


Article Figures & Data
Figures
- FIGURE 1.
Receiver-operating-characteristic analysis using cardiac metaiodobenzylguanidine activity (late HMR) and tetrofosmin SS for identification of patients with primary cardiac event. Metaiodobenzylguanidine HMR of 1.90 and tetrofosmin SS of 12 were selected as optimal cutoff values. TF = tetrofosmin.
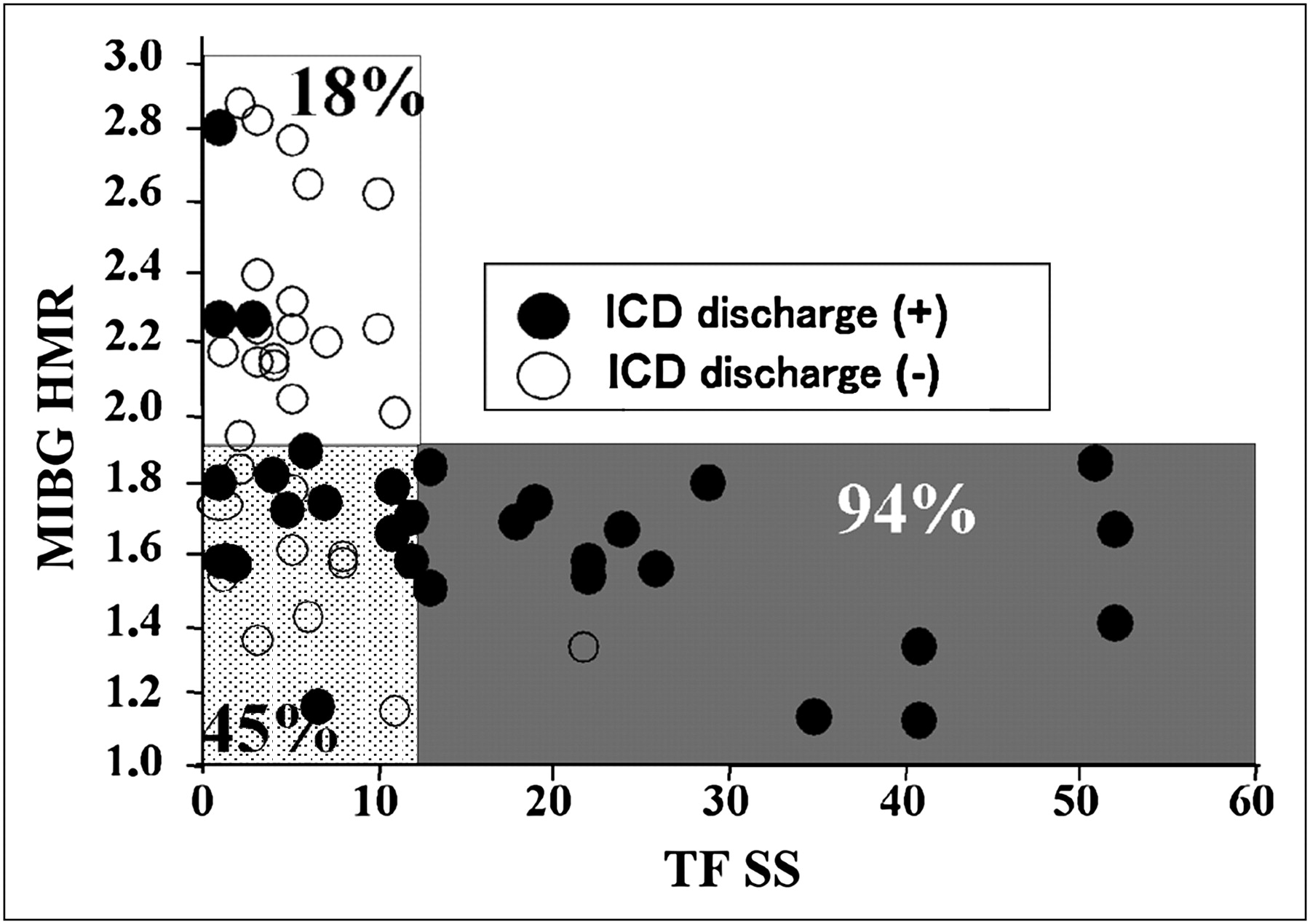
- FIGURE 2.
Scatterplots of patients with (●) and without (○) primary cardiac events who were divided into 3 groups based on cutoff vales of cardiac metaiodobenzylguanidine activity and tetrofosmin uptake identified by receiver-operating-characteristic analysis. There are significant (P < 0.05) differences in event rate among the 3 groups (94% for group with impaired metaiodobenzylguanidine and tetrofosmin uptake, 45% for group with impaired metaiodobenzylguanidine and preserved tetrofosmin uptake, and 18% for group with preserved metaiodobenzylguanidine and tetrofosmin uptake). Unshaded area = preserved uptake of both metaiodobenzylguanidine and tetrofosmin (n = 22); dotted area = impaired metaiodobenzylguanidine uptake and preserved tetrofosmin uptake (n = 20); shaded area = impaired uptake of both metaiodobenzylguanidine and tetrofosmin (n = 18). MIBG = metaiodobenzylguanidine; TF = tetrofosmin.
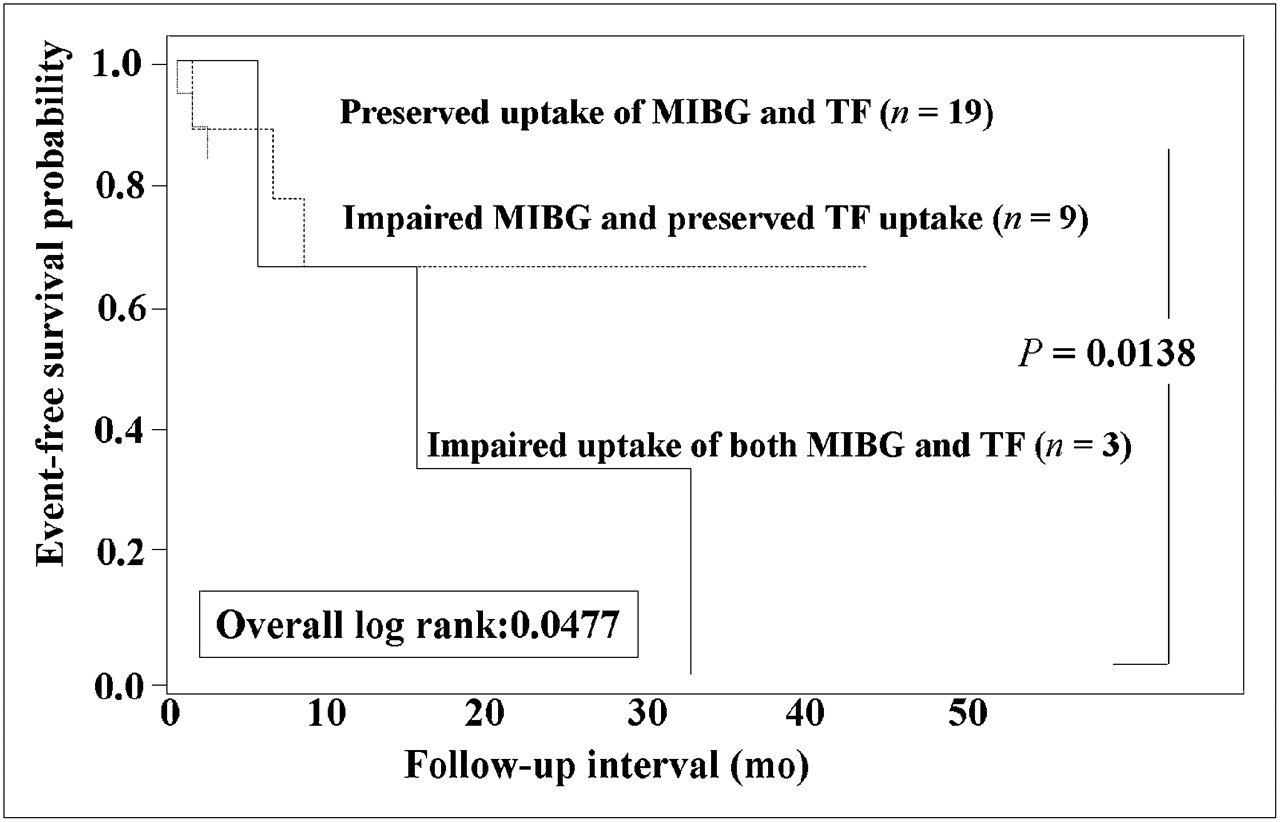
- FIGURE 3.
Kaplan–Meier event-free curves of 3 groups based on metaiodobenzylguanidine and tetrofosmin uptake show that patients with impaired uptake of both metaiodobenzylguanidine and tetrofosmin had significantly lower event-free rate than did patients in the other 2 groups. MIBG = metaiodobenzylguanidine; TF = tetrofosmin.
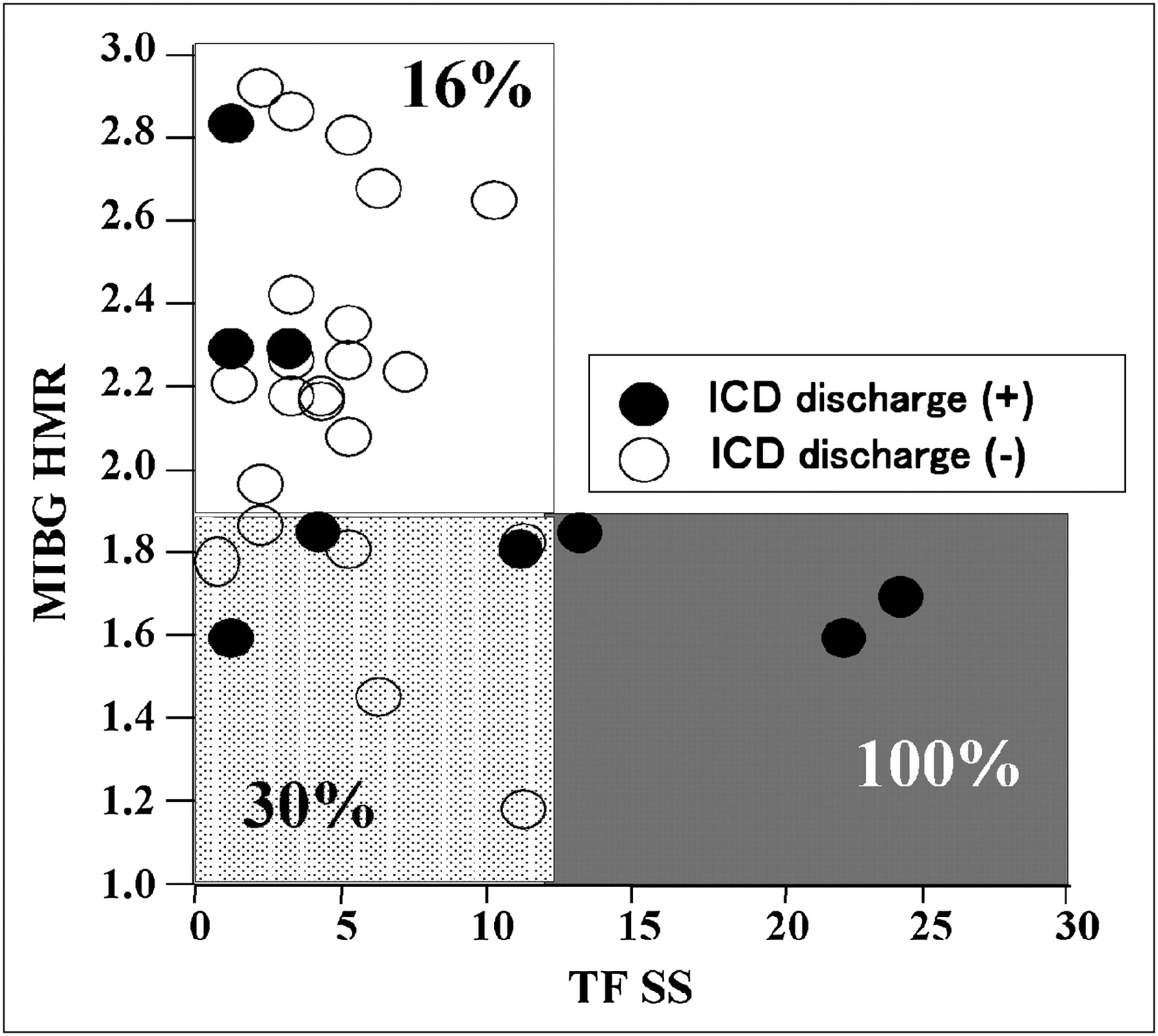
- FIGURE 4.
Scatterplots of patients with (●) and without (○) primary cardiac events when 31 patients with LVEF of 50% or more are considered. Patient group with impaired uptake of both metaiodobenzylguanidine and tetrofosmin had greatest (P < 0.05) event rate (100%) when compared with other groups (16%–30%). Unshaded area = preserved uptake of both metaiodobenzylguanidine and tetrofosmin (n = 19); dotted area = impaired metaiodobenzylguanidine uptake and preserved tetrofosmin uptake (n = 9); shaded area = impaired uptake of both metaiodobenzylguanidine and tetrofosmin (n = 3). MIBG = metaiodobenzylguanidine; TF = tetrofosmin.
- FIGURE 5.
Kaplan–Meier event-free curves of 3 groups based on metaiodobenzylguanidine and tetrofosmin uptake when 31 patients with LVEF of 50% or more are considered. Patients with impaired uptake of both metaiodobenzylguanidine and tetrofosmin had significantly lower event-free rate than did group with preserved uptake of both metaiodobenzylguanidine and tetrofosmin. MIBG = metaiodobenzylguanidine; TF = tetrofosmin.
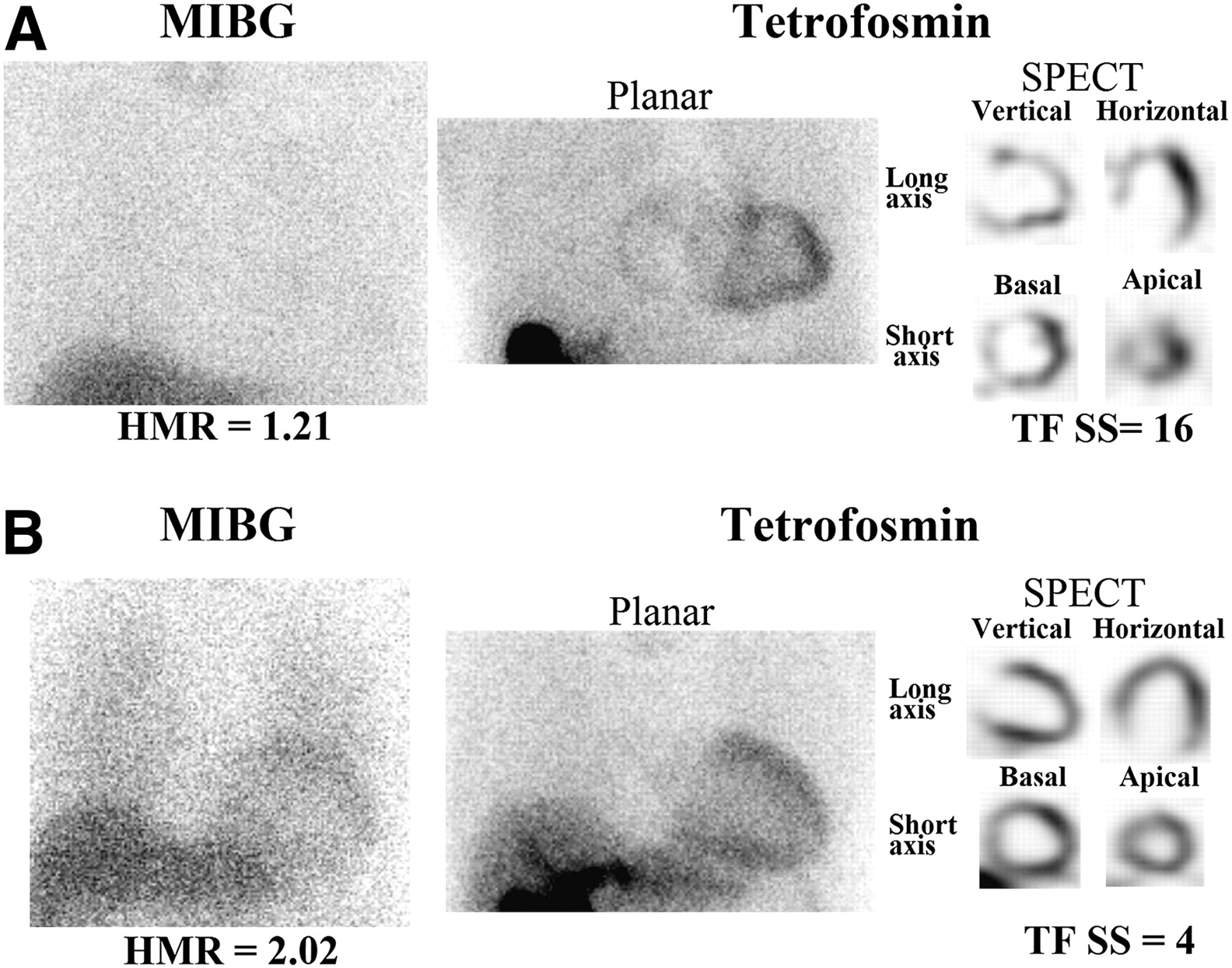
- FIGURE 6.
Planar metaiodobenzylguanidine images and planar and tomographic tetrofosmin images. (A) A 56-y-old woman had both markedly reduced metaiodobenzylguanidine activity (HMR of 1.21) and perfusion uptake (tetrofosmin SPECT SS of 16) and underwent ICD shocks 3 mo after implantation because of electrical storm of ventricular tachyarrhythmia. (B) A 60-y-old man had highly dilated left ventricle but nearly normal cardiac metaiodobenzylguanidine activity (HMR of 2.02) and perfusion score (tetrofosmin SS of 4). Neither ICD shock nor other lethal cardiac event was observed during follow-up. MIBG = metaiodobenzylguanidine; TF = tetrofosmin.




Tables
- TABLE 1.
Comparison of Clinical Backgrounds Between Patients With and Without Primary Endpoints
Parameter Patients with cardiac events (n = 30) Patients without cardiac events (n = 30) P Mean age ± SD (y) 53.3 ± 15.0 53.4 ± 12.1 NS Sex (female) 8 (27) 11 (37) NS Coronary risk factors Diabetes mellitus 8 (27) 4 (13) NS Hypertension 7 (23) 8 (27) NS Dyslipidemia 14 (47) 7 (23) NS Chronic renal failure 2 (7) 3 (10) NS Underlying cardiac disease Prior myocardial infarction 8 (27) 3 (10) Dilated cardiomyopathy 15 (50) 7 (23) Hypertrophic cardiomyopathy 2 (7) 5 (17) NS Arrhythmogenic right ventricular dysplasia 2 (7) 4 (13) Brugada syndrome 1 (3) 9 (30) Idiopathic ventricular arrhythmia 2 (7) 2 (7) NYHA functional class NS I 15 25 II 0 3 III 14 0 IV 1 2 Mean follow-up period ± SD (mo) 31 ± 17 28 ± 15 NS ECG (mean ± SD) LVEF (%) 42 ± 18 56 ± 15 0.002 Left ventricular end-diastolic diameter (mm) 57 ± 11 50 ± 11 0.017 BNP (pg/mL) 209 ± 198 101 ± 140 0.018 Presenting arrhythmia before ICD implantation VF 6 (20) 7 (23) NS Sustained VT 18 (60) 8 (27) 0.02 Nonsustained VT 6 (20) 5 (17) NS Electrophysiologic study Inducible VT 17 (57) 12 (40) NS Inducible VF 16 (53) 10 (33) NS Concomitant medication Diuretic 14 (47) 6 (20) NS Spironolactone 15 (50) 4 (13) 0.005 Digitalis 3 (10) 0 (0) NS β-blocker 22 (73) 11 (37) 0.011 ACEI/ARB 19 (63) 9 (30) 0.02 Nitrate 6 (20) 1 (3) NS NS= not significant; NYHA = New York Heart Association; VF = ventricular fibrillation; VT = ventricular tachyarrhythmias; ACEI = angiotensin converting enzyme inhibitor; ARB = angiotensin II receptor blocker.
Data in parentheses are percentages.
- TABLE 2.
Comparison of Scintigraphic Data Between Patients With and Without Primary Endpoints
Parameter Patients with cardiac events (n = 30) Patients without cardiac events (n = 30) P Metaiodobenzylguanidine Early HMR 1.96 ± 0.26 2.16 ± 0.37 0.019 Late HMR 1.73 ± 0.34 2.06 ± 0.46 0.003 Washout rate 33.1 ± 14.0 28.6 ± 11.0 NS Tetrofosmin SS 18.0 ± 16.2 5.7 ± 4.4 0.000 LVEF 36 ± 19 54 ± 13 0.000 LVEDV 187 ± 117 109 ± 87 0.005 LVESV 157 ± 121 75 ± 74 0.002 NS = not significant; LVEDV = left ventricular end-diastolic volume; LVESV = left ventricular end-systolic volume.
Values are shown as mean ± SD.
Univariate Multivariate (Cox proportional hazards model) 95% Confidence interval 95% Confidence interval Parameter Wald Hazard ratio Lower Upper P Wald Hazard ratio Lower Upper P Age (y) 0.050 0.997 0.969 1.026 0.824 Sex 0.908 1.489 0.657 3.376 0.341 Clinical VT/VF 3.992 4.34 1.028 18.313 0.046 Inducible VT/VF 0.210 0.839 0.396 1.779 0.647 SAECG 0.574 1.492 0.530 4.198 0.449 Medications 1.615 1.629 0.767 3.459 0.204 BNP 4.579 1.002 1.000 1.004 0.032 0.655 1.001 0.998 1.004 0.418 HMR (late) 7.771 0.205 0.067 0.625 0.005 Washout 0.663 1.014 0.981 1.047 0.415 HMR ≦ 1.9 8.509 5.966 1.797 19.806 0.004 3.705 4.560 0.973 21.374 0.054 Tetrofosmin SS 13.547 1.043 1.020 1.067 0.000 Tetrofosmin SS ≧ 12 13.691 4.022 1.924 8.408 0.000 4.083 2.842 1.032 7.830 0.043 HMR ≦ 1.9 and tetrofosmin SS ≧ 12 13.691 4.022 1.924 8.408 0.000 6.454 3.857 1.361 10.928 0.011 LVEF 4.188 0.978 0.958 0.999 0.041 0.890 0.346 0.983 1.051 0.346 VT = ventricular tachycardia; VF = ventricular fibrillation; SAECG = signal-averaged electrocardiographic findings.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Sympathetic structural and electrophysiological remodeling in a rabbit model of reperfused myocardial infarction
- Chondroitin Sulfate Proteoglycan 4,6 sulfation regulates sympathetic nerve regeneration after myocardial infarction
- Nuclear Imaging of the Cardiac Sympathetic Nervous System: A Disease-Specific Interpretation in Heart Failure
- Molecular Mechanisms of Sympathetic Remodeling and Arrhythmias
- The Nervous Heart: Role of Sympathetic Reinnervation in Cardiac Regeneration
- Predicting Risk Versus Predicting Potential Survival Benefit Using 123I-mIBG Imaging in Patients With Systolic Dysfunction Eligible for Implantable Cardiac Defibrillator Implantation: Analysis of Data From the Prospective ADMIRE-HF Study
- Introduction to Cardiac Neuronal Imaging: A Clinical Perspective
- Cardiac 123I-MIBG Imaging for Clinical Decision Making: 22-Year Experience in Japan
- A Pooled Analysis of Multicenter Cohort Studies of 123I-mIBG Imaging of Sympathetic Innervation for Assessment of Long-Term Prognosis in Heart Failure
- Infarct-Derived Chondroitin Sulfate Proteoglycans Prevent Sympathetic Reinnervation after Cardiac Ischemia-Reperfusion Injury
- Cardiac iodine-123 metaiodobenzylguanidine imaging predicts ventricular arrhythmia in heart failure patients receiving an implantable cardioverter-defibrillator for primary prevention
- Cardiac Mortality Assessment Improved by Evaluation of Cardiac Sympathetic Nerve Activity in Combination with Hemoglobin and Kidney Function in Chronic Heart Failure Patients
- 123I-Metaiodobenzylguanidine Imaging in the Era of Implantable Cardioverter Defibrillators: Beyond Ejection Fraction