


Article Figures & Data
Figures
- FIGURE 1.
(A) 18F-FLT. (B) 18F-FMAU.
- FIGURE 2.
Newly diagnosed glioblastoma. (A) MRI (contrast-enhanced T1-weighted image) shows large area of contrast enhancement in right frontal lobe. (B and C) Both 18F-FDG PET (B) and 18F-FLT PET (C) show increased uptake in same area. (Reprinted with permission of (189).)
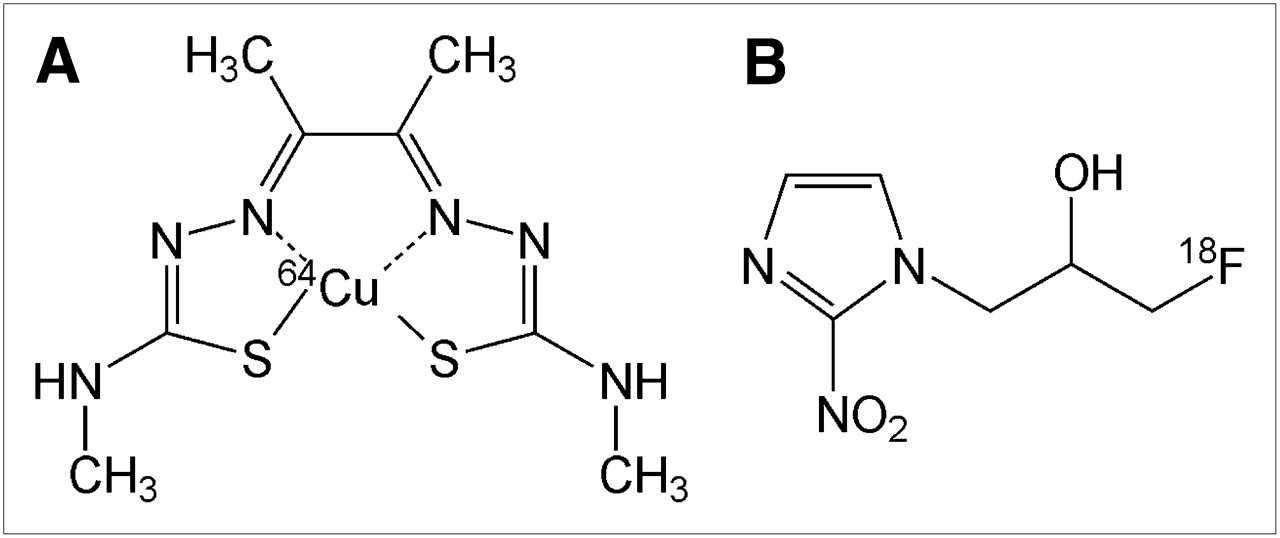
- FIGURE 3.
(A) 64Cu-ATSM. (B) 18F-FMISO.
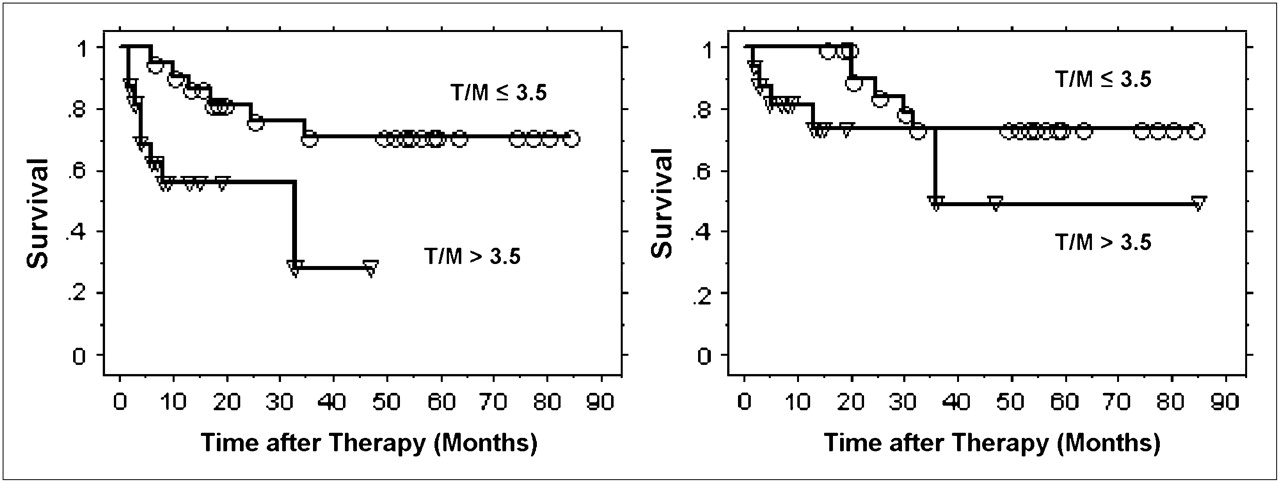
- FIGURE 4.
Progression-free survival (left) and cause-specific survival (right) determined from 60Cu-ATSM uptake by Kaplan–Meier method. ○ = event in patients with T/M of ≤3.5; ▿ = event in patients with T/M of >3.5. (Reprinted with permission of (83).)
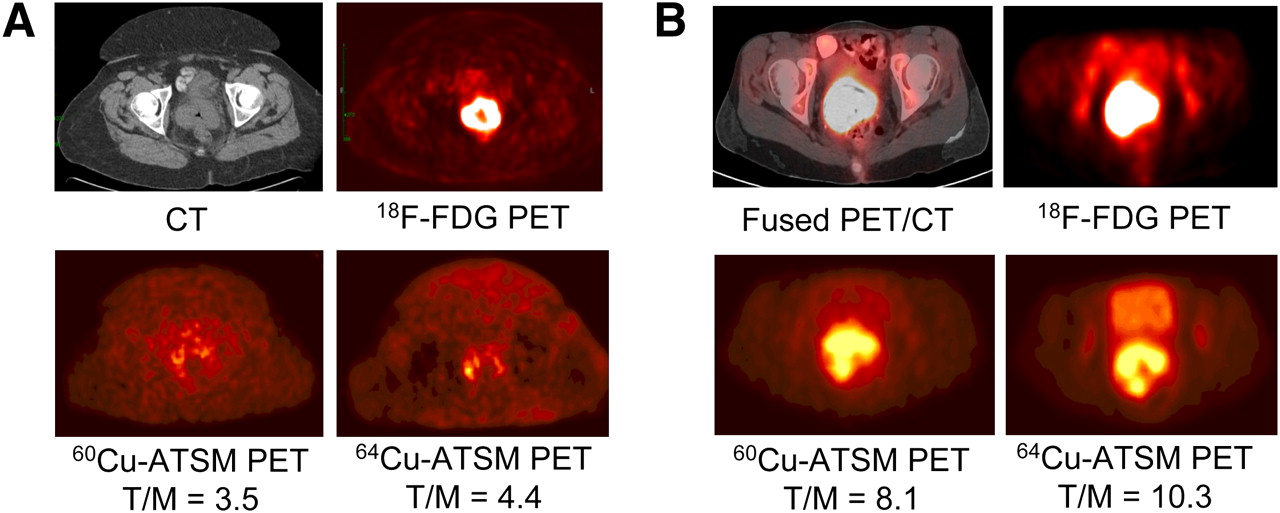
- FIGURE 5.
(A) Transaxial CT (top left) and 18F-FDG PET (top right) images of pelvis show intense 18F-FDG uptake within known cervical tumor at site of cervical mass seen on CT. Transaxial 30- to 60-min summed images of 60Cu-ATSM PET (bottom left) and 64Cu-ATSM PET (bottom right) of pelvis at same level demonstrate mildly increased uptake within known primary cervical tumor. There are similar patterns of 60Cu-ATSM and 64Cu-ATSM uptake within tumor. (B) Transaxial coregistered 18F-FDG PET/CT (top left) and 18F-FDG PET (top right) images of pelvis show intense 18F-FDG uptake within known cervical tumor at site of cervical mass seen on CT. Transaxial 30- to 60-min summed images of 60Cu-ATSM PET (bottom left) and 64Cu-ATSM PET (bottom right) of pelvis at same level demonstrate markedly increased uptake within known primary cervical tumor. There are similar patterns of 60Cu-ATSM and 64Cu-ATSM uptake within tumor. (Reprinted with permission of (86).)
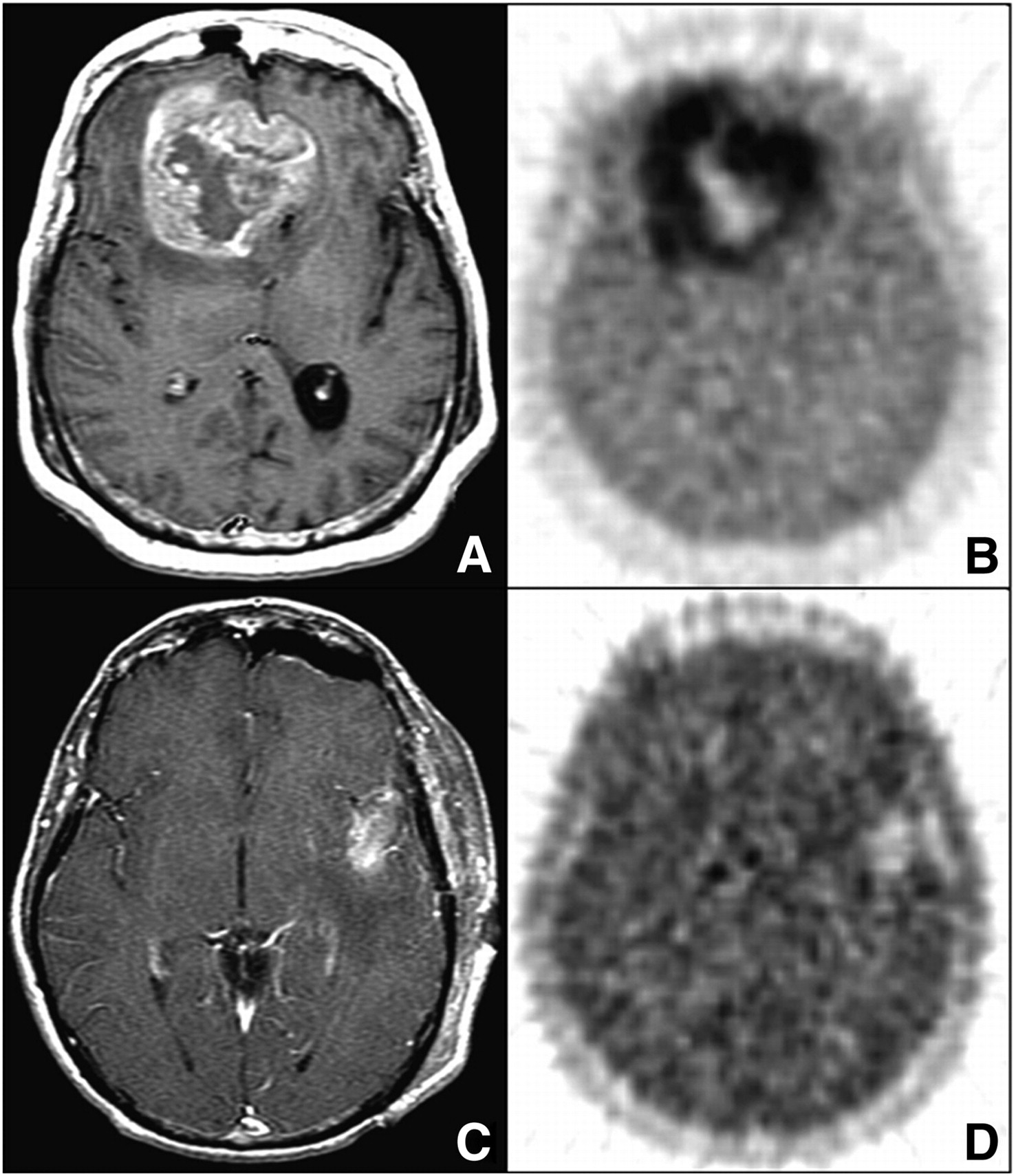
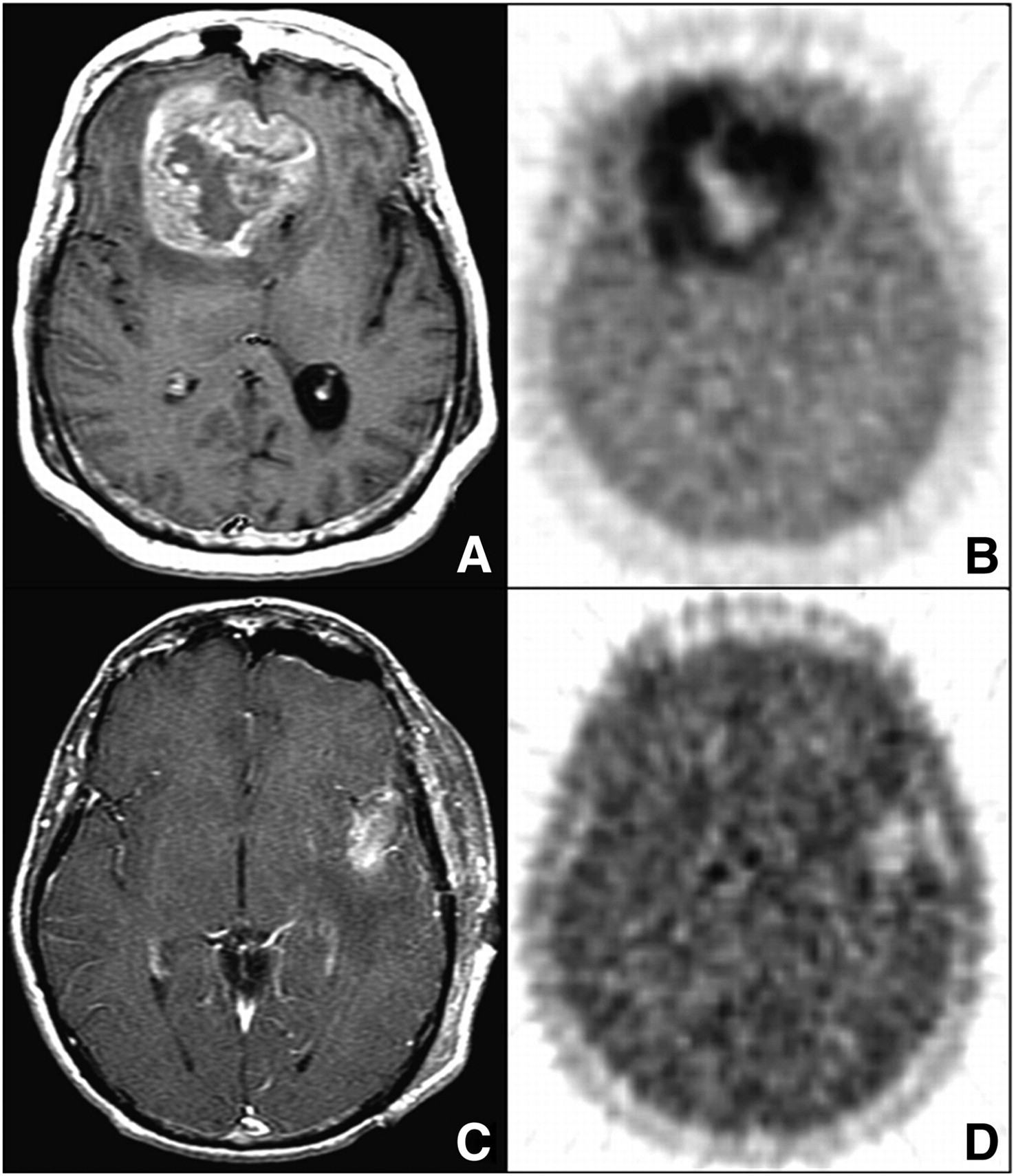
- FIGURE 6.
(A and B) Bifrontal glioblastoma multiforme imaged after biopsy in 55-y-old woman. (A) MRI (gadolinium-enhanced T1-weighted image [T1Gd]) shows large, contrast-enhancing, irregular ring-shaped tumor with necrotic center. Non–contrast-enhanced volume was 20 cm3, T1Gd volume was 80 cm3, and T2-weighted volume was 167 cm3. (B) 18F-FMISO image through same plane. HV was 129 cm3, and T/Bmax ratio was 3.0. (C and D) Left temporal glioblastoma multiforme imaged after gross total resection in 53-y-old man. (C) MRI (T1Gd) shows only blood products and no residual contrast-positive disease. Non–contrast-enhanced volume was 1 cm3, T1Gd volume was 7 cm3, and T2-weighted volume was 37 cm3. (D) 18F-FMISO image through same plane. HV was 5.3 cm3, and T/Bmax ratio was 1.6. (Reprinted with permission of (97).)
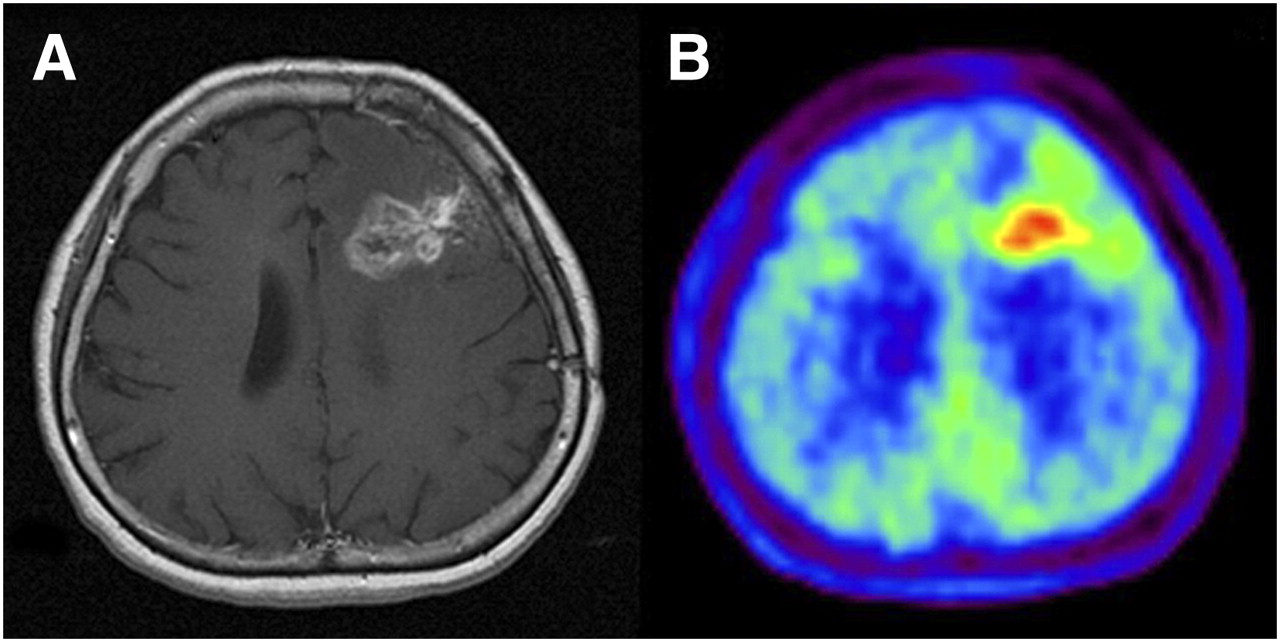
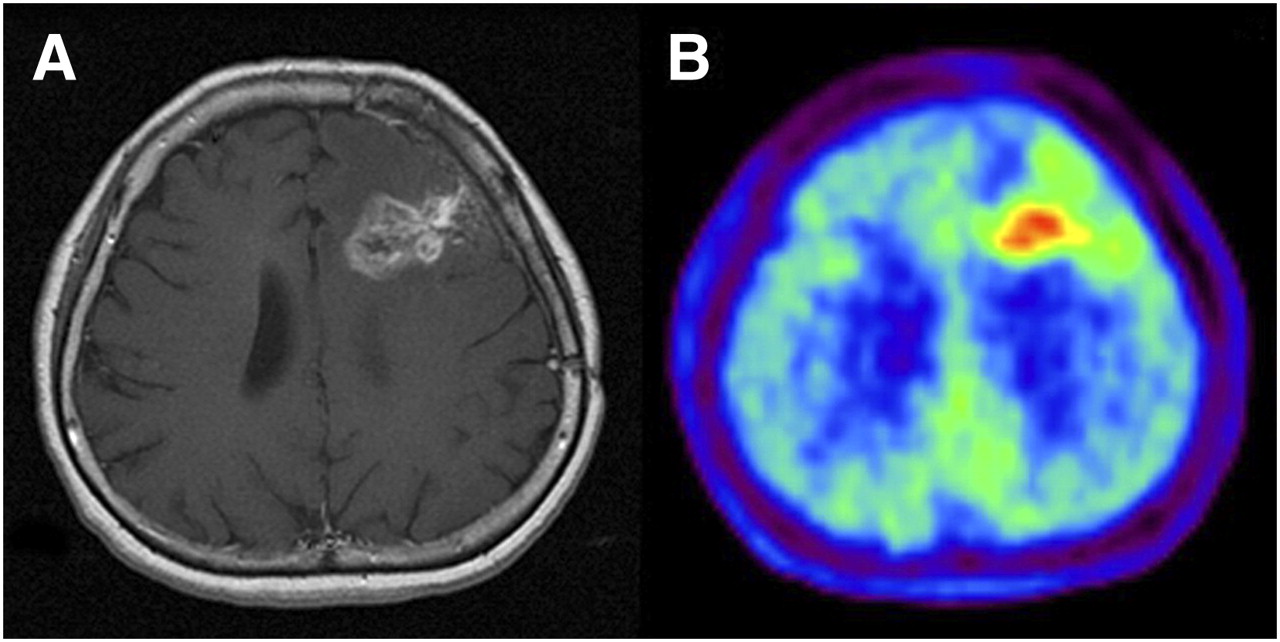
- FIGURE 7.
Imaging of 49-y-old woman who had been previously treated for glioblastoma multiforme with tumor resection and conventional radiotherapy at dose of 60 Gy. (A) T1-weighted MR image obtained with contrast medium 13 mo after initial surgery showed contrast-enhanced lesion in left frontal lobe. (B) 11C-MET PET image showed obvious accumulation of tracer corresponding to abnormality on MR image. Mean lesion-to-normal tissue ratio was 1.70. Recurrent tumor was pathologically confirmed by second surgery. (Reprinted with permission of (106).)
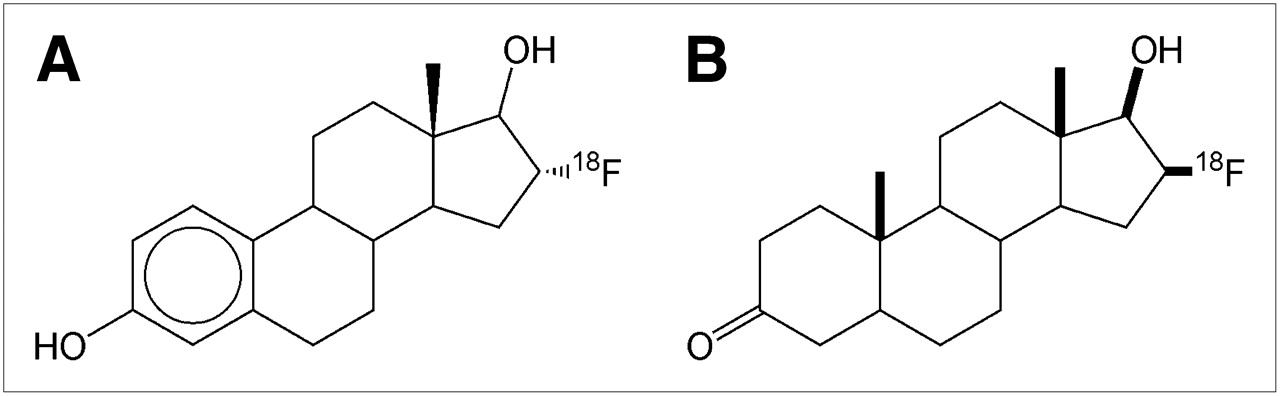
- FIGURE 8.
(A) 18F-FES. (B) 18F-FDHT.
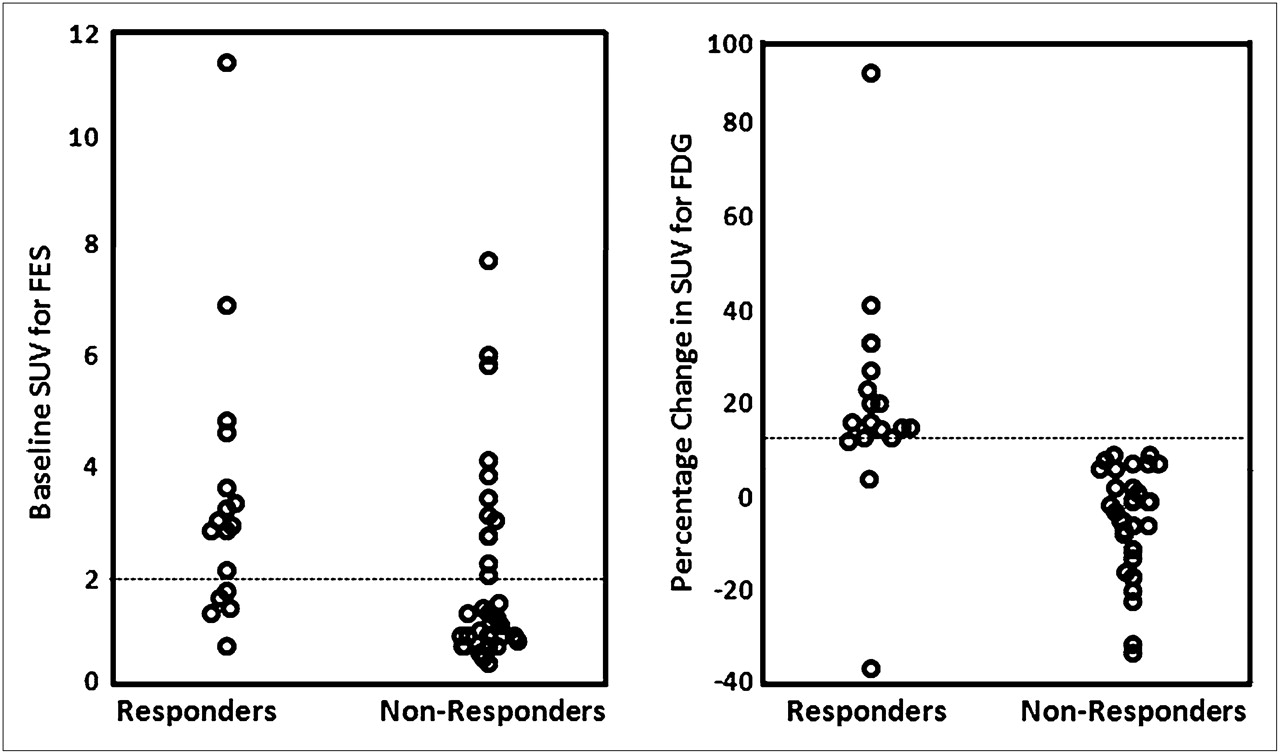
- FIGURE 9.
Baseline tumor 18F-FES (left) and percentage change in tumor 18F-FDG (right) uptake after estradiol challenge in patients who responded and patients who did not respond to endocrine therapy. (Reprinted with permission of (140).)
- FIGURE 10.
18F-FDHT (A) and 18F-FDG (B) scans displayed in maximum-intensity-projection format. This figure demonstrates the contrasting metabolism of the 2 tracers in a patient with metastatic prostate cancer. (Reprinted with permission of (158).)




Tables
- TABLE 1
Selected Clinical Studies Using Molecular Probes Other Than 18F-FDG for Monitoring of Therapy with PET
Agent Tumor type or stage Authors Year No. of patients Criteria for response on PET Outcome measures Hazard ratio P 18F-FLT Recurrent malignant glioma Chen et al. (57) 2007 19 SUV decrease of 25% Overall survival and TTP 5.0 0.02 18F-FLT Rectal cancer Wieder et al. (55) 2007 10 % decrease in SUV* Histopathologic response (<10% residual tumor) NR NS 18F-FLT Lymphoma Herrmann et al. (58) 2007 14 Posttherapy SUV* Complete vs. partial response NR 0.009 18F-FLT Lymphoma Kasper et al. (47) 2007 48 SUV < 1.5 Overall survival NR 0.016 60Cu-ATSM Non–small cell lung cancer, IA–IV Dehdashti et al. (84) 2003 14 T/M < 3.0 Response to therapy NR 0.002 60Cu-ATSM Cervical cancer, Ib1–IVa Dehdashti et al. (83) 2008 38 T/M < 3.5 Progression-free survival NR 0.01 60Cu-ATSM Rectal cancer, T2–T4 Dietz et al. (85) 2008 17 T/M < 2.6 Progression-free survival NR 0.05 18F-FMISO Head and neck cancer Rajendran et al. (96) 2006 73 T/Bmax ratio > 1.6† Overall survival 1.68 0.002 18F-FMISO Glioblastoma multiforme Spence et al. (97) 2008 22 T/Bmax ratio > 2.06† Overall survival 1.46 0.0002 18F-FMISO Head and neck cancer, III–IV Rischin et al. (99)‡ 2006 45 Qualitative scoring Locoregional failure (with different treatment regimens) 11C-MET§ Malignant glioma, II–IV Galldiks et al. (104) 2006 15 Decrease in % uptake TTP NR 0.01 18F-FES Breast cancer Dehdashti et al. (140) 2008 41 Pretherapy SUV ≥ 2 Overall survival NR NS 18F-FES Breast cancer Dehdashti et al. (144) 1999 11 % decrease in SUV* Clinical response NR 0.008 18F-FES Breast cancer McGuire et al. (141) 1991 16 NR Clinical response NR NR 18F-FES Breast cancer Mortimer et al. (143) 2001 40 Pretherapy SUV*and % decrease in SUV* Clinical response NR for both criteria 0.0007 for pretherapy SUV and 0.0003 for % decrease in SUV 18F-FES Breast cancer Mortimer et al. (145) 1996 43 Pretherapy SUV ≥ 1.0 Clinical response NR NS 18F-FES Breast cancer Linden et al. (142) 2006 47 SUV ≥ 1.5 Tumor response (modified RECIST) NR 0.01 ↵* No prospective SUV threshold was used; retrospective statistical correlations were derived.
↵† T/B ratio of ≥1.2 indicated severe hypoxia.
↵‡ See Rischin et al. (99) for hazard ratio and P value data; multiple treatment regimens were used.
↵§ See also Table 2 in article by Singhal et al. (103).
NR = not reported; NS = not statistically significant.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A Bridge Not Too Far: Linking Disciplines Through Molecular Imaging Probes
- Improved Differentiation of Benign and Malignant Breast Tumors with Multiparametric 18Fluorodeoxyglucose Positron Emission Tomography Magnetic Resonance Imaging: A Feasibility Study
- Early Assessment of Tumor Response to Gefitinib Treatment by Noninvasive Optical Imaging of Tumor Vascular Endothelial Growth Factor Expression in Animal Models
- Novel insights on imaging sex hormone-dependent tumourigenesis in vivo
- In Vivo Imaging in Cancer
- A Bridge Not Too Far: Linking Disciplines Through Molecular Imaging Probes
- Assessing Tumor Response to Therapy