


Abstract
Some antihistamine drugs that are used for rhinitis and pollinosis have a sedative effect as they enter the brain and block the H1 receptor, potentially causing serious accidents. Receptor occupancy has been measured with PET under single-dose administration in humans to classify antihistamines as more sedating or as less sedating (or nonsedating). In this study, the effect of repeated administration of olopatadine, an antihistamine, on the cerebral H1 receptor was measured with PET. Methods: A total of 17 young men with rhinitis underwent dynamic brain PET with 11C-doxepin at baseline, under an initial single dose of 5 mg of olopatadine (acute scan), and under another 5-mg dose after repeated administration of olopatadine at 10 mg/d for 4 wk (chronic scan). The H1 receptor binding potential was estimated using Logan graphical analysis with cerebellum as reference region input. Results: The acute scan showed a slight decrease in H1 receptor binding potential across the cerebral cortex (by 15% in the frontal cortex), but the chronic scan showed a marked decrease (by 45% from the acute scan in the frontal cortex). Behavioral data before and after the PET scans did not reveal any sedative effect. Conclusion: The results may be interpreted as either intracerebral accumulation of olopatadine or H1 receptor downregulation due to repeated administration. The study shows feasibility and potential value for PET in evaluating the pharmacologic effect of a drug not only after a single dose but also after repeated administration.
Antihistamines are widely used as a medication for common allergic disorders such as seasonal pollinosis, chronic rhinitis, and urticaria. Some antihistamine drugs have a sedative side effect as they enter the brain and block histamine H1 receptor, potentially causing traffic accidents and other serious events, but the sedative effect is difficult to evaluate because of a large variation in neuropsychological measures and subjective symptoms. Measurement of cerebral histamine H1 receptor occupancy using PET with 11C-doxepin under a single administration of antihistamines has been effective in evaluating the sedative effect, allowing the drugs to be classified as more sedating or as less sedating (or nonsedating) (1,2). Olopatadine is a widely used antihistamine with high antiallergy efficacy and has been reported to be less sedating on the basis of PET measurements and neuropsychological tests (3). A mild sedative effect has been pointed out for olopatadine despite higher efficacy than fexofenadine, which is a nonsedating antihistamine (4).
Recently, the sedative effect of olopatadine has been shown in neuropsychological tests to wear off after repeated administration (5). Investigators administered either olopatadine (10 mg/d) or fexofenadine (120 mg/d) in a double-blind manner for more than 6 wk to 42 subjects of 15–64 y old with seasonal pollinosis and found that those who took olopatadine complained of mild sleepiness at 2 wk, with the sleepiness score being significantly higher than that for subjects who took fexofenadine (P < 0.05). However, the sedative effect wore off and the sleepiness scale decreased to the level of fexofenadine after 4 and 7 wk of repeated administration. Although the underlying mechanism of the wear-off phenomenon is not clear, such tolerance has been observed for other antihistamines, including diphenhydramine (6), mequitazine, and dexchlorpheniramine (7).
The H1 receptor can be imaged and its binding potential (BP) evaluated with PET, but the technique has not been applied to the effect of repeated dosing with antihistamine, possibly because of the limited availability of the PET technique and the difficulty in controlling the medication for a certain period from the viewpoint of ethics and compliance. The purpose of the present study was to demonstrate the feasibility of measuring the H1 receptor BP and receptor occupancy using PET with 11C-doxepin after a 4-wk repeated administration of olopatadine and, thereby, to explore the possible mechanism of the wear-off phenomenon. Contrary to our initial expectation, we found a striking reduction in the H1 receptor BP, as reported here.
MATERIALS AND METHODS
Subjects
The study protocol and the informed consent documents were approved by the Ethics Committee of the Institute of Biomedical Research and Innovation, and written informed consent was obtained from every subject.
A total of 17 young Japanese men (age 20–24) with perennial nasal allergy participated in the study. To be included, the subjects had to be male and 20–29 y old, with clinically moderate allergic rhinitis based on the guideline of the Japanese Society of Allergology, a IgE titer score of 2 or higher level for house-dust mites, a history of antihistamine treatment but no current treatment with antihistamine medication, and a visual acuity of more than 0.1. The exclusion criteria were contraindications for MRI, organic brain disease or morphologic brain anomaly, and liver or renal dysfunction.
The entire study schedule is illustrated in Figure 1A. The study was conducted as a single-blind crossover design during the off-season for pollen allergy, and each subject made 5 visits. On the first visit, the subject underwent the screening tests to confirm that he fit the criteria. On the second visit, a baseline PET scan was obtained after administration of a placebo (baseline scan). The subject was administered the placebo every day until the third visit, on which a second PET scan was obtained after a 5-mg single dose of olopatadine (acute scan). Then, the subject was treated with 10 mg/d (5 mg twice a day) of olopatadine for 4 wk (range, 27–33 d; 30 d on average) until the fifth visit. On the fourth visit (interim visit), events were checked and maintenance of compliance confirmed. On the fifth visit, a third PET scan was obtained after another 5-mg dose of olopatadine (chronic scan), with the last dose of the repeated administration having been taken on the previous evening.
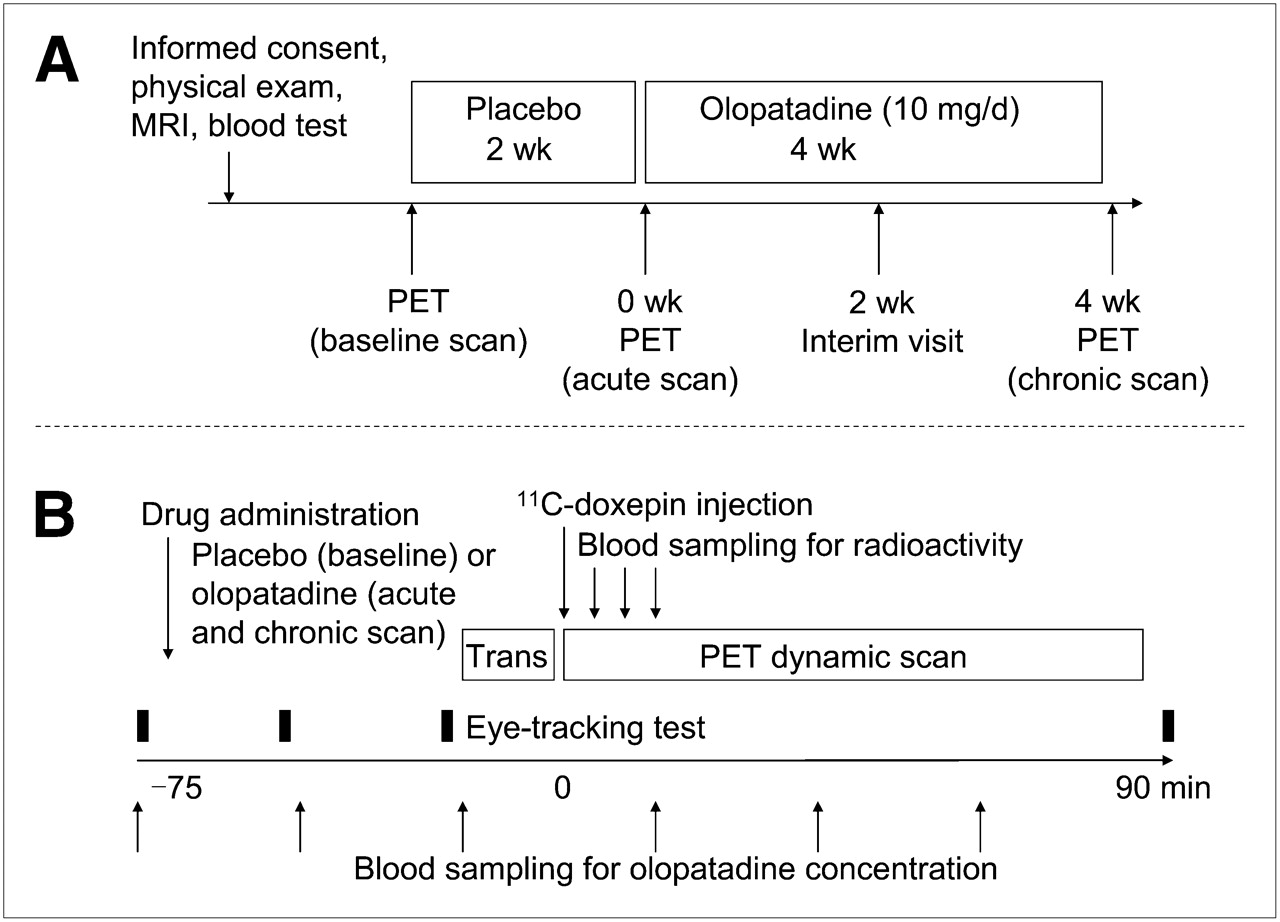
(A) Entire study schedule. (B) PET measurement protocol. Trans = transmission scan.
The subjects were instructed to keep a diary of taking designated drugs during the period (compliance being 93% on average) and were informed of the possible sedative effect of the drug. They were told to refrain from taking any drugs during the study period that might contain antihistamines or that might affect the central nervous system. The subjects were also told not to take any alcoholic drink on the day before the PET scan and not to smoke or take tea or coffee beforehand on the day of the PET scan.
The drugs were prepared by a controller as capsules (Japanese Pharmacopoeia capsule 0) containing either 5 mg of olopatadine or a nonabsorbable intestinal medicine, Biofermin (Biofermin Pharmaceutical Co., Ltd.), which has generally been used as a placebo in the histamine receptor PET studies.
PET Measurement
11C-doxepin was synthesized by 11C-methylation of N-desmethyldoxepin with 11C-methyliodide (8). The radiochemical purity was more than 95%. The injected dose was 770 ± 41 MBq, and the specific activity was 22 ± 4 MBq nmol−1 (21, 22, and 23 MBq nmol−1 are the averages for baseline, acute, and chronic scans, respectively). The preparation and quality control of 11C-doxepin was approved for human use by the PET Radiopharmaceutical Committee of the Institute of Biomedical Research and Innovation.
The PET measurement protocol is illustrated in Figure 1B. The pharmacokinetics data had shown that the time to peak plasma concentration was 60 min for olopatadine administration (9). Because the capsule-dissolving time is 15 min, the PET scan (11C-doxepin injection) was scheduled to start 75 min after the administration of placebo or olopatadine. The subject was positioned in the gantry of the PET camera (ECAT EXACT HR+; Siemens/CTI) with the head fixed in the holder, and after a 10-min transmission scan to acquire data for attenuation correction, a dynamic scan was obtained in 2-dimensional mode for 90 min (4 × 15 s, 7 × 30 s, 3 × 90 s, 7 × 180 s, 6 × 300 s, and 3 × 600 s) after intravenous injection of 11C-doxepin. Venous blood was sampled from the other arm at 5, 10, and 15 min after the injection and was measured for the plasma radioactivity concentration. The images were reconstructed with filtered backprojection with a gaussian filter that provided image resolution of 8 mm in full width at half maximum.
To measure the plasma concentration of olopatadine, we also sampled blood before the administration of olopatadine and at 30, 60, 90, 120, and 150 min afterward. The plasma was frozen and stored for measurement of the olopatadine concentration with liquid chromatography–tandem mass spectrometry at Kyowa Hakko Kogyo Laboratory.
To assess the sedative effect, we performed eye-tracking tests before administration of the drug, 30 and 60 min after administration of the drug (before the PET scan), and 180 min after administration of the drug (after the PET scan). An electronically designed goggle was used (Meditester VOG; Matsushita/Panasonic Electric Works) (10–13). The subject was instructed to track a cross target on a virtual screen 4 m ahead for measurement of saccadic latency. The subject was also asked how sleepy he felt, on a 4-step scale, after he took the drug.
Data Analysis
Quantitative analysis was performed on several representative cortical regions to estimate the BP of 11C-doxepin for each scan. Sets of circular regions of interest 1 cm in diameter were placed along the cortical rims over the dorsolateral prefrontal cortex (DLPFC), frontobasal cortex, temporal cortex, parietal cortex, occipital cortex, and anterior cingulate cortex, as well as in the thalamus and the cerebellum on the baseline scan images of each subject to obtain the time–activity curves for each region. The acute and chronic images were coregistered to the baseline images of each subject to obtain the time–activity curves for the same regions of interest as on the baseline images. The distribution volume ratio was computed from the time–activity curve for each region using Logan graphical analysis with reference region input (14). Cerebellum was used as the reference region because of negligible H1 receptor (15–17). The cerebellar efflux constant was set to be the average of healthy subjects in a previous study (0.022 min−1) (18). BP (as BPND, where ND = nondisplaceable) was computed as distribution volume ratio – 1, and receptor occupancy was computed as 1 – (BPND at acute scan/BPND at chronic scan). When the computed receptor occupancy was negative, zero was assigned. For each region, BPND was compared between the scans using 2-way ANOVA with Fisher's least significant difference (19). Statistical significance was tested with Bonferroni adjustment by a factor of 7 (7 regions).
We also used an alternative approach that was in line with previous investigations. The standard input function of 11C-doxepin from previously obtained normal data was calibrated with the 3-point plasma radioactivity data for each scan of the present study. This calibrated input function was applied as the input function after metabolite correction using the unmetabolized 11C-doxepin fraction data of the population (20). The distribution volume of 11C-doxepin was obtained for each region using Logan graphical analysis with calibrated standard input (21). BP (as BPND) for each region was computed as (distribution volume in the target region/distribution volume in the cerebellum) −1, and receptor occupancy was computed in the same way.
RESULTS
In 3 of the 17 subjects, the plasma concentration of olopatadine rose (arbitrarily above 20 ng mL−1) toward the very end of the PET scan or did not rise at all by 150 min after the drug had been administered in the acute or chronic scan or both. These subjects were thought to have a drug absorption problem or unusual pharmacokinetic behavior and were excluded from the data analysis. For the remaining 14 subjects, the average and SD of the plasma concentration of olopatadine at 0, 30, 60, 90, 120, and 150 min after administration was 0 ± 0, 21 ± 25, 62 ± 28, 46 ± 21, 36 ± 9, and 33 ± 11 ng mL−1, respectively, for the acute scan and 7 ± 8, 28 ± 24, 69 ± 29, 52 ± 13, 41 ± 9, and 35 ± 8 ng mL−1, respectively, for the chronic scan. The area under the curve was 57 ± 16 and 64 ± 14 ng mL−1 h (P = 0.13 by paired t test) for the duration of the acute and chronic scans, respectively.
The latency in the saccadic eye-tracking test was highly variable and did not present statistically significant results (Table 1). At the acute scan, when the subjects first took olopatadine for the study, the saccadic latency showed no significant difference between the preadministration result and the results at 30 or 60 min after the administration. The latent period tended to lengthen at 180 min (42% on average), but the increase was not statistically significant because of large individual variations. However, a mild increase in latency (38%) was also observed for the baseline study at 180 min when the subjects took placebo instead of olopatadine. Similar results were observed for the chronic scan as well. Compared with the acute scan, the chronic scan showed no significant effect of repeated administration on lengthening of latency at 180 min after olopatadine administration. No difference was observed in the latency between rightward and leftward movement.
Saccadic Latency Before and After Administration of Placebo or 5 mg of Olopatadine
The subjective sleepiness scale was also highly variable and did not show any significant difference or tendency between any of the measurements.
Figure 2 represents the PET images of standardized uptake value (tissue activity divided by injected activity per body weight) acquired at 70–90 min after injection, which roughly reflects distribution volume (22), for the baseline, acute, and chronic scans in a typical case. The 11C-doxepin uptake was slightly decreased at the acute scan and was markedly decreased at the chronic scan, compared with baseline.

PET images of standardized uptake value (tissue activity divided by injected activity per body weight) acquired at 70–90 min after injection of 11C-doxepin on representative subject at baseline (placebo), following an initial single dose (acute scan), and following a dose after repeated administration (chronic scan).
When the cerebellar time–activity curves were normalized with injected activity, no significant difference was observed between baseline, acute, and chronic scans, with the area under the curve being 5,571 ± 531, 5,651 ± 483, and 5,632 ± 669 (mean ± SD) Bq mL−1 MBq−1 min, respectively (Supplemental Fig. 1; supplemental materials are available online only at http://jnm.snmjournals.org).
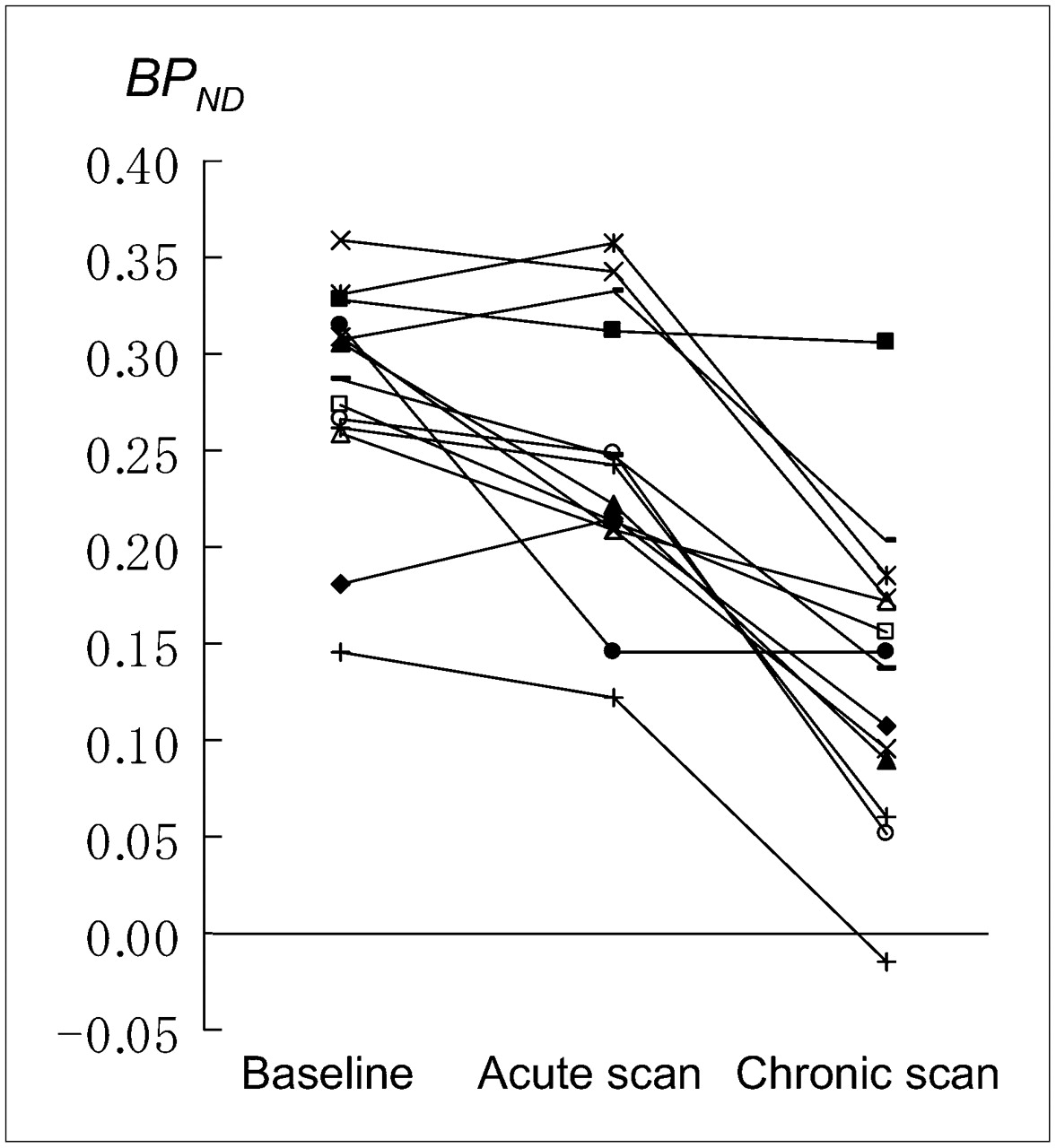
Table 2 summarizes the BPND computed from the Logan graphical analysis with reference tissue input at baseline, acute, and chronic scans for each region of interest, as well as receptor occupancy for the acute scan (results of Logan plot in Supplemental Fig. 2). At the acute scan, the BPND for each region presented a slight to mild decrease from baseline (reduction of 10%−28%, depending on the region; 13% in DLPFC). The receptor occupancy for the acute scan ranged from 11% to 26% (15% in DLPFC). In contrast, the BPND presented a marked and significant decrease at the chronic scan for every analyzed region except thalamus (reduction of 38%−52% from the acute scan; 45% for DLPFC). If computed nominally, the receptor occupancy at the chronic scan would amount to 46%−65% (55% for DLPFC). Figure 3 depicts the BPND for DLPFC cortex as a representative area and its change for each subject. Despite individual variation, the BPND showed a marked decrease from the acute to the chronic scan except for 2 subjects who presented similar BPND values between the two.

BPND of 11C-doxepin in DLPFC of each subject at baseline (placebo), following an initial single 5-mg dose of olopatadine (acute scan), and following another single 5-mg dose after repeated administration of olopatadine for 4 wk (chronic scan).
Histamine H1 Receptor BPND of 11C-Doxepine for the Various Regions Measured with PET at Baseline and After Administration of 5 mg of Olopatadine in Acute and Chronic Scans
When blood-calibrated standard input was used for Logan graphical analysis, similar results were obtained: BPND for DLPFC was 0.31 ± 0.07, 0.26 ± 0.06, and 0.13 ± 0.08 for baseline, acute, and chronic scans, respectively, and receptor occupancy for the acute scan was 15 ± 15.
DISCUSSION
Pharmacologic Considerations
The sedative effect of antihistamines has been effectively evaluated with H1 receptor occupancy using PET with 11C-doxepin under a single dose in healthy subjects (2). The Consensus Group on New-Generation Antihistamines issued a guideline recommending the use of PET for evaluating the sedative effect of newly developed antihistamines (23). The purpose of the present study was to evaluate the effect of repeated administration of olopatadine on the H1 receptor.
The results in Table 2 indicate that BPND was slightly reduced, with receptor occupancy of 15% in the DLPFC cortex under a single dose (acute scan), as is consistent with the previous PET measurement (3). After 4 wk of repeated administration, BPND was dramatically reduced when measured under another dose (chronic scan). According to the report of the phase I study, the plasma olopatadine level drops to below 4% or 7% of the peak concentration at 12 h after single or repeated oral administration, respectively (Fig. S3 of Supplemental Appendix 1) (9). Therefore, the hangover effect on the plasma olopatadine level at the chronic scan should be minimal. In fact, the plasma concentration of olopatadine at the chronic scan was comparable to that at the acute scan with the preadministration level being reduced to the lowest. Therefore, the striking reduction in BPND after repeated administration must be due to some intracerebral change, that is, intracerebral olopatadine accumulation or a change in the H1 receptor itself.
The first interpretation is a possibility that olopatadine has accumulated in the brain after repeated administration to such a level that the receptor is occupied, as revealed in this study. Many drugs may have slower clearance from the brain than from plasma, including risperidone, a dopamine D2 antagonist that showed a much slower decrease in cortical D2 receptor occupancy than in plasma concentration (24). Repeated administration may also cause saturation of P-glycoprotein, of which olopatadine is a substrate (25), and hamper efflux (26). However, a rat experiment using 14C-labeled olopatadine has indicated that the drug concentration in the brain after the 21st daily oral dose of olopatadine (1 mg kg−1 per day) was comparable to the concentration after the initial single dose, reaching a peak of 6.8 versus 6.0 ng Eq g−1 at 2 h, and was reduced to a nondetectable level at 24 h (27). This nonsaturability is understandable, considering that olopatadine is essentially a peripherally acting therapeutic drug. Furthermore, assuming that the amount of H1 receptor and its affinity for olopatadine and 11C-doxepin are constant, receptor occupancy would nominally be as high as 55% for DLPFC if the receptor occupancy were computed simply from the baseline data in the same way as for the acute scan. Such a high receptor occupancy would have resulted in a serious sedative effect, which neither was observed in the present study nor has been reported so far by physicians. Therefore, it is difficult to explain the striking reduction in BPND only by intracerebral accumulation of olopatadine.
An alternative interpretation of the BPND reduction is downregulation (reduction in the total amount) of the H1 receptor. The present results would amount to a reduction of the receptor by 45% after repeated administration, if one assumes constant affinity and receptor occupancy. However, repeated administration of a receptor antagonist in general causes upregulation, not downregulation. Although downregulation of 5-hydroxytryptamine receptor subtype 2 has been reported after repeated administration of the antagonist mianserin on rats (28), no such data have been reported for H1 receptor. In fact, levoprotiline, an antidepressant having an H1 antagonistic effect, was reported to induce upregulation of H1 receptors in the rat (29). There may be an excess release of intracerebral histamine, which may cause downregulation, although no supporting data are available. To reach a conclusion, we need more investigations, including another placebo study after 4 wk of repeated administration.
Although the behavioral data in the present study did not show any wear-off effect, the marked reduction in BPND at the chronic scan may be somehow related to a possible wear-off effect.
Methodologic Issues
The PET techniques have inherent limitations. PET measurement of BP with a radiolabeled ligand is based on the assumption that the BP is constant during the PET measurement period (90 min for this study). However, this assumption is usually not true, because of a possible change in the intracerebral olopatadine concentration caused by the change in the plasma concentration. In the present study, the PET measurement started 75 min after the oral administration. Considering the capsule-dissolving time of 15 min, that timing would correspond to the average time of peak plasma concentration (1 h) in the pharmacokinetics for healthy human subjects (9). It has been a standard procedure in 11C-doxepin PET studies to start the PET measurement at the time of the predicted peak plasma concentration (2). This scheduling is appropriate because the brain concentration is considered to peak somewhat later than the plasma concentration and to remain at the peak for a while, as suggested by the rat data (27).
The input function is another source of error in the estimation of BP and receptor occupancy. Sequential arterial blood sampling with metabolite analysis is an idealistic way to measure BP but is invasive and not practical, especially when the subjects undergo two or more PET scans as they did in the present study. Therefore, Logan graphical analysis with reference input was adopted in the present study. This method requires the cerebellar efflux constant, which was obtained from normal values in the previous reports, assuming it was not influenced by the pharmacologic intervention. An alternative method using calibrated standard input was also adopted so that the results could be compared with previous reports (1,3) that used a similar principle, under the assumption that the shape of the input function is not influenced by the pharmacologic intervention. Both methods provided similar values for BPND. The obtained receptor occupancy value under the initial single dose of olopatadine was 15%—close to the value (14%) reported in the previous study (3) and thus supporting the validity and feasibility of the present study. In fact, the cerebellar time–activity curves showed no significant difference between the scans (Supplemental Fig. 1).
CONCLUSION
A substantial reduction in the histamine H1 receptor BP was observed after repeated administration of the antihistamine olopatadine. This reduction may have been caused either by increased intracerebral olopatadine or by H1 receptor downregulation. The use of PET to evaluate the effect of repeated administration of an antihistamine drug on the H1 receptor is possible and plausible and may be useful for developing antihistamine drugs that are less sedating.
Acknowledgments
This study was financially supported in part by Grant-in-Aid in Scientific Research B 16390350 of the Japan Society for Promotion of Science and by Kyowa Hakko Kogyo Co. Ltd., which is the manufacturer of olopatadine (Allelock). We thank Miho Suzuki and Shusaku Tazawa for acquiring the data, and Jun-ichi Nagase and Masaru Takaishi for coordinating the study.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication September 25, 2008.
- Accepted for publication February 27, 2009.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.