


Abstract
This review highlights and compares risk assessment, predictive accuracy, and economic outcomes for 3 commonly applied cardiac imaging procedures: stress myocardial perfusion SPECT or PET and coronary CT angiography (CCTA). This review highlights an expansive evidence base for stress myocardial perfusion imaging and reveals a decided advantage for higher-risk patients, notably those who have established coronary artery disease (CAD). It is likely that the use of CCTA will continue to expand, particularly for patients with more atypical symptoms and patients with a lower likelihood of CAD. Despite a high level of evidence, comparative research is not available across modalities that could definitively drive utilization of cardiac imaging modalities.
Evidence about the accuracy of a variety of noninvasive imaging tests for the identification of at-risk patients with known and suspected coronary artery disease (CAD) has been evolving. Most of the early published research on noninvasive cardiology, from the 1980s and early 1990s, focused on the diagnostic accuracy of a test. More recent research has focused on evaluating the ensuing risk in patients with normal and abnormal cardiac imaging findings. Further exploration has been aimed at the graded or directly proportional relationships between the extent and the severity of imaging risk markers and major adverse cardiovascular events. These relationships highlight a common theme throughout the literature of ever-increasing and worsening cardiac event risk with more extensive and severe imaging abnormalities. More recent topics in the prognosis literature are the utility of new technology, such as coronary CT angiography (CCTA), and its accuracy compared with that of conventional testing, such as stress nuclear imaging. For this report, we compare risk assessment, predictive accuracy, and economic outcomes for 3 commonly applied cardiac imaging procedures: stress myocardial perfusion SPECT or PET and CCTA. We further highlight the potential value of hybrid imaging with PET/CT or even sequential imaging with SPECT plus CT.
CORRELATION BETWEEN MYOCARDIAL ISCHEMIA AND CORONARY ANATOMY
Early research focused on the accuracy of stress nuclear imaging for detecting obstructive coronary stenosis. Lessons learned from these evaluations were that the detection of obstructive stenosis was related to the severity of the stenosis, collateral flow, and underlying endothelial function. Documentation of high rates of false-positive results (i.e., ischemia with no obstructive CAD) with stress myocardial perfusion may be related to vascular dysfunction, an early marker of atherosclerosis. In addition, normal stress perfusion results in patients with CAD are related to many factors, including collateral blood flow or prior coronary revascularization. It is for these reasons that much of the recent imaging research has focused on risk determination. However, for discussion purposes, it is helpful to understand the relationship between ischemia and coronary anatomy.
INDUCIBLE ISCHEMIA DETECTED BY STRESS ELECTROCARDIOGRAPHY
In patients with chest pain and a low to intermediate likelihood of ischemia, a stress electrocardiogram without imaging is a first-line test for the evaluation of suspected CAD. The correlation between electrocardiographic parameters and CCTA-defined CAD was evaluated in 156 low- to intermediate-risk patients (1). In that report, only half of patients with ST segment depression had obstructive CAD on CCTA. Interestingly, compared with purely calcified or noncalcified plaque, mixed plaque was more often associated with ST segment depression, with an odds ratio of 1.5 (range, 1.2–1.9). Although CCTA-defined CAD is more strongly associated with perfusion than with ischemia detected by electrocardiography, ischemia is more commonly associated with mixed plaque, which is a more advanced form composed of both calcified plaque and noncalcified plaque. Given the current understanding of the ischemic cascade, the onset of ST segment depression occurs more often with significant CAD, which is now known from CCTA to include mixed, advanced plaque that is often stenotic.
An understanding of the ischemic cascade can also provide insight into the potential correlation across anatomic compared with other ischemic markers. Although reports on the relationship between echocardiography and CT have not been published, given that wall motion abnormalities occur later in the ischemic cascade, in the presence of more severe stenosis, we would expect the correlation between wall motion abnormalities visualized by echocardiography and CCTA-defined CAD to be stronger and more accurate. In contrast, the onset of a perfusion abnormality occurs earlier in the ischemic cascade, along with intermediate coronary stenosis, and may be detected more easily than wall motion abnormalities.
INDUCIBLE ISCHEMIA DETECTED BY STRESS MYOCARDIAL PERFUSION AND CCTA
To date, 7 reports on the correlation between ischemia detected by stress myocardial perfusion (SPECT or PET) and CCTA have been published (2–8). Most of the evidence reveals substantial variability between inducible ischemia and atherosclerotic plaque composition and constrictive remodeling severity. This variability has tremendous implications for diagnostic accuracy and risk determination and provides supportive evidence for the increasing application of hybrid or sequential imaging.
The underlying burden of atherosclerotic disease is often more severe and extensive than the burden of myocardial ischemia (3). Moreover, in patients undergoing a test for ischemia and CCTA, there is often substantial variability, with less than 25% of patients having concordant abnormal findings (3). As the prevalence of obstructive CAD increases, the correlation between stress myocardial perfusion and angiographic findings improves (2). For a lesion with a minimal cross-sectional area of less than 3.7 mm2 or greater than 60% stenosis, the diagnostic sensitivity and specificity of stress myocardial perfusion SPECT were 98% and 84%, respectively (2). An important finding was that the frequencies of inducible ischemia were 0%, 5%, 33%, 54%, and 86% for CCTA-defined stenosis of 0%, 0%−60%, 60%−70%, 70%−80%, and more than 80%, respectively (P < 0.0001) (2). Thus, when ischemia is present (excluding artifacts), the likelihood of obstructive CAD is high. Additionally, the accuracies of CCTA for the identification of 82Rb PET-defined ischemia were 67% for mild CAD (<50% stenosis), 85% for intermediate lesions (50%−70% stenosis), and 93% for significant CAD (>70% stenosis) (7). Specifically, the likelihood of CAD in patients with severe myocardial perfusion defects is high (7).
However, when stress myocardial perfusion results are normal, the opposite situation is not guaranteed; that is, obstructive CAD cannot be excluded. Patients with CAD on CCTA frequently have normal stress perfusion findings (4). Another way to state this concept is that CTA is a poor predictor of inducible ischemia (7). In patients with 3-vessel or left main CAD, balanced reduction may result in normal stress perfusion findings. In one recent report, all 9 patients with positive CCTA and normal perfusion findings had multivessel CAD (4).
Added Value of Determination of Coronary Calcium with Stress Myocardial Perfusion
There are several novel pathways by which patients may now be referred to nuclear imaging for the assessment of myocardial ischemia; one pathway is a high burden of coronary artery calcification (CAC). CAC imaging is indicated for patients with an intermediate Framingham risk score (9). Biomarkers and risk factors not included in the Framingham risk score may also be applied to define candidates for CAC testing, including patients with elevated levels of high-sensitivity C-reactive protein (≥3 mg/dL), patients with metabolic syndrome, and patients with a family history of premature CAD. The rationale for the determination of CAC is supported by current guidelines, systematic reviews, and large population studies that reported high cardiac event rates in women and men of diverse ethnicities and with high CAC scores (9–11). The risk of death from a cardiovascular event or myocardial infarction increases with the extent of CAC, from an annual rate of 0.4% for patients with no CAC to an annual rate of ≥2% for patients with high CAC scores (≥400) (11). The latter risk group signifies “coronary heart disease risk equivalent status,” with patients in this group having the same clinical outcomes as those with established CAD. Because of this elevated risk, evaluation of the underlying ischemic burden is reasonable for patients with high CAC scores.
The detection of CAC by SPECT or PET has been shown to provide incremental value to myocardial perfusion results (3,4,12). Specifically, when perfusion is normal, the addition of a CAC score can improve the detection of CAD—notably, severe multivessel CAD. 82Rb PET is also more accurate for the detection of 3-vessel or left main CAD, particularly for adding information on changes in the left ventricular ejection fraction or measuring coronary flow reserve after stress (13). However, the addition of a CAC scan to stress myocardial perfusion imaging may prove particularly valuable in patients with a higher prevalence of more severe and extensive CAD as well as patients with a higher likelihood of CAD (e.g., patients with diabetes and older patients) (3,14). On a very crude level, the addition of a CAC scan (with minimal radiation, ∼1 mSv) may be viewed as a “poor man's” coronary angiogram.
Although CAC is neither synonymous with nor site specific for obstructive CAD (9), there is a proportional relationship between the extent of CAC and inducible ischemia in asymptomatic and symptomatic patients. A recent consensus statement from the American Society of Nuclear Cardiology encompassed 5 published reports on the correlation between inducible ischemia and CAC findings. The results revealed that as the CAC-based Agatston score increased, the frequency of inducible ischemia increased (15). That is, the prevalence of inducible ischemia was low for CAC scores of less than 100 but increased dramatically for higher CAC scores. In one large observational series, the rate of inducible ischemia approached 20% for patients with CAC scores of ≥400 (16). The frequency of inducible ischemia is elevated in diabetic patients, patients with metabolic syndrome, and patients with a family history of premature CAD at a lower threshold—CAC scores of ≥100. Prognosis varies with 82Rb PET perfusion results and CAC scores; for example, for patients with normal stress PET results, higher cardiac event rates were associated with higher CAC scores (13). This finding of higher cardiac event rates in patients with normal stress perfusion results has been reported as a frequent occurrence in patients with known CAD or those with greater comorbidity (17). The documentation of CAC as a direct marker of atherosclerosis can be used to target patients requiring more intensive management of risk factors (such as secondary prevention goals in the presence of high levels of CAC).
Plaque Composition and Inducible Ischemia
Recent observations indicated that inducible ischemia is found more often in the presence of mixed or calcified plaque than in the presence of noncalcified plaque (5,8). Although these findings are preliminary, they suggest intriguing possibilities for the determination of risk with CCTA. It appears reasonable to suggest that ischemia would be more prevalent in more advanced plaque (i.e., calcified or mixed plaque), in which constrictive remodeling results in flow limitations. In addition, it has been hypothesized that noncalcified plaque is more vulnerable to progression to acute coronary syndromes (ACS). Should these data be validated in larger, prognostic patient series, documentation of noncalcified plaque may be a harbinger for near-term instability with an associated high risk of ACS. If such a relationship is reported, then the use of CCTA for the detection of “vulnerable” lesions may be an important strategy for the identification of at-risk patients (18). In a recent report, Motoyama et al. (19) revealed that the CCTA characteristics of plaque associated with ACS included constrictive arterial remodeling (i.e., coronary stenosis) and low plaque density (i.e., noncalcified plaque). Spotty calcification was also a marker for ACS, particularly when it surrounded areas of low plaque density (i.e., mixed plaque).
COMPARATIVE DIAGNOSTIC ACCURACY OF STRESS NUCLEAR IMAGING WITH CCTA
Although CCTA is a rather new modality, evidence is rapidly unfolding with regard to its accuracy in comparison with the accuracy of more traditional stress imaging tests, such as myocardial perfusion SPECT and PET. Five meta-analyses on the diagnostic accuracy of CCTA for the detection of obstructive CAD, confirmed by the gold standard of invasive cardiac catheterization, have been published (20–24). The most recent study reported excellent accuracy statistics for 64-slice CCTA; the diagnostic sensitivity and specificity were 94% (range, 93%−97%) and 85% (range, 80%−90%), respectively (24). The high correlation of a noninvasive angiogram with an invasive assessment of anatomic CAD is expected. In patients at a low–intermediate pretest likelihood, one strength of CCTA is its high negative predictive value, exceeding 95% (25). It remains likely that if CCTA has a radiation burden consistently lower (<4 mSv) than that currently applied, then its high negative predictive value would be an advantage for patients with a likelihood of CAD in the range of greater than 15% to less than 50% or for patients with more atypical chest pain symptoms.
Multicenter Clinical Trials with CCTA
This observational evidence has now been corroborated by 2 multicenter clinical trials of the diagnostic accuracy of CCTA (26,27). In the former trial (26), 230 patients underwent CCTA and invasive coronary angiography (59% men; mean age, 57 y). The diagnostic sensitivity and specificity for detecting ≥50% stenosis were 95% and 83%, respectively. Comparable diagnostic accuracy results were noted for nonobese and obese patients (a subset particularly problematic for SPECT). Of importance is the finding that diminished diagnostic specificity was reported for patients with CAC scores of greater than 400. The latter finding supports the utility of a functional assessment of ischemic burden by stress myocardial perfusion SPECT or PET in patients with a high likelihood of extensive CAC (e.g., older patients).
Diagnostic Accuracy of SPECT and PET
Contemporary myocardial perfusion SPECT has a diagnostic sensitivity in the range of 85%−90% (28). The reported high rate of false-positive (i.e., diminished-specificity) SPECT scans, particularly for women and obese patients, can be reduced by using attenuation correction algorithms as well as integrating the gated left ventricular ejection fraction and regional wall motion into test interpretations; diagnostic specificity can be improved to within the range of 80%−90% (29–33). The addition of a prone image has also been reported to improve diagnostic specificity (33). Higher diagnostic sensitivity statistics for the detection of CAD are consistently reported with stress 82Rb PET—on average, 5%−10% higher (13,34). In a recent study with 82Rb PET/CT, the diagnostic sensitivity and specificity were 93% and 83%, respectively (35); in particular, the accuracy for detecting multivessel CAD was exceedingly high. Major advantages of the use of myocardial perfusion PET are the abilities to quantify measures of absolute blood flow and to define areas of dampened coronary flow reserve (36). The addition of nonperfusion findings, such as changes in the left ventricular ejection fraction, and the addition of a CAC scan can further improve the detection of CAD by PET (13).
RISK STRATIFICATION WITH CARDIAC IMAGING
There is an abundance of available evidence about the risk of major adverse cardiovascular events after stress myocardial perfusion SPECT (17); more recent reports note similar findings for 82Rb PET (37,38). The large body of literature demonstrates that as the extent and severity of perfusion abnormalities worsen, the ensuing major cardiac event rates increase; thus, there is a directly proportional relationship between stress perfusion abnormalities and prognosis (Fig. 1) (17). For patients with normal stress perfusion results, the annual cardiac death or nonfatal myocardial infarction rate is 0.6% but varies from a low of 0.3% for women to a high of nearly 2% for patients undergoing pharmacologic stress imaging (16,17). This range of event rates mirrors the scale of events noted for patients with CAC scores of 0 to as high as 400 or more. Thus, in the setting of normal stress perfusion results, one may expect a “sliding scale” in terms of anticipated annual events; the rate may decrease in lower-risk populations and may increase nearly 3-fold in higher-risk patients with more extensive comorbidities (e.g., older patients or patients with known CAD). One may anticipate that adding CAC scores for patients with more extensive comorbidities will further guide risk-reducing, preventive decision making. It should be noted that the issue of Bayesian theory affecting accuracy is relevant to all imaging modalities including CCTA and SPECT; yet with CCTA there is a limited evidence base to explore this relationship with the same assuredness as with SPECT imaging.

Comparative 1-y cardiac event rates for coronary CT angiography (CTA) and stress myocardial perfusion SPECT or PET. (Left) Low-risk findings of either normal perfusion or no obstructive CAD. (Right) Moderate- to high-risk findings of moderate to severely abnormal perfusion or obstructive CAD.
For patients with inducible perfusion abnormalities, mild abnormalities (e.g., summed stress score [SSS] of 4–8) are associated with higher event rates, generally in the range of 1%−3% (39). The Cedars–Sinai group has suggested that higher rates of myocardial infarction (compared with death) may be seen in patients with mild perfusion abnormalities. This finding is supported by serial angiographic results showing more progressive CAD in patients initially presenting with subcritical stenosis. Although speculative, the observation of elevated rates of acute myocardial infarction was validated in a recent multicenter registry (40). More extensive and severe perfusion abnormalities, encumbering 10% or more of the myocardium, are associated with up to 5% annual cardiac event rates. The latter subset is decidedly high risk and favors the use of intensive risk factor management (including secondary prevention targets), aggressive anti-ischemic therapy, and consideration of coronary angiography and revascularization (when appropriate). A general tenet of therapeutic intervention is that as the risk in a given population increases, so does the relative risk reduction. That is, patients with high-risk perfusion abnormalities will benefit, in terms of dramatic reductions in risk, from very intensive posttest therapeutic intervention.
Prognostic Accuracy of Stress PET
More recent data are available regarding prognosis predicted by 82Rb PET (37,38). In a cohort of 1,441 patients undergoing pharmacologic stress PET, annualized all-cause mortality rates were 2.4% for SSS of 0–3, 4.1% for SSS of 4–8, and 6.9% for SSS exceeding 8 (P < 0.001) (37). In a related series of 367 patients, annual cardiac event rates were 0.4%, 2.3%, and 7.0% for normal, mild, and moderate to severe stress 82Rb PET findings, respectively (38). Risk-adjusted survival models revealed that 82Rb PET SSS were the strongest predictors of cardiac events. Importantly, 82Rb PET results provided improved risk stratification for obese patients and for patients after indeterminate SPECT results. Several series with 82Rb PET perfusion noted a contribution to risk determination by the addition of measurement of changes in the ejection fraction, improving the identification of 3-vessel CAD (13,37).
Prognostic Accuracy of CCTA
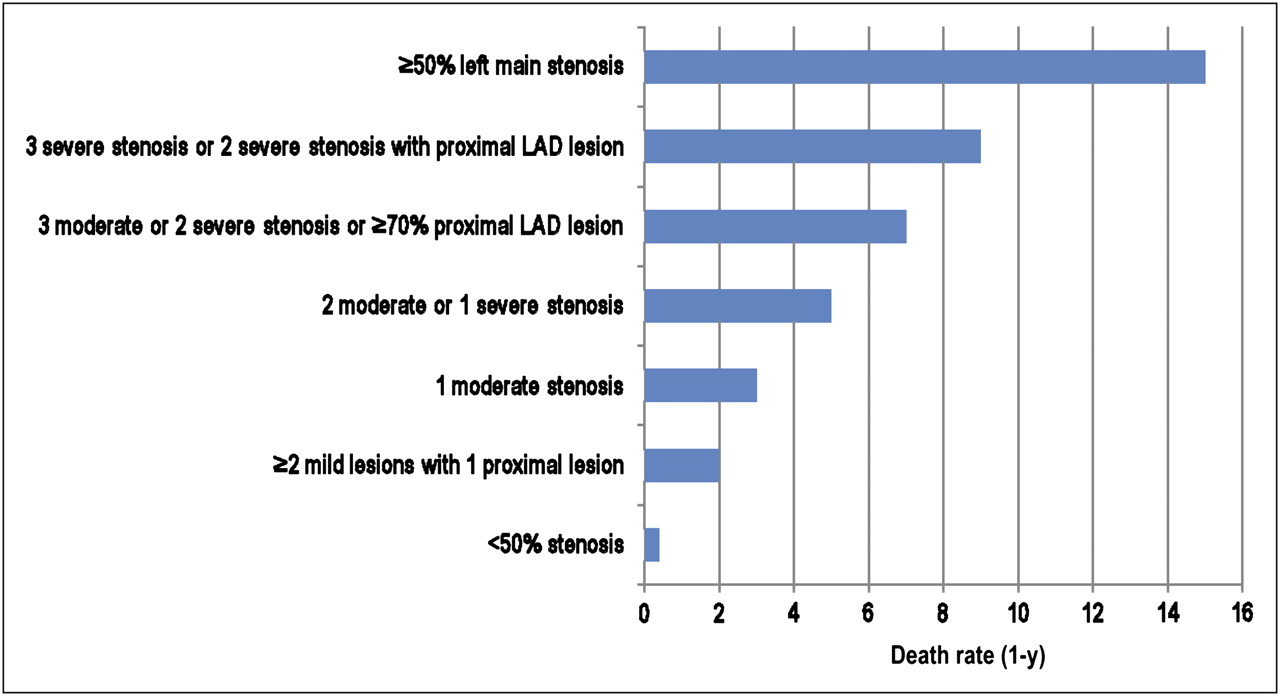
A similarly low 1-y cardiac event rate was reported for patients without obstructive CAD on CCTA (0.6% of 1,371 patients) (41–45). In a series of 810 patients (43), the 3-y cardiac event rate was 1.2% for patients without obstructive CAD. For patients with obstructive CAD, the results from 5 published reports revealed a 1-y cardiac event rate of 14.5% (n = 543) (41–45). Given the limited evidence regarding prognosis predicted by CCTA, one would expect this rate to decline as larger patient series are evaluated. In the largest series (n = 1,127) published to date (42), event rates were higher for patients with CCTA-defined proximal left anterior descending CAD and multivessel CAD, and survival worsened with ever-increasingly higher Duke CAD Prognostic Index scores (Fig. 2). This angiographic index incorporates both the site and the severity of any stenosis, as well as the number of obstructed vessels. Although initially devised and validated for invasive angiographic subsets, the gradations in risk for invasive angiography are similar to those now reported for patients undergoing CCTA.

One-year all-cause death rates by extent and severity of CCTA results in 1,127 patients. LAD = left anterior descending coronary artery.
SERIAL TESTING PARADIGMS FOR STRESS NUCLEAR IMAGING OF PATIENTS WITH CAD
There is now a further evolution of clinical trials using stress myocardial perfusion ischemia as an integral component within strategies of medical and surgical intervention for CAD patients. Observations support a threshold of 10% myocardial ischemia or more as critical for deriving optimal benefit from coronary revascularization (46). In one study of 10,627 patients, cardiac death rates were significantly lower for patients who had ≥10% ischemic myocardium who underwent coronary revascularization when compared with medical management. Conversely, medical management was associated with improved survival for patients with non–high-risk ischemia (i.e., no multivessel or anterior ischemia or increased lung uptake) (47). In management strategies for stable ischemic heart disease, the integration of stress nuclear imaging entails serial testing to assess the effectiveness of a therapeutic intervention. This strategy was initially undertaken in patients who had CAD and were enrolled in a trial comparing angioplasty with medicine; in that trial, the normalization of stress planar 201Tl perfusion was associated with improved survival after 6 mo of randomized treatment with medical therapy or angioplasty (48). Smaller studies with SPECT consistently reported reduced stress-induced ischemia in patients receiving nitrates, calcium antagonists, β-blockers, or statin therapies (49).
This paradigm of serial testing for patients with CAD was recently evaluated in a trial entitled the Clinical Outcomes Using Revascularization and Aggressive druG Evaluation (COURAGE trial) (49). The evidence suggested that ischemia is an integral marker for therapeutic decision making for patients with stable ischemic heart disease (50). Technical points worth noting when using serial testing are to match the type of stress, repeat the test when patients are on medications (vs. when not taking medications for the baseline scan), and watch for significant improvement or worsening on the second scan that exceeds test repeatability (e.g., a change on repeat imaging of ≥5% of the quantitative total perfusion deficit or SSS of ≥4) (49–51). This paradigm is optimally applied for patients who have CAD and demonstrable ischemia before treatment, particularly those with moderate to severe index ischemia.
The COURAGE trial was a randomized trial including patients with CAD and stable chest pain symptoms; the vast majority had multivessel CAD. In the COURAGE trial nuclear substudy, patients were generally tested 1 y after percutaneous coronary intervention (PCI) plus optimal medical therapy (OMT; an array of anti-ischemic and risk factor–reducing therapies) (PCI + OMT) versus OMT alone. Patients randomized to receive PCI + OMT had a greater reduction in inducible ischemia than those randomized to receive OMT alone. Overall, 33% of patients receiving PCI + OMT showed a reduction in their ischemic burden of ≥5% of the myocardium; the corresponding value for patients receiving OMT alone was ∼20% (P = 0.004). Reductions in ischemia were associated with improvements in angina frequency and stability.
In an exploratory prognostic analysis, patients not showing a reduction in their ischemic burden by at least 5% of the myocardium had worsening death or myocardial infarction rates compared with patients exhibiting greater reductions in ischemia. Thus, a failure to reduce a patient's ischemic burden signifies high-risk status warranting intensification of OMT and consideration of repeat angiography for CAD progression (including revascularization, if warranted). Other critical markers of risk during serial testing are the extent and severity of residual ischemia. After either OMT or revascularization, the extent and severity of residual ischemia were powerful prognostic factors in the COURAGE trial. For patients with an increasing burden of residual ischemia, higher death or myocardial infarction rates were reported. Survival (no death or myocardial infarction) rates were 100%, 84%, 78%, and 61% for patients with 0%, 1%−4.9%, 5%−9.9%, and ≥10% ischemic myocardium, respectively (P < 0.0001) (Fig. 3). However, the COURAGE trial nuclear substudy included only 314 patients, and the ensuing prognostic results were exploratory. Within this small cohort of patients, it appeared that patients with moderate to severe ischemia, encumbering 10% or more of the myocardium, exhibited more definitive benefits—greater reductions in ischemia and relative risk reductions of ∼50%—when their ischemic burden was reduced by 5% or more of the myocardium. Given these preliminary findings, we await future trials randomizing patients with at least 10% ischemic myocardium to PCI + OMT versus OMT alone.

Annual death or nonfatal myocardial infarction rates by percentage of residual ischemic myocardium on repeat imaging (at 1 y) after PCI + OMT or OMT alone.
RESOURCE USE AND COST-EFFECTIVE STRATEGIES
There is a wealth of economic evidence applying to stress myocardial perfusion SPECT and PET as well as more recent comparative evidence about the value of using CCTA (Table 1) (52–56). Although earlier reports with decision models explored the cost-effectiveness of a variety of noninvasive tests (57–61), more recent applications have relied on “real-world” data to devise models for comparing the incremental cost-effectiveness of stress myocardial perfusion imaging with that of noninvasive procedures, such as CCTA. Models that rely on real-world data can be used to more precisely describe current practice patterns and devise more efficient strategies of care or even dominant strategies (i.e., strategies with lower costs and enhanced effectiveness).
Economic Analysis of Stress Myocardial Perfusion SPECT or PET and Invasive Catheterization or CCTA
Before we embark on a review of current economic data, we discuss several reports that describe near-term resource use data and may also provide some insight into the comparative value of a given cardiac imaging procedure. Figure 4 shows a comparison of the posttest use of coronary revascularization in patients referred for stress myocardial perfusion SPECT or PET (defined as the functional diagnostic approach) with the anatomic diagnostic approach (either invasively or with CCTA). The diagnostic strategy of direct invasive angiography resulted in higher rates of coronary revascularization without improvements in clinical outcomes (52). Reductions in revascularization were recently seen with stress 82Rb PET (56). An anatomic diagnostic approach with CCTA resulted in even lower revascularization rates than invasive catheterization, yet its rate of PCI or coronary artery bypass surgery was ∼2-fold higher than that of stress myocardial perfusion imaging (41,44,45,54,55). It appears that anatomic approaches, either invasive or noninvasive, result in higher rates of revascularization. We await additional details about the costs of anti-ischemic therapies, which may be higher with functional testing, resulting in similar total costs.

Comparative analysis of use of coronary revascularization in patients referred for direct anatomic testing or direct functional testing. (Left) Earlier data showing higher rate (more than 2-fold) of revascularization with direct invasive angiography than with myocardial perfusion SPECT (MPS). (Right) Comparison of initial anatomic testing with CCTA and functional testing with MPS. These more recent data revealed rates of revascularization lower than those obtained with invasive anatomic strategies. Importantly, however, anatomic testing with CCTA resulted in higher rates of revascularization than did functional testing with MPS.
Defining Cost-Effectiveness
The term “cost-effectiveness” is often used inappropriately in the medical literature but, by definition, it provides an assessment of the value of a test-driven strategy. Cost-effectiveness analysis (CEA) may be calculated as the incremental cost of a given test strategy divided by the marginal difference in effectiveness. CEA is generally defined as the change in cost per life year saved with a threshold of economic efficiency set at less than $50,000 per life year saved. In countries with limited resources, the CEA has been set at less than $20,000 per life year saved. There are several means by which a diagnostic procedure may be proven cost-effective. First, the test can be less costly (including the subsequent or induced costs associated with a given index procedure) and slightly less effective yet remain cost-effective. Second, the test can be more costly (including induced costs) and more effective, thus producing a favorable CEA ratio. The latter strategy is more commonly seen in the cardiac imaging literature with the introduction of new technology. Third, the test can be less costly and more effective and is termed a “dominant strategy.” Finally, 2 comparative tests can be similarly effective or have similar clinical outcomes, but lower costs favor one of the tests. The latter situation is termed a “cost savings” or “cost minimization” approach and can be used only when outcomes are equivalent.
The United Kingdom's National Institute of Clinical Excellence performed a systematic review of the cost-effectiveness literature on stress myocardial perfusion SPECT, noting that favorable CEA data supported its utility for patients with an intermediate risk of CAD (62,63). More recently, the American Society of Nuclear Cardiology published a statement on CEA of stress myocardial perfusion SPECT (64). This document highlights the diversity of CEA data in nuclear imaging, including economic analyses of SPECT for the evaluation of acute chest pain in emergency departments (EDs), as well as evaluation of patients with suspected or known CAT in the outpatient setting.
Cost Savings with Stress SPECT
In the ED, nuclear imaging has been shown to elicit cost savings (of up to $700) for patients with equivocal biomarkers or nonspecific electrocardiographic findings. Importantly, the negative predictive value of nuclear imaging is exceedingly high (>95%), supporting the use of nuclear imaging as an effective gatekeeper for hospitalization and for minimizing the number of patients with missed ACS. More recently, this concept of using nuclear imaging in EDs was challenged by 2 reports on the utility of CCTA (65,66). In the first report, from a single center (62), CCTA was performed without the knowledge of ED physicians. Although only 14 of 103 enrolled patients had ACS, the negative predictive value for CCTA was 100%. In the second report, for a single-center randomized trial comparing CCTA with myocardial perfusion SPECT (for 197 low-TIMI [Thrombolysis in Myocardial Infarction]-risk patients presenting to an ED for the evaluation of acute chest pain), the results revealed that both CCTA and nuclear imaging were equally safe (i.e., no procedural complications) and accurate (defined as the correct identification of patients with CAD or the correct discharge of patients with negative test results and no events 6 mo later) (accuracies of 95% for CCTA and 91% for nuclear imaging; P = 0.24) (66). However, CCTA offered a significantly shorter time to diagnosis than nuclear imaging (∼3 vs. 15 h; P < 0.001) and cost savings of ∼$300 (P < 0.001). Frequent hurdles in the performance of nuclear imaging in EDs have been reported and, given the common noncardiac applications of CT in EDs, the more recent findings do support a CCTA-guided approach for the evaluation of acute chest pain. Importantly, early postacute myocardial infarction stress myocardial perfusion imaging in stable, uncomplicated cases has been shown to be cost-effective, with substantial cost savings, by identifying patients who can be safely discharged after normal or low-risk stress perfusion imaging results at days 2–5 after infarction (51). Thus, although the comparative economic evidence in EDs favors CCTA, it appears that stress myocardial perfusion imaging has proven value for patients who have a low to intermediate TIMI risk score and a stable postinfarction course and who may be safely discharged at days 2–5 after normal stress perfusion imaging results.
There is an abundance of economic literature on the comparative evaluation of stress nuclear imaging for patients with stable chest pain symptoms (51–53,56,67–71). Several reports have noted that, compared with a direct angiographic approach, stress nuclear imaging can provide significant cost savings (∼30%−40%) for 2–3 y of follow-up cardiac care (52,53,56,69,70). Notably, the cost advantages of stress nuclear imaging are most prominent when it is applied to a population at intermediate risk of CAD. This evidence is similarly applicable for women and men as well as for people with and people without diabetes (53,67). For patients presenting for the evaluation of stable chest pain, the extent and severity of ischemia are major drivers of clinical outcomes as well as costs. Patients with moderate to severe perfusion abnormalities require more intensive, costly care, including frequent referral for coronary angiography, more intensive anti-ischemic therapies, and coronary revascularization (when appropriate). The cumulative costs for these required procedures and therapies can result in a high-cost pattern of care. Of course, for high-risk patients, the net health benefit can be defined as the clinical outcome resulting when an ischemic burden is not detected and not treated, with ensuing adverse sequelae, which may include death or some other major cardiac event. Patients with stable chest pain also have substantial out-of-pocket expenses (or indirect costs), which approach $2,000/y (71). Thus, the costs of care for patients referred to a stress nuclear imaging laboratory can be quite high. Comparative CEA is helpful for devising a metric for this health care spending level.
Incremental Cost-Effectiveness of Stress SPECT
In a recent report, Shaw et al. compared the CEA of exercise myocardial perfusion SPECT with that of exercise echocardiography in 9,521 patients presenting for the evaluation of stable chest pain symptoms (68). Although nuclear imaging had slightly higher diagnostic or procedural costs ($419 vs. $294), the CEA ratios varied on the basis of the pretest risk in the population. For patients whose pretest risk was low to intermediate (i.e., <50% pretest risk), the CEA ratio was favorable for exercise echocardiography, at less than $20,000 per life year saved. Importantly, for patients undergoing exercise echocardiography, coronary angiography rates were lower. And, for exercise echocardiography patients undergoing coronary angiography, the ratio of angiography to revascularization was high compared with that for patients undergoing myocardial perfusion SPECT. A high ratio of angiography to revascularization is favorable and indicates a more selective referral of patients who have CAD and require surgical intervention. However, for patients with a higher likelihood of CAD, including those with intermediate to high pretest risk or known CAD, exercise nuclear imaging was decidedly more advantageous, with a CEA ratio of $32,381 per life year saved. Importantly, for nuclear imaging, there was an early (≤90-d) posttest referral to angiography and revascularization—a rate 2-fold higher than that for echocardiography. Early revascularization resulted in a 3-y improvement in life expectancy (1.2 y longer than that for patients undergoing revascularization after echocardiography). For patients with an intermediate to high likelihood of CAD, the higher-cost strategy of nuclear imaging was offset by a decided improvement in life years saved, thus producing a favorable CEA ratio for nuclear imaging versus exercise echocardiography.
Comparative Cost Savings of CCTA and SPECT
Stress myocardial perfusion SPECT was compared with CCTA in 2 reports (54,55). For patients with suspected CAD, the high negative predictive value of CCTA resulted in a more efficient diagnostic pathway, with cost savings of ∼$600 for CCTA versus SPECT (55). For patients with known CAD, the costs of care were $2,451 higher with CCTA than with stress myocardial perfusion SPECT because of repeated invasive angiography after CCTA. In a related report of 1,647 patients undergoing CCTA and 6,588 patients undergoing stress myocardial perfusion SPECT for suspected CAD (54), risk-adjusted CAD costs were ∼25% lower (i.e., ∼$1,075) with CCTA than with myocardial perfusion SPECT. Interestingly, the higher costs associated with nuclear imaging were the result of a 6-fold greater use of angiography after nuclear imaging. Importantly, 9-mo clinical outcomes were similar with these 2 modalities, indicating “true” cost savings for CCTA in this comparison. This analysis was derived from administrative claims data that were nonrandomized, resulting in uncontrolled differential case-mix and other practice patterns. Although stress myocardial perfusion SPECT has well-established pathways to angiography, it remains plausible that such pathways will evolve over time and favor CCTA. We await additional comparative evidence to support cost-savings strategies for either CCTA or stress myocardial perfusion imaging. A large-scale randomized trial involving CEA of CCTA and more conventional ischemia tests, such as stress myocardial perfusion SPECT or PET, is being designed.
NEW STANDARDS FOR ASSESSMENT OF OUTCOMES
The Centers for Medicare & Medicaid Services recently put forth an additional standard for evaluating cardiac imaging test performance (72,73). The new standard focuses on the impact of an imaging modality on health outcomes. In a broader sense, this new standard requires evidence more rigorous than that published so far and stipulates that a given imaging modality must improve patient outcomes. That is, a patient must have an improved health status (i.e., improved quality of life or well-being) or life expectancy. There are few examples of this new standard of establishing a net improvement in health outcomes. However, it is clear that this new evidence will become a standard for the effectiveness of cardiac imaging procedures and a method for allocating finite resources within a framework of quality imaging standards; thus, “equitable” cost shifting may be possible. With regard to this new standard of improving health outcomes for cardiac imaging procedures, the vast majority of current evidence does not meet this new standard. This discussion on research focusing on improved health outcomes is relevant because imaging modalities with a significant gap in research may face ever-increasing difficulties in garnering reimbursement. In addition, the new standard is important because the U.S. Food and Drug Administration approval process currently does not require evidence of a net improvement in health outcomes. Therefore, as the new standard put forth by the Centers for Medicare & Medicaid Services becomes a threshold upon which coverage decisions are based, there will remain a gap in research. This gap should become a major priority for medical societies, such as the Society of Nuclear Medicine and the American Society of Nuclear Cardiology; research efforts should be focused on ensuring high-quality imaging, and innovative imaging technology should be introduced to the medical marketplace as expeditiously as possible. In addition, new imaging technology should be widely used by the clinical community only if high-quality evidence has been obtained for that technology.
CONCLUSION
There is an expansive evidence base for the clinical and economic outcomes associated with a variety of cardiac imaging procedures. The data for stress myocardial perfusion imaging are robust and reveal a decided advantage for higher-risk patients, notably those who have established CAD and for whom therapeutic decision making (including the use of coronary revascularization) is inextricably linked to the extent and severity of inducible ischemia. As patterns of testing develop in this era of declining reimbursement, stress nuclear imaging has a strong advantage over many other procedures for high-risk patients. It is likely that the use of CCTA will continue to expand, particularly for patients with more atypical symptoms and patients with a lower likelihood of CAD. We await the development of a large observational registry and clinical trial data for both cardiac PET and CCTA to suggest optimal testing strategies for producing improved clinical outcomes or providing economic value to the health care system. Our synthesis of economic and prognostic evidence into a possible optimal testing strategy is shown in Figure 5.

Possible optimal testing strategy for specific subsets of patients (those with lower likelihood [LK] of CAD and those with higher LK of CAD). Strategy was based on consideration of added clinical and economic outcomes of each procedure for each patient subset.
Footnotes
-
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH AUGUST 2010.
-
No potential conflict of interest relevant to this article was reported.
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.
- 7.↵
- 8.↵
- 9.↵
- 10.
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.
- 22.
- 23.
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.
- 31.
- 32.
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.
- 59.
- 60.
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- Received for publication November 19, 2008.
- Accepted for publication February 9, 2009.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- CORRELATION BETWEEN MYOCARDIAL ISCHEMIA AND CORONARY ANATOMY
- INDUCIBLE ISCHEMIA DETECTED BY STRESS ELECTROCARDIOGRAPHY
- INDUCIBLE ISCHEMIA DETECTED BY STRESS MYOCARDIAL PERFUSION AND CCTA
- COMPARATIVE DIAGNOSTIC ACCURACY OF STRESS NUCLEAR IMAGING WITH CCTA
- RISK STRATIFICATION WITH CARDIAC IMAGING
- SERIAL TESTING PARADIGMS FOR STRESS NUCLEAR IMAGING OF PATIENTS WITH CAD
- RESOURCE USE AND COST-EFFECTIVE STRATEGIES
- NEW STANDARDS FOR ASSESSMENT OF OUTCOMES
- CONCLUSION
- Footnotes
- References
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- Ischaemia change with revascularisation versus medical therapy in reduced ejection fraction
- Computed tomographic coronary angiography - is it ready as a screening tool for coronary artery disease?
- Nuclear cardiology
- Ischemia Change in Stable Coronary Artery Disease Is an Independent Predictor of Death and Myocardial Infarction
- Coronary Computed Tomography Angiography: CONFIRMations and Perspectives
- Intermediate Lesions: Retrieving Black From Shades of Gray
- PET Assessment of Myocardial Perfusion Reserve Inversely Correlates with Intravascular Ultrasound Findings in Angiographically Normal Cardiac Transplant Recipients