


Abstract
Our objective was to investigate the use of bowel preparation before 18F-FDG PET/CT to reduce intestinal 18F-FDG uptake. Methods: Sixty-five patients with abdominal neoplasias were assigned either to a bowel-preparation group (n = 26) or to a native group (n = 39). 18F-FDG activity was measured in the small intestine and the colon. Results: In the 26 patients with bowel preparation, average maximal standardized uptake value (SUVmax) was 3.5 in the small intestine and 4.4 in the colon. In the 39 patients without bowel preparation, average SUVmax was 2.6 in the small intestine and 2.7 in the colon. 18F-FDG activity impaired diagnosis in 6 patients (23%) in the bowel-preparation group and 11 patients (28%) in the native group (P = 0.5). SUVmax in the colon was significantly higher in the bowel-preparation group (P = 0.002), but SUVmax in the small intestine did not significantly differ between the 2 groups (P = 0.088). Conclusion: Bowel preparation increases 18F-FDG activity in the large intestine and is therefore not useful before PET/CT.
In the daily clinical routine of reading 18F-FDG PET/CT scans, physiologic intestinal uptake of the tracer is frequently observed (1). In general, such tracer accumulation is only faint or moderate and diffuse. Such a pattern is usually easy to identify as nonpathologic, especially if morphologic abnormalities are absent (2). However, there are still a considerable number of patients with a higher and more focal accumulation of 18F-FDG in the intestine. Such physiologic 18F-FDG uptake in the bowel can lead to misinterpretation, unnecessary interventions, or inaccurate treatment decisions. Many patients will be referred for colonoscopy, which generates additional costs and causes discomfort to the patients (3,4). In the literature, recommendations have been made in order to reduce physiologic uptake of 18F-FDG in the intestine or to improve the ability to evaluate intestinal structures (5–8). However, no published study has proven that bowel preparation before PET/CT is beneficial. We therefore conducted a naturally randomized and single-blinded study to evaluate the effects of bowel cleansing on intestinal 18F-FDG activity in PET/CT.
MATERIALS AND METHODS
This prospective, naturally randomized, and single-blinded study was approved by our local ethics committee. Between August 2007 and June 2008, 65 patients with primary abdominal malignancies were included. All patients had been referred to our institution for oncologic PET/CT. Before the examination, they received study information together with a prescription for a senna-glycoside solution (X-Prep [Mundipharma], 75 mL). Only those patients with a gap of at least 3 working days between referral and scheduling could be included. No further selection criteria were used. Patients willing to perform the bowel-cleansing procedure were assigned to the bowel-preparation group. Patients who preferred not to do so were assigned to the native group. Written informed consent was obtained from all patients before the procedure.
Preparations
Patients in the bowel-preparation group had to drink 75 mL of the senna-glycoside solution together with 2 L of tap water by 2 pm the day before the PET/CT examination. After ingestion of the solution, no more solid meals were allowed. Complete fasting was necessary for at least 4 h before the scheduled examination. Patients in the native group had to fast for at least 4 h before the examination as part of our routine procedure. No oral contrast agent was administered to either of the groups.
PET/CT
PET/CT was performed as a clinical procedure according to the routine parameters used at our institution (9).
Image Evaluation and SUVmax Measurements
Images were evaluated on commercially available Advantage workstations (version 4.4; GE Healthcare) by 2 physicians board-certified in both radiology and nuclear medicine, reading by consensus. The readers were unaware of the group assignment and history of the patients. The purge was qualitatively assessed by determining whether intraluminal stool was visible in the 4 portions of the colon (ascending, transverse, descending, and sigmoid/rectum). An additional quantitative assessment was performed by measuring the maximal diameters of the 4 portions of the colon. Maximal standardized uptake values (SUVmax) were obtained from the small intestine as a whole and from the different parts of the colon by creating a volume of interest over the region with the visually highest tracer activity. No differentiation was made between bowel wall and lumen. Additionally, a 4-step scoring system for the areas with the highest 18F-FDG activity in the small intestine and colon was applied. The scoring system used the liver and brain as reference sites (Table 1). Finally, the influence of intestinal 18F-FDG accumulation on diagnostic image quality was evaluated. Any focal 18F-FDG accumulation within the colon was regarded as a factor leading to diagnostic uncertainty. Thus, diagnostic impairment was postulated for those patients. Diffuse 18F-FDG accumulations were not considered suggestive of malignancy. Therefore, no diagnostic impairment was postulated.
Four-Step Scoring System for Areas with Highest Activity, Using Liver and Brain as Reference Sites
Statistical Analysis
Statistical analysis was performed using the Mann–Whitney and Pearson χ2 tests. A P value of less than 0.05 was considered to indicate statistical significance.
RESULTS
Patient and Disease Characteristics
All patients had primary abdominal malignancies. Fifty-one patients had a history of colorectal carcinoma (78%), 11 had gynecologic malignant disease (17%), 2 had gastric carcinoma (3%), and 1 had pancreatic cancer (2%). Twelve patients were scanned for primary staging, and 53 were examined for follow-up or because of suspected recurrence. Most patients had advanced disease, stage III or IV (n = 45). Seven patients had received no treatment before PET/CT; the others had undergone surgery (n = 16) or had received chemotherapy (n = 2) or multimodal therapy (n = 40). The average interval between the last therapy and PET/CT was 11 mo in the bowel-preparation group and 13 mo in the native group. Statistical analysis showed no significant difference between the 2 groups regarding sex (P = 1), age (P = 0.874), tumor entity (P = 0.598), tumor stage (P = 0.871), reason for examination (primary staging, follow-up, or recurrence) (P = 0.836), previous treatment (P = 0.262), or interval between last treatment and PET/CT (P = 0.872).
Native Versus Bowel-Preparation Groups
Twenty-six patients were included in the bowel-preparation group and 39 in the native group. In the bowel-preparation group, 2 patients had undergone previous resection of the sigmoid/rectum. In the native group, 4 patients had undergone previous resection of the ascending colon, 1 of the transverse colon, and 1 of the descending colon. The assessment of purge efficiency showed that significantly more patients in the native group had visible stool in all colonic segments (Table 2). Except for the descending colon, the average diameters of each colonic segment were also significantly larger in the native group (Table 3). These findings proved the efficiency of the cleansing procedure.
Segmental Analysis of Stool Content in Colon
Segmental Analysis of Average Colon Diameter
SUVmax was higher in the bowel-preparation group than in the native group for small intestine and colon. The Mann–Whitney test showed that the difference in the small intestine was not significant (P = 0.088). In the colon, however, the difference was highly significant in all colonic segments except the sigmoid/rectum (Table 4). In the bowel-preparation group, most patients had the highest SUVmax in the ascending colon (15/26), followed by the sigmoid/rectum (8/26). In the native group, most patients had the highest SUVmax in the sigmoid/rectum (19/39), followed by the ascending colon (13/39).
Segmental and Overall Analysis of SUVmax Measured in Small Intestine and Colon
The visual score analysis corresponded to the SUVmax measurements, with higher scores in the bowel-preparation group. Pearson χ2 testing showed no significant difference in the small intestine (P = 0.685) and a highly significant difference in the colon (P < 0.001) (Table 5).
Visual Score Analysis of Area with Highest 18F-FDG Uptake in Small Intestine and Colon
The comparison of diagnostic impairment from intestinal 18F-FDG accumulation showed slightly increased total impairment in the native group. Six patients (23%) in the bowel-preparation group and 11 (28%) in the native group had focal 18F-FDG accumulation in the colon (Fig. 1). One patient in the native group had 3 colonic segments with focal 18F-FDG activity. The Mann–Whitney test showed no statistically significant difference between the groups (P = 0.5).
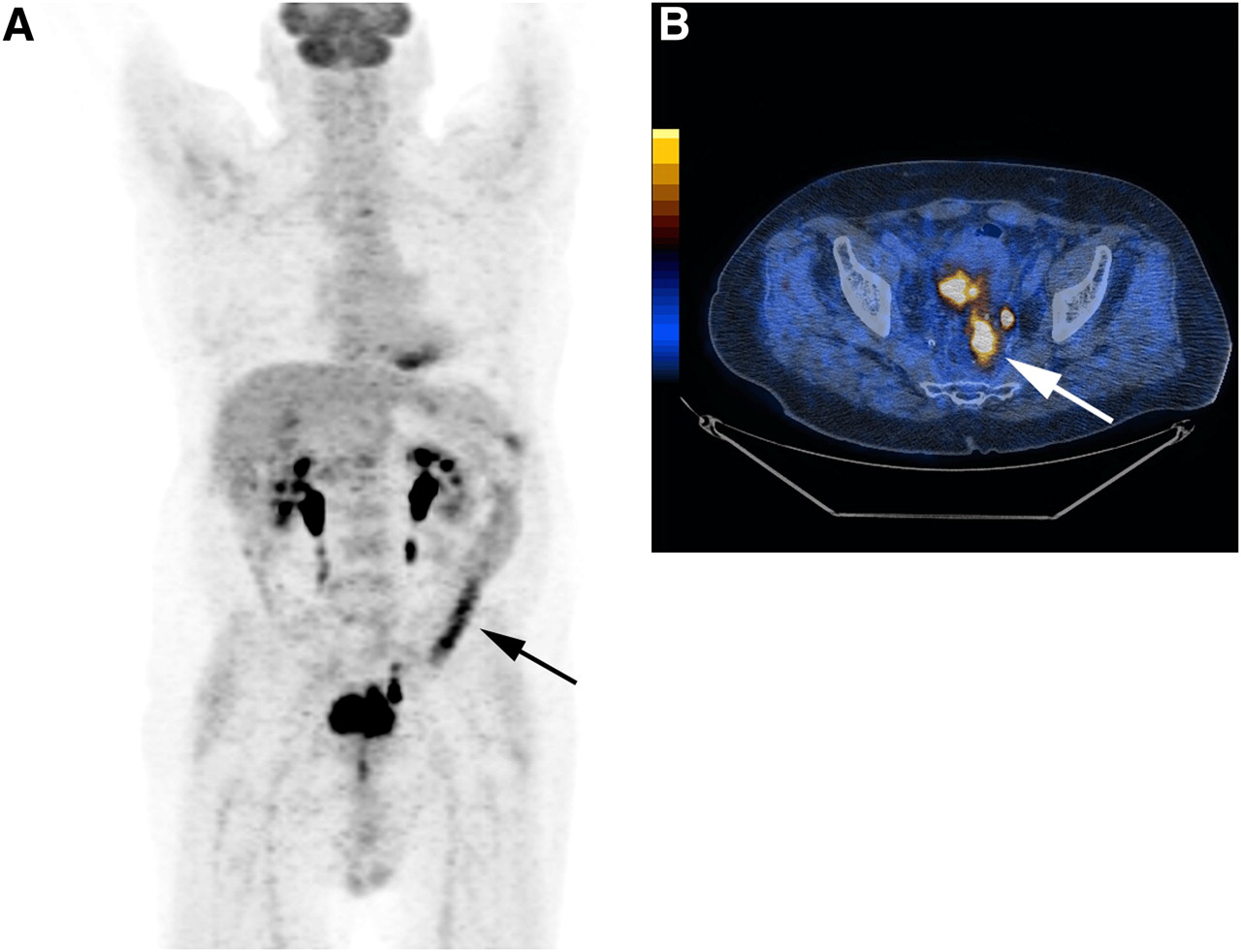
A 72-y-old man from bowel-preparation group with rectal carcinoma and suspected recurrence. Patient initially had stage III disease, diagnosed and treated 7 y before imaging with resection of primary tumor and adjuvant radiochemotherapy. Images show intense 18F-FDG accumulation in colon (SUVmax, 9.4), with diffuse activity in descending colon (arrow in A) and focal activity in rectum (arrow in B). Despite bowel cleansing, diagnostic uncertainty regarding local recurrence in rectum remained.
DISCUSSION
The need to differentiate between physiologic and pathologic intestinal 18F-FDG uptake has been discussed since the very beginnings of PET, and suggestions on patient preparation (including bowel cleansing) have been made (6–8). To our knowledge, ours has been the first prospective, naturally randomized study to investigate the value of bowel preparation with a purging agent before PET/CT. Our findings—significantly higher 18F-FDG activity in the colon despite sufficient cleansing, and approximately similar percentages of patients with diagnostic impairment in both patient groups—indicate that cleansing of the bowel does not improve diagnostic image quality in PET/CT.
From radioactivity measurements of stool samples, one study showed that secretion of 18F-FDG or its derivatives into the bowel lumen is a possible reason for bowel activity besides uptake in the bowel wall itself (10). Further, a positive correlation between areas of constipation in the colon and 18F-FDG uptake was described in the same study. Thus, large amounts of stool might irritate the intestinal wall, leading to increased secretion and therefore 18F-FDG accumulation in the lumen. Consequently, the hypothesis for our study was developed to eliminate irritating stool and avoid increased secretion of 18F-FDG into the bowel lumen. In several publications, reduction of bowel wall motion, particularly using anticholinergic muscle-relaxing drugs, was discussed to reduce 18F-FDG activity. However, previous results with anticholinergic drugs were rather controversial (7,8,11). Since such therapy is much more delicate than bowel preparation because of possible interaction with other drugs, a combination of both (laxative plus anticholinergic drug) did not seem useful. In addition, separating the effects of the 2 treatments would have been difficult.
Essentially all types of purging agents for bowel cleansing, senna-glycosides included, increase intestinal secretory activity either directly or indirectly (12). For sennosides, this effect seems to be achieved by activation of chloride channels in the bowel wall (13).
From a practical point of view and convenience for the patient, we selected a senna-glycoside which is easily applicable the day before the PET examination. All patients in the bowel-preparation group demonstrated significantly less stool in the colon, proving successful cleansing. However, the drug seemed to cause an activation/irritation of the colon clearly beyond a potential irritation caused by large amounts of stool, since significantly higher 18F-FDG uptake was demonstrated in the colon in the bowel-preparation group than in the native group. Interestingly, no difference was seen in the small bowel. Senna-induced colitis, causing inflammation and explaining the increased 18F-FDG activity, was not reported in our patients. Therefore, increased uptake can be related only to secretion or muscle activity. Muscle activity does not seem to be the cause of intestinal uptake, since motility reduction by the use of anticholinergic drugs could not demonstrate significant reduction in bowel uptake (11). It could be argued that secretion is probably also associated with increased bowel motility, which then causes increased 18F-FDG uptake. However, diffuse uptake in all colonic structures would be expected in such a case, which was not observed in our study. According to our results, which showed significantly increased intestinal 18F-FDG uptake in all colonic segments except the sigmoid/rectum, we postulate that activity in intestinal structures is caused mainly by 18F-FDG secretion into the bowel lumen. The nonsignificant difference in the in the rectum/sigmoid segment can be explained by the large number of patients in the native group with stool content, which seems also to cause increased secretion (10).
Interestingly, increased 18F-FDG uptake did not interfere with diagnostic quality. This was mainly due to the fact that increased 18F-FDG uptake observed in the bowel-preparation group was not focal but diffuse. Diffuse uptake is rarely related to malignant disease and therefore did not account for diagnostic impairment.
Regarding the limitations of this study, the natural randomization used to assign patients to the 2 groups could introduce a relevant selection bias (14). Natural randomization represented an easy approach with the greatest convenience for our patients. Statistical analysis of the patient population parameters showed no significant difference between the groups. If a selection bias had been introduced, we hypothesize that the bias would have been toward those patients with more severe disease choosing to enter the control group. Severely ill patients in general have also had more therapies influencing bowel habits (e.g., chemotherapy, radiotherapy, or resection), causing various effects including inflammatory changes and diarrhea. We believe that these effects would have introduced an increased intestinal 18F-FDG uptake, leading to a falsely high 18F-FDG accumulation in the native group, even underestimating the irritating effects of bowel preparation.
CONCLUSION
Bowel preparation using a purging procedure increases 18F-FDG activity in the large intestine and is therefore not useful before PET/CT.
Footnotes
-
COPYRIGHT © 2010 by the Society of Nuclear Medicine, Inc.
References
- Received for publication September 29, 2009.
- Accepted for publication December 10, 2009.





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.