
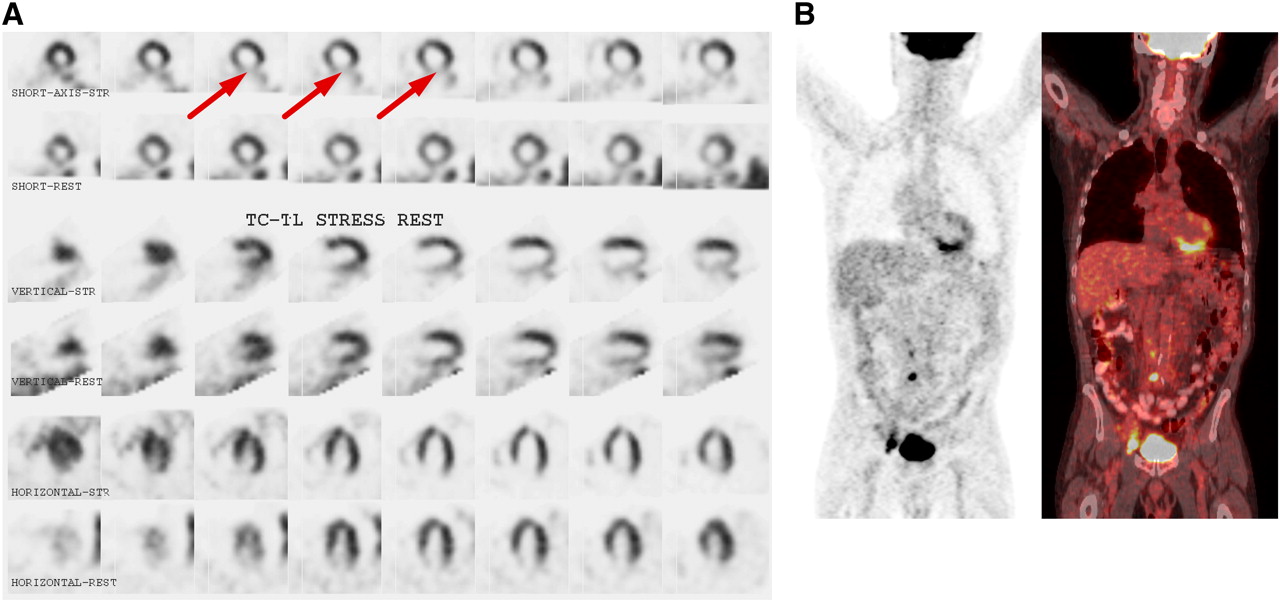
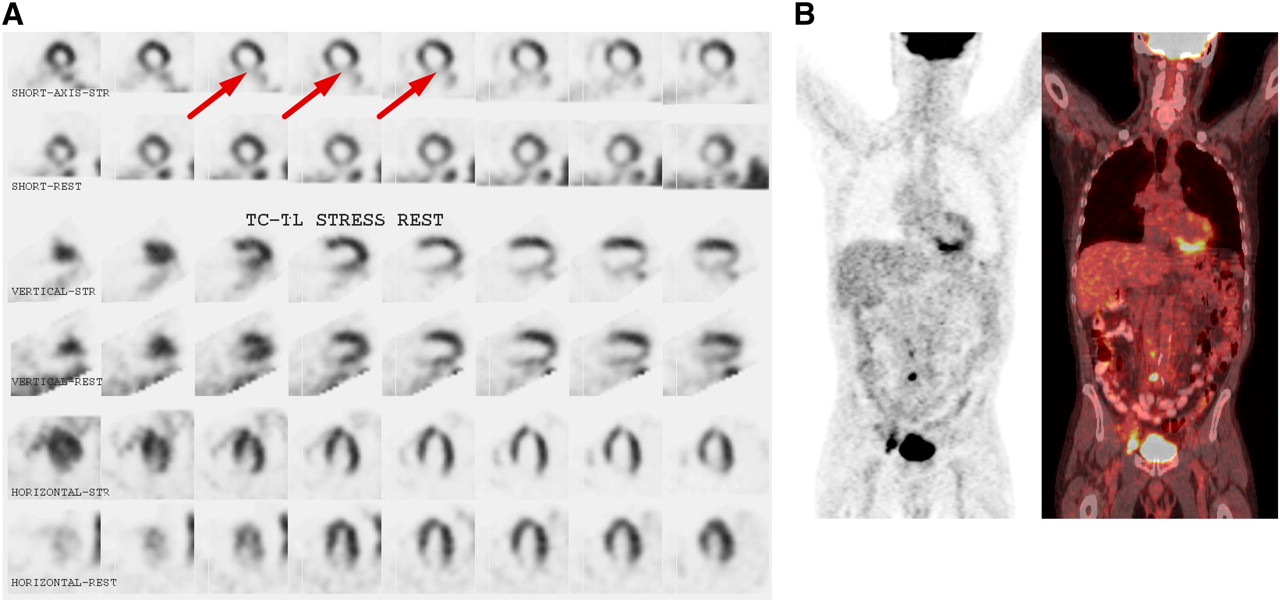
Concordant perfusion defect on MPI and 18F-FDG uptake in 68-y-old man with esophageal cancer and lymphoma. Patient achieved 6.6 METS on treadmill test. MPI (A) shows large area of moderate ischemia in inferior wall and apex. Coronal PET and fused PET/CT (B) done 24 h and 23 min later, with 83-min uptake time, shows tracer uptake in inferior wall.
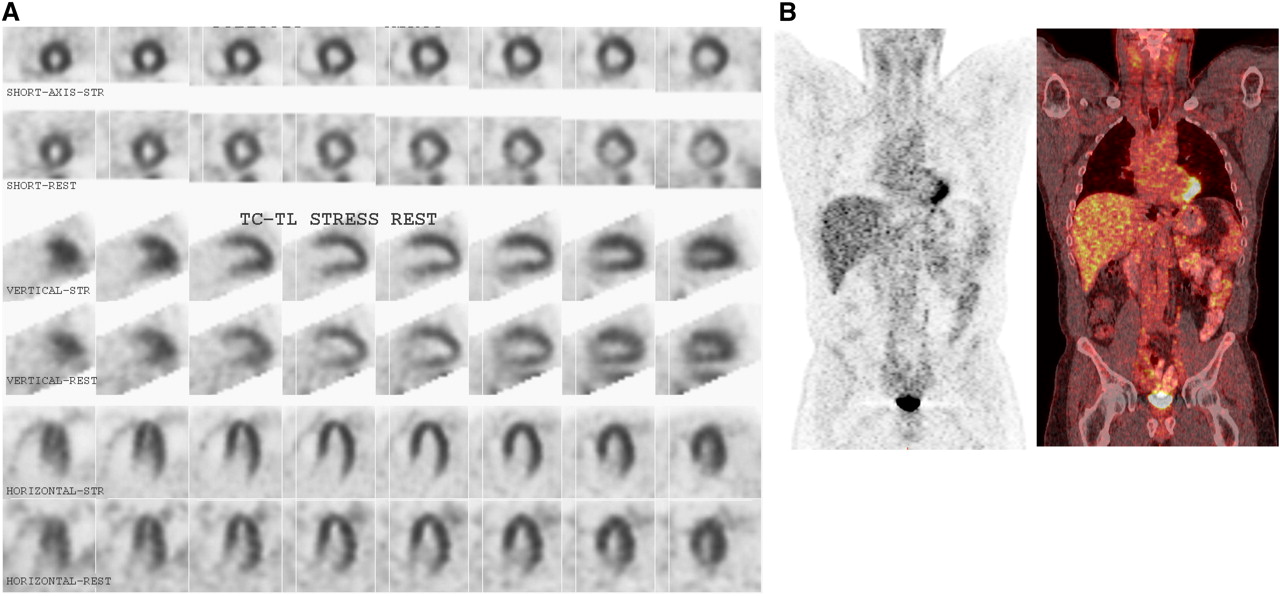
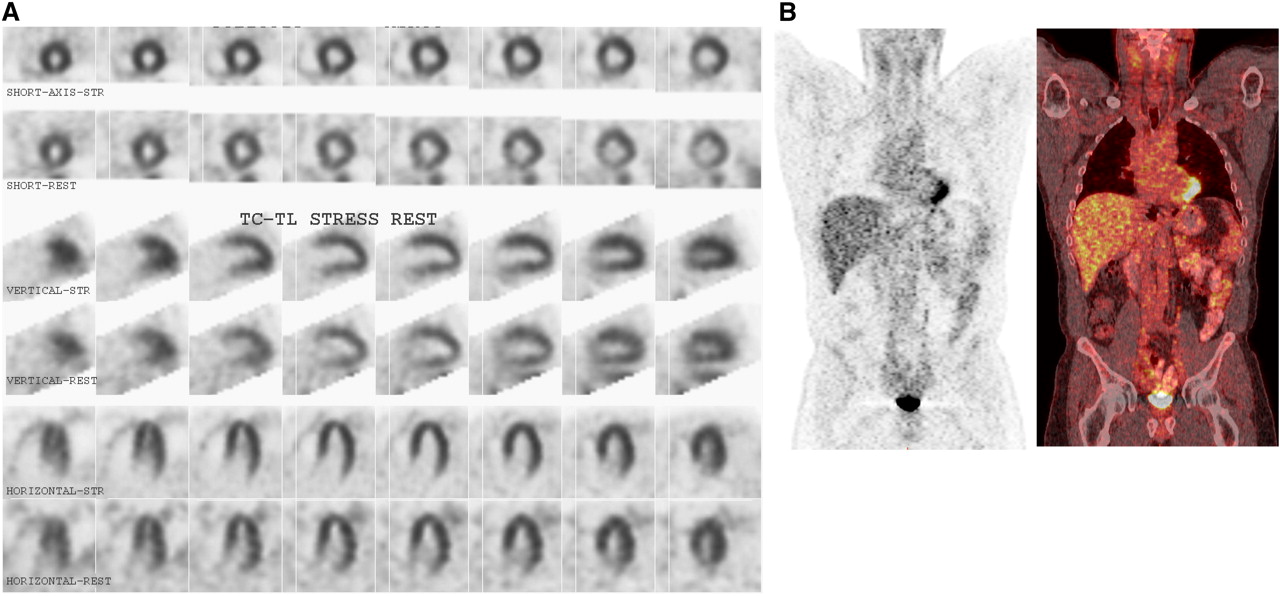
Discordant findings on MPI and 18F-FDG PET/CT in 52-y-old man with right lower lobe lung cancer. Patient achieved 12.3 METS on treadmill test. MPI (A) shows normal perfusion. Coronal PET and fused PET/CT (B) done 29 h and 19 min later, with 66-min uptake time, shows focal tracer uptake in apex.
DISCUSSION
Theoretically, increased 18F-FDG uptake in skeletal muscle may reduce the amount of radiotracer available for tumor uptake. Exercise-induced 18F-FDG uptake in skeletal muscles has been studied (9,10,15). With treadmill exercise, 18F-FDG uptake increases in the soleus, gastrocnemius, gluteal, and quadriceps muscles, followed by adductors and hamstring muscles. Fifteen to 50 min of level walking increases 18F-FDG uptake in calf muscles and gluteus minimus muscles (10,15) by about a factor of 2. Guidelines recommend that patients refrain from exercise in the hours preceding 18F-FDG PET. Because of scheduling conflicts or errors, we encountered patients (1.4% of all MPI patients and 0.2% of all PET patients during the study period) who underwent exercise testing within less than 48 h of PET. Contrary to our expectation, we did not find any effect of treadmill exercise on muscle 18F-FDG uptake.
How can these data be reconciled? First, the duration of exercise stress testing in our patients was relatively short and the intensity relatively low. By comparison, studies in healthy volunteers involved much more demanding regimens (6,9,15,16). Although our patients achieved a reasonable work load, the exercise capacity in a predominantly elderly group of oncology patients is probably lower than that of healthy (and mostly younger) volunteers in applied physiology protocols. A general catabolic state or the frailty of older age may also have altered exercise-induced muscle glucose flux. Finally, our patients had fasted for at least 6 h before 18F-FDG injection, and thus plasma insulin concentrations are expected to be low. Our data suggest that some recommendations for patient preparation, including one that specifically discourages patients from commuting by bicycle to the imaging center (12), may be overly conservative.
Some clinical reports suggested that cardiac 18F-FDG uptake is a sensitive marker of acute and prolonged myocardial ischemia (13,14). This finding contrasts with clinical observations that the pattern of myocardial 18F-FDG uptake varies widely (17). We therefore investigated the relationship between perfusion defects on MPI and myocardial 18F-FDG uptake on a subsequent PET scan. Indeed, experimental studies show persistent increased myocardial glucose metabolism after acute, chronic, or repetitive ischemia (18,19). In this setting, glucose is probably predominantly used for glycolysis (rather than glucose oxidation or glycogen synthesis), and glycolytically derived adenosine triphosphate appears essential for cellular homeostasis (20). Clinical studies used simultaneous injection of 99mTc-sestamibi and 18F-FDG during peak stress (13,14). One study for 26 patients reported perfusion defects in 22 of 51 territories supplied by stenotic vessels (>50% luminal narrowing) and increased 18F-FDG uptake in 34 of 51 territories (14). In contrast to these studies, our patients were injected with 18F-FDG several hours after stress testing, and we found no correlation between areas of ischemia on MPI and myocardial 18F-FDG uptake. Although only few patients showed ischemia on MPI, the number of patients with focal 18F-FDG uptake (n = 29) far exceeded the number of patients with ischemia on MPI (n = 11). Moreover, 9 of 34 patients in our No Ex control group also showed focal myocardial 18F-FDG uptake. Thus, in daily practice patterns of cardiac 18F-FDG uptake vary widely and should not be used as a surrogate for myocardial perfusion status.
CONCLUSION
Contrary to widespread belief, 18F-FDG PET can be performed on the same day as a treadmill exercise test and MPI without deterioration of PET image quality. Prospective studies are needed to better define the frequency, magnitude, quantitative relationship, and clinical significance (if any) between mild to moderate myocardial ischemia and cardiac 18F-FDG uptake patterns noticeable on PET.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online May 14, 2012.
- © 2012 by the Society of Nuclear Medicine, Inc.
REFERENCES
- Received for publication January 25, 2012.
- Accepted for publication February 6, 2012.




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.