


Abstract
Although several prognostic factors are used to predict recurrence and to select adequate candidates for liver transplantation for hepatocellular carcinoma (HCC), these prognostic factors have some clinical limitations. The purpose of this study was to evaluate 18F-FDG PET as a prognostic factor and to optimize its ability to predict tumor recurrence in liver transplantation for HCC. Methods: The study included a total of 59 HCC patients (45 men and 15 women; mean age ± SD, 56 ± 8 y) who underwent 18F-FDG PET and subsequent orthotopic liver transplantation. All patients were followed up for more than 1 y (mean, 29 ± 17 mo), and recurrence of tumor was monitored. Three PET parameters—maximal standardized uptake value (SUVmax), ratio of tumor SUVmax to normal-liver SUVmax (TSUVmax/LSUVmax), and ratio of tumor SUVmax to normal-liver mean SUV (TSUVmax/LSUVmean)—were tested as prognostic factors and compared with conventional prognostic factors. Results: Among the 3 parameters tested, TSUVmax/LSUVmax was the most significant in the prediction of tumor recurrence, with a cutoff value of 1.15. In a multivariate analysis of various prognostic factors including TSUVmax/LSUVmax, serum α-fetoprotein, T stage, size of tumor, and vascular invasion of tumor, TSUVmax/LSUVmax was the most significant, and only vascular invasion of tumor had additional significance. According to TSUVmax/LSUVmax, the 1-y recurrence-free survival rate above the cutoff was markedly different from the rate below the cutoff (97% vs. 57%, P < 0.001). Conclusion: In this study, 18F-FDG PET was an independent and significant predictor of tumor recurrence. In liver transplantation for HCC, 18F-FDG PET can provide effective information on the prognosis for tumor recurrence and the selection of adequate candidates for liver transplantation.
In early but unresectable hepatocellular carcinoma (HCC), liver transplantation is the best option for radical treatment. Satisfactory results have been reported, with midterm (≥3 y) survival rates of 60%−70% (1–5). However, there is still a considerable rate of therapeutic failure, of which the most common cause is recurrence of tumor (1). Because liver transplantation requires donor organs, which are limited resources, careful patient selection for liver transplantation is required to reduce recurrence and maximize the effectiveness of the limited resources.
Conventional criteria for selecting liver transplantation candidates usually include the size and number of tumors as prognostic factors. The most commonly used criteria are the Milan criteria, in which patients with a solitary tumor no more than 5 cm in diameter or 2 or 3 tumors no more than 3 cm in diameter are recommended as candidates (2). Recently, attempts have been made to expand the Milan criteria to include larger tumors; the UCSF (University of California, San Francisco) criteria include as candidates for liver transplantation those patients who have a single tumor no more than 6.5 cm in diameter or those patients who have 2 or 3 tumors of which the largest diameter is no more than 4.5 cm and the sum of the diameters is no more than 8 cm (6). However, exact evaluation of the size and number of tumors is possible only through pathologic evaluation of the explanted livers. Tumor size and number as evaluated by preoperative radiologic studies have varied considerably from postoperative pathologic results (7,8). Although other factors, such as vascular invasion, tumor grade, and serum α-fetoprotein (AFP), have been proposed as prognostic factors in addition to tumor size and number (4,5,9–11), none of these factors except serum AFP can be evaluated other than by pathologic examination of the explanted livers. Moreover, evaluation of size and number of tumors has now become more complicated because of the increase in preoperative local therapy for tumor control (12).
A recent study performed at our institute suggested that 18F-FDG PET may have a potential role in the prediction of tumor recurrence in liver transplantation (13). Because glucose metabolism assessed on 18F-FDG PET is related to progression or aggressiveness of HCC (14–18), it is feasible that 18F-FDG PET uptake, like size and number of tumors, has prognostic value for tumor recurrence in liver transplantation. However, the appropriate application of 18F-FDG PET or its significance as a prognostic factor has not been investigated in the prediction of tumor recurrence in liver transplantation for HCC.
In this study, we tried to find the most effective prognostic factor on 18F-FDG PET and investigated the value of the prognostic factor in the prediction of tumor recurrence in liver transplantation for HCC.
MATERIALS AND METHODS
Patients and Follow-Up
This study retrospectively enrolled a total of 59 HCC patients (45 male and 14 female) who underwent 18F-FDG PET and subsequent orthotopic liver transplantation (Table 1). Patients who had a previous history of other malignancy were excluded from the study. The mean age (±SD) of the enrolled patients was 56 ± 8 y (range, 33–71 y). All the patients had chronic liver disease associated with viral infection: 54 patients had hepatitis B virus, 4 others had hepatitis C virus, and 1 other had both. Forty-four patients had a history of local treatment, including transarterial chemoembolization (27 patients), percutaneous ethanol injection (5 patients), radiofrequency ablation (4 patients), and a combination of these (transarterial chemoembolization and percutaneous ethanol injection in 6 patients; transarterial chemoembolization and radiofrequency ablation in 2 patients).
Patient Characteristics
Among the 59 patients, living donor liver transplantation was performed on 57 and deceased donor liver transplantation on 2. The donors underwent a thorough work-up to confirm freedom from malignancy, liver disease, and significant infectious disease. All explanted livers were pathologically examined to determine the size, number, T stage, pathologic grade, and vascular invasion of the tumors. The pathologic grade was determined by Edmondson and Steiner's grading system (19), and T stage was determined according to the staging manual of the American Joint Committee on Cancer (20).
All patients were followed up for more than 1 y after liver transplantation, and the mean duration of follow-up was 29 ± 17 mo (range, 12–72 mo). During follow-up, patients were clinically assessed every month, and blood tests (including serum AFP), liver ultrasonography, chest CT, and abdomen CT were performed every 4–6 mo during the first 2 y after liver transplantation. Afterward, the patients were clinically assessed every 3 mo, and diagnostic studies were performed yearly. If the clinical assessment or diagnostic studies showed an abnormal finding, additional studies such as 18F-FDG PET and pathologic confirmation were performed.
18F-FDG PET
18F-FDG PET was performed a mean of 21 ± 21 d (range, 2–115 d) before liver transplantation, using a PET scanner (ECAT Exact; Siemens) or a PET/CT scanner (Gemini; Philips). After fasting for at least 6 h, the patients were injected with 5.2 MBq of 18F-FDG per kilogram of body weight, and images were acquired 1 h later. CT or transmission scanning using an external 68Ge rod source was performed for attenuation correction, and afterward, emission scanning was performed from the skull base to the proximal thigh. Images were reconstructed using an iterative algorithm (ordered-subset expectation maximization).
To evaluate 18F-FDG uptake, we drew regions of interest (ROIs) for the tumor and the normal liver and measured standardized uptake value (SUV) in each ROI. The ROI was drawn to encircle the highest activity of each tumor, with guidance from the CT scans that were acquired from PET/CT or from MRI scans or additional diagnostic images. For normal-liver regions, 3 circular ROIs of about 50 pixels each were drawn, 2 in the right lobe and 1 in the left lobe, at a location where tumor was not detected on other images. All tumor and normal-liver regions were defined by careful correlation with diagnostic CT or MRI scans. The maximum SUV (SUVmax) was measured in each ROI, and mean SUV (SUVmean) was additionally measured in the normal-liver ROI. In the case of multiple tumors, the SUVmax of the tumors was defined as the highest SUVmax of the tumors. The SUVmax of normal liver was defined as the highest SUVmax of the 3 ROIs drawn on normal liver, and the SUVmean of normal liver was defined as the mean value of SUVmean of the 3 ROIs.
Data Analysis
To determine the most effective prognostic factor on 18F-FDG PET, we calculated for each patient the SUVmax of tumor, the ratio of tumor SUVmax to normal-liver SUVmax (TSUVmax/LSUVmax), and the ratio of tumor SUVmax to normal-liver SUVmean (TSUVmax/LSUVmean). The predictive value of each factor for tumor recurrence was determined by analysis of the area under the receiver-operating-characteristic curve. After determination of the most effective prognostic factor on 18F-FDG PET, the predictive value was compared with the predictive values of the conventional prognostic factors, including size, number, vascular invasion, T stage, pathologic grade, serum AFP, and the Milan criteria. The significance of predictive value was analyzed by log-rank testing in univariate analysis and by Cox proportional hazards regression testing in multivariate analysis.
In statistical analyses, groups were compared using Mann–Whitney or χ2 tests, and recurrence-free survival was evaluated by Kaplan–Meier survival analysis. The statistical tests were performed using SPSS (version 15.0; SPSS Inc.) and MedCalc (MedCalc Software). P values of less than 0.05 were considered significant.
RESULTS
Follow-Up of Patients
During follow-up, tumor recurrence was observed in 14 (24%) of 59 patients; 10 in the first year, 3 in the second year, and 1 in the third year after liver transplantation. The 1-y and overall recurrence-free survival rates were 83% and 76%, respectively. Initially detected recurrences involved only the transplanted livers in 2 patients, the transplanted livers and other organs in 8 patients, and only other organs in 4 patients. All liver lesions of the 10 patients, and all extrahepatic lesions of the 4 patients who showed only extrahepatic recurrences (3 in lung and 1 in bone), were confirmed by histopathologic evaluation. The recurrence characteristics of the tumors are summarized in Table 2.
Tumor Characteristics According to Recurrence
Prognostic Factors on 18F-FDG PET and Predictive Values
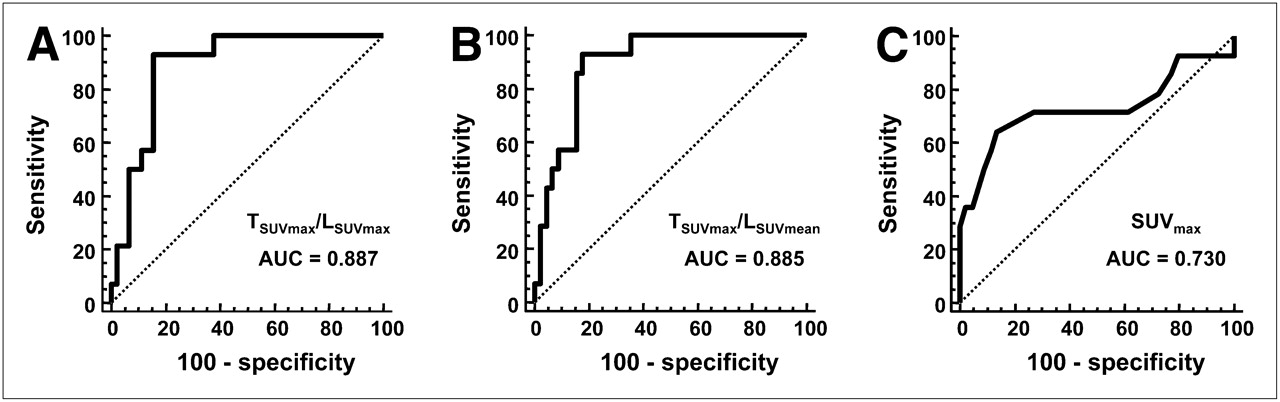
TSUVmax/LSUVmax and TSUVmax/LSUVmean were calculated for all 59 patients, although SUVmax was not measured in 2 patients because of computational problems. The overall SUVmax of tumor was 3.1 ± 1.9, and the overall SUVmax and SUVmean of normal liver were 2.4 ± 0.5 and 2.1 ± 0.4, respectively. On receiver-operating-characteristic curve analysis, TSUVmax/LSUVmax showed the highest area under the curve, 0.887. The areas under the curve of TSUVmax/LSUVmean and SUVmax were 0.885 and 0.730, respectively (Fig. 1). The optimal cutoff values for TSUVmax/LSUVmax, TSUVmax/LSUVmean, and SUVmax were 1.15, 1.35, and 3.0, respectively. From these results, a TSUVmax/LSUVmax of 1.15 was used as the most effective prognostic factor on 18F-FDG PET in the prediction of tumor recurrence. Twenty-one patients showed a TSUVmax/LSUVmax of 1.15 or more, and the other 38 patients showed a TSUVmax/LSUVmax of less than 1.15. Among them, 16 patients showed a TSUVmax/LSUVmax of 1.0 or less.
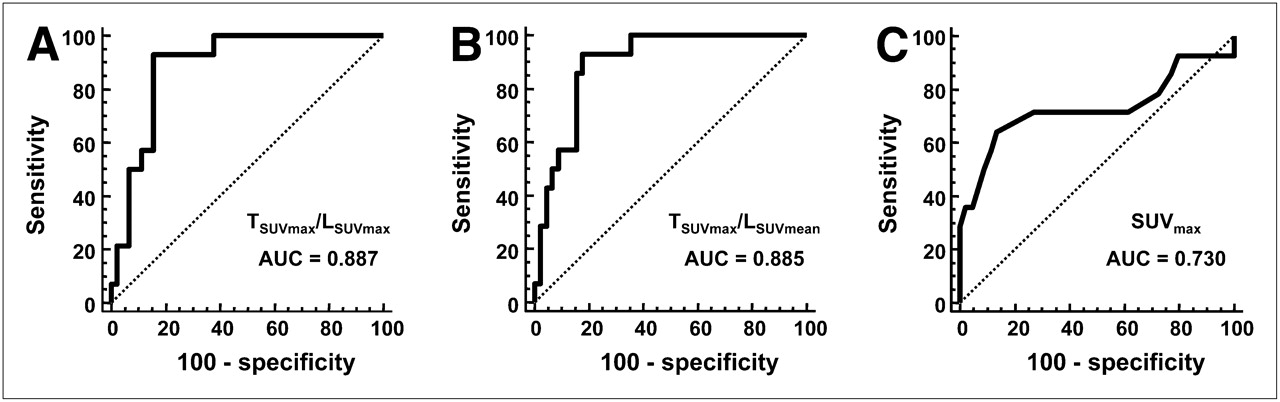
Predictive values of prognostic factors on 18F-FDG PET. TSUVmax/LSUVmax (A) shows highest area under curve on receiver-operating-characteristic curve analysis. TSUVmax/LSUVmean (B) shows similar area under curve, but SUVmax (C) shows significantly lower area under curve.
In the comparison between recurrence and nonrecurrence groups, tumor size, serum AFP, vascular invasion, and TSUVmax/LSUVmax showed significant differences (Table 2). Also, these factors were determined as significant prognostic factors for tumor recurrence in the univariate analysis. However, in the multivariate analysis, only TSUVmax/LSUVmax and vascular invasion were determined to be significant (Table 3).
Significance of Prognostic Factors in Prediction of Tumor Recurrence
Tumor Recurrence According to 18F-FDG PET
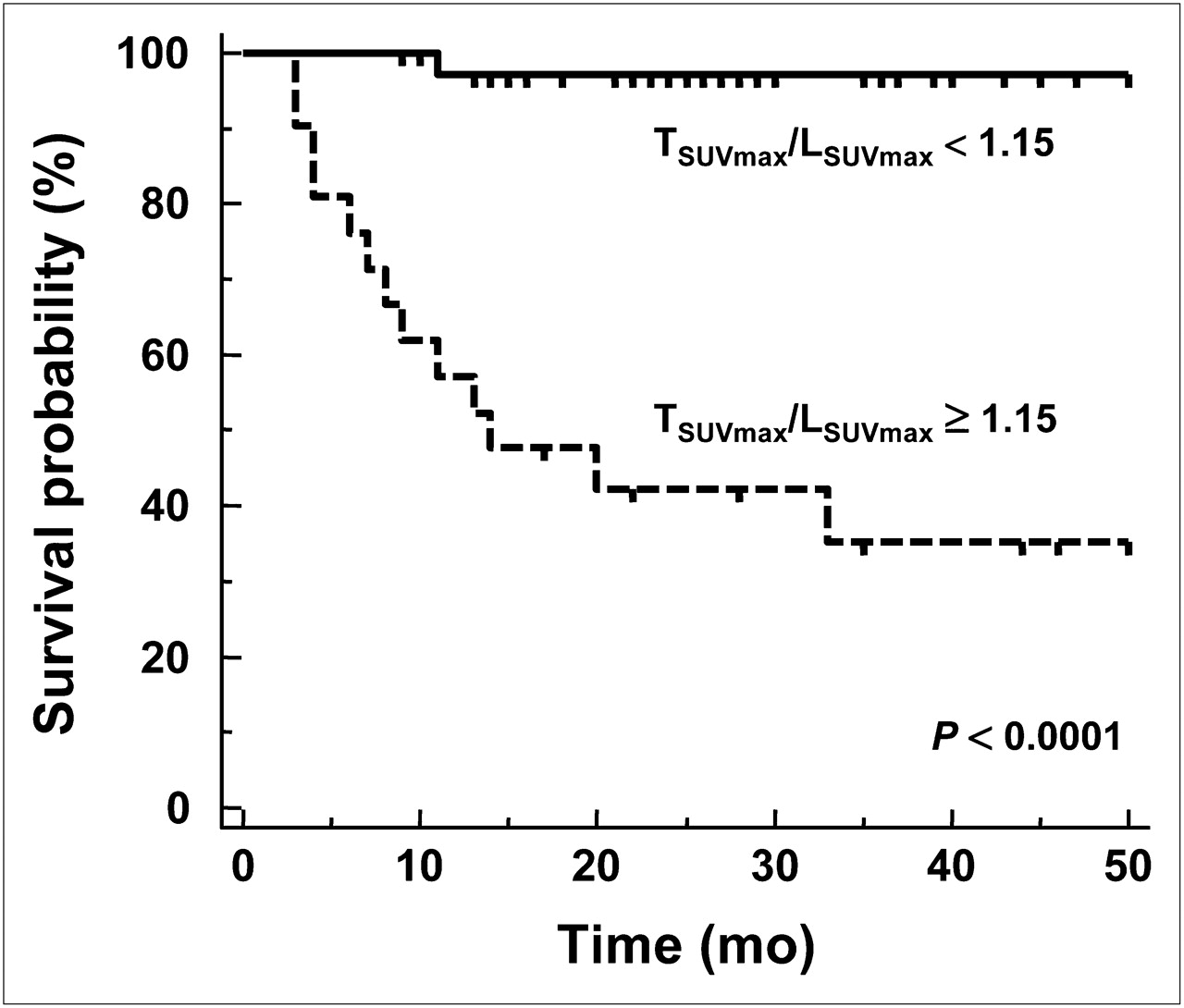
Among the tumor-recurrence patients, 93% (13/14) showed a TSUVmax/LSUVmax of 1.15 or more, whereas just 18% (8/45) of the nonrecurrence patients showed a TSUVmax/LSUVmax of 1.15 or more. Figures 2 and 3 show examples of 18F-FDG PET findings. Recurrence-free survival above and below the cutoff value was significantly different according to TSUVmax/LSUVmax. The 1-y recurrence-free survival rate was 97% for the patients who had a TSUVmax/LSUVmax of less than 1.15 but was 57% in the patients who had a TSUVmax/LSUVmax of 1.15 or more (P < 0.001). The 2-y recurrence-free survival rate was 97% and 42% in each group (P < 0.001, Fig. 4).
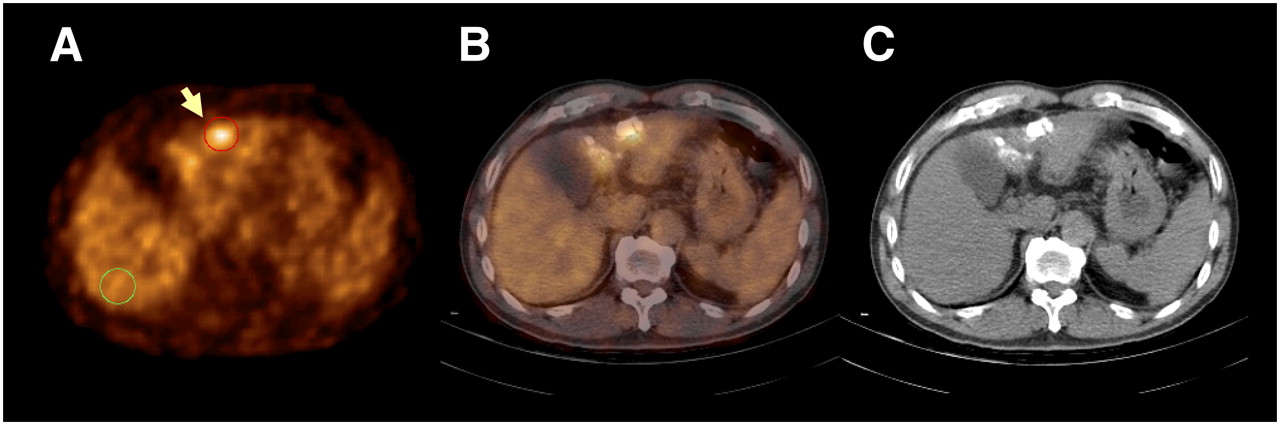
(A) PET, (B) fusion, and (C) CT scans of patient with positive TSUVmax/LSUVmax of 1.62 (arrow). SUVmax of tumor, SUVmax of liver, and SUVmean of liver were 4.20, 2.60, and 2.03, respectively. Red and green circles are examples of drawn ROIs for tumor and liver, respectively. Despite meeting Milan criteria, tumor recurred during follow-up.
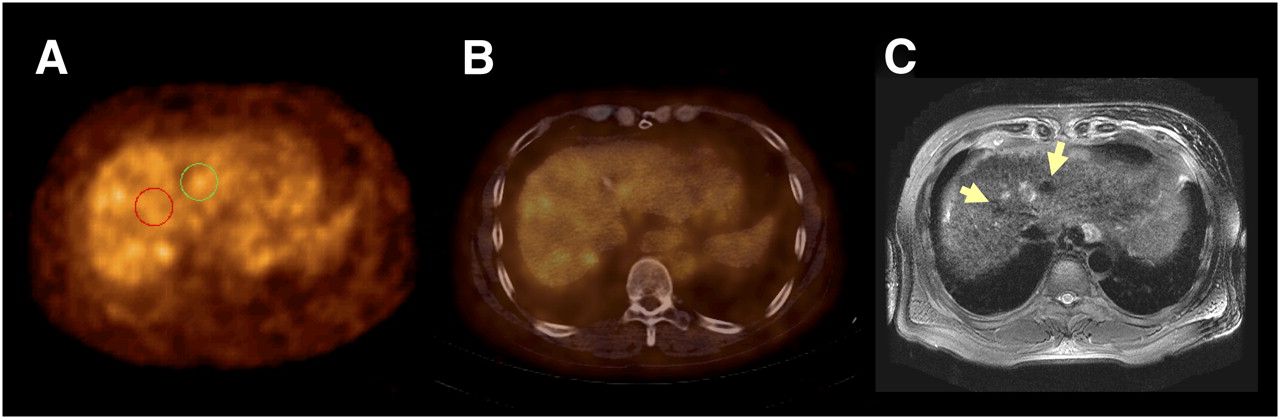
(A) PET, (B) fusion, and (C) MRI scans of patient with negative TSUVmax/LSUVmax of 0.99. SUVmax of tumor, SUVmax of liver, and SUVmean of liver were 2.50, 2.53, and 2.10, respectively. Circles are examples of drawn ROIs for tumors. Case exceeded Milan criteria because of multiple nodules (arrows). However, tumor did not recur during follow-up of 17 mo.

Kaplan–Meier survival analysis according to 18F-FDG PET findings. Patients with TSUVmax/LSUVmax less than 1.15 showed significantly better survival than those with TSUVmax/LSUVmax of 1.15 or more (P < 0.001).
Combining TSUVmax/LSUVmax with vascular invasion (the other significant prognostic factor on multivariate analysis) enhanced the predictive value, whereas combining TSUVmax/LSUVmax with the Milan criteria did not. In patients who showed a TSUVmax/LSUVmax of less than 1.15 and were negative for vascular invasion, there was no recurrence. In contrast, the recurrence rate was 100% in patients who showed a TSUVmax/LSUVmax of 1.15 or more and were positive for vascular invasion. In patients who either had a TSUVmax/LSUVmax of 1.15 or more or were positive for vascular invasion, the recurrence rates were 17%−50% (Table 4).
Recurrence Rate with Combination of Criteria
DISCUSSION
This study demonstrated that 18F-FDG PET is an independent and significant prognostic factor for tumor recurrence in liver transplantation for HCC, with a cutoff TSUVmax/LSUVmax value of 1.15. In a comparison of various prognostic factors by multivariate analysis, 18F-FDG PET was the most significant. According to the TSUVmax/LSUVmax value of each patient, recurrence-free survival rates were markedly different above and below the cutoff value: 97% vs. 57% for 1 y and 97% vs. 42% for 2 y. The results demonstrated prognostic value for 18F-FDG PET in HCC, in addition to diagnostic value.
Although liver transplantation is the best option for early but unresectable HCC, the shortage of donor organs is a major limitation. Even in the case of living donors, selection of candidates for liver transplantation should carefully take into consideration cost, benefit, and especially the safety of donors, in the aspect of medical ethics. To this end, several prognostic factors to predict recurrence of tumor have been investigated and suggested (2,6,9–11). Among them, size and number of tumors were adopted in the most commonly used selection criteria, the Milan criteria (2). The Milan criteria were also adopted to allocate organs for recipients by organ-sharing systems, such as the United Network for Organ Sharing in the United States. In many studies, patients who have met the Milan criteria have had significantly better recurrence-free survival (≤90%), whereas recurrence-free survival has been 40%−60% in patients who exceeded the Milan criteria (2–5).
However, preoperative assessment cannot exactly determine whether a patient meets the Milan criteria, because the exact size and number of tumors can be assessed only by thorough pathologic evaluation of the explanted liver. In the study that originally suggested the Milan criteria, postoperative pathologic evaluation revealed that 27% of patients exceeded the preoperatively determined stage. Recurrence-free survival was 59% in these patients but 92% in patients who were correctly classified as meeting the Milan criteria before liver transplantation (2). Although preoperative diagnosis of the size and number of tumor is performed using conventional radiologic imaging such as CT, MRI, and ultrasonography, it is not so easy to correctly diagnose the size and number of tumors in patients with cirrhotic HCC (7). As a result, a significant discrepancy exists between preoperative radiologic and postoperative pathologic assessments of tumor size and number. In a direct-comparison study, the agreement ratio was as low as 41% between preoperative radiologic and postoperative pathologic staging according to the Milan criteria (8). Furthermore, most of the other potential prognostic factors proposed hitherto, such as tumor grade, T stage, and vascular invasion, have similar limitations as they cannot be exactly assessed on preoperative studies.
18F-FDG PET is a noninvasive, convenient, and feasible tool that now is inevitable in the management of various cancers. In many institutes, 18F-FDG PET has been used to assess extrahepatic metastasis before liver transplantation for HCC (21–23). The present study demonstrated that 18F-FDG PET, in addition to its original purpose, can be an independent prognostic factor in the prediction of tumor recurrence after liver transplantation. In the Milan or UCSF criteria, size and number of tumors are regarded as representative of the progression and aggressiveness of HCC, with the assumption that more progressive and aggressive HCC is prone to recur by microscopic invasion or seeding. Glucose metabolism as assessed on 18F-FDG PET is also a factor related to tumor progression or aggressiveness (14–18). Evident uptake of 18F-FDG has been observed in poorly differentiated HCC (14–17), and a correlation between tumor growth rate and 18F-FDG uptake has also been reported (18). Tumor recurrence after liver transplantation is speculated to result from hematogenous metastasis (24) or undetected preoperative micrometastasis. Although 18F-FDG uptake by primary liver lesions is not a direct indicator of these metastases, the biologic activity of viable cancer cells in primary lesions is represented by 18F-FDG uptake and is deemed to be closely correlated with the probability of metastasis.
As was shown in this study, in 18F-FDG PET of HCC the ratio of tumor uptake to liver uptake is more commonly used as an effective parameter than is SUVmax itself (14–16,18). Uptake of 18F-FDG in HCC is well known to vary with the expression of glucose-6-phosphatase (25). Moreover, most patients who have HCC accompanied by viral infection have underlying liver cirrhosis, which affects glucose metabolism (26), blood glucose level, and tumor uptake of 18F-FDG. Therefore, the tumor-to-liver ratio of SUV is a more commonly used diagnostic factor than is SUV in 18F-FDG PET of HCC patients, as the ratio reflects the underlying variation of glucose metabolism in the liver. The tumor-to-liver ratio of SUV was reported to correlate with the differentiation pattern of HCC and has also been used for diagnosis of HCC (14–16). In a direct-comparison study, the tumor-to-liver ratio of SUV correlated more closely with tumor volume doubling time (a prognostic factor in HCC) than did SUV (18).
Most of the previously reported prognostic factors in liver transplantation were also significant in the present study. In the univariate analysis, serum AFP, T stage, size of tumor, and vascular invasion were determined to be as significant as TSUVmax/LSUVmax. However, in the multivariate analysis, vascular invasion was the only significant factor besides TSUVmax/LSUVmax, the most significant factor. Even the Milan criteria were not so effective in the prediction of tumor recurrence in this study, possibly because of downstaging due to preoperative local therapy. As much as 75% of the enrolled patients had undergone local therapy, including transarterial chemoembolization, radiofrequency ablation, and percutaneous ethanol injection, while awaiting liver transplantation. Although only viable portion–containing nodules were counted and measured in the pathologic review, as is usual (12), it is not easy to assess the size and number of viable portions and to determine whether the Milan criteria were met. Moreover, the prognostic value of the Milan criteria in cases of downstaging by local therapy is still controversial. Although patients who met the Milan criteria by downstaging showed results as good as those of patients who originally met the Milan criteria in one study (27), other studies have had results inconsistent with that study (12,28). However, the results of our study suggest that 18F-FDG PET can be a practical and significant prognostic factor in patient groups complicated by preoperative local therapy.
In our study, most patients underwent living donor liver transplantation, as is usual in Asian countries. Whereas several studies have reported comparable survival rates for living donor and deceased donor liver transplantations (4,5,29), some researchers reported a significantly higher rate of tumor recurrence for living donor liver transplantation (30). This finding is speculated to be related to selection bias (31). Because the waiting time is relatively shorter for a living donor transplant than for a deceased donor transplant, highly aggressive tumors in living donor recipients are less likely to develop to the extent that the person must be dropped from the transplantation waiting list. This speculation also supports the use of 18F-FDG PET as a prognostic factor in living donor liver transplantation, because 18F-FDG PET is expected to show the present biologic activity of cancer cells while the Milan criteria provide just cross-sectional information on the status of tumor progression. Although most of the patients included in this study were living donor recipients, the results may also be applied to deceased donor recipients because the 18F-FDG PET information represents the biologic and metabolic activity of cancer cells in both types of transplantation.
CONCLUSION
The present study demonstrated that 18F-FDG PET is a significant predictor of tumor recurrence in liver transplantation. For an optimal cutoff TSUVmax/LSUVmax of 1.15, recurrence-free survival was significantly different between groups. In the comparison of various factors, TSUVmax/LSUVmax was more significant than any other prognostic factor, even the Milan criteria. Therefore, 18F-FDG PET should be performed in pretransplantation evaluation of HCC not only for detection of extrahepatic metastasis but also for prediction of prognosis.
Acknowledgments
This research was supported by a grant of the Korea Healthcare Technology R&D Project, Ministry for Health, Welfare, and Family Affairs, Republic of Korea (A070001).
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication November 24, 2008.
- Accepted for publication January 27, 2009.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 18F-Fluorocholine PET/CT as an Imaging Biomarker in Patients With Hepatocellular Carcinoma Receiving Atezolizumab Plus Bevacizumab
- 18F-FDG PET/CT Can Predict Survival of Advanced Hepatocellular Carcinoma Patients: A Multicenter Retrospective Cohort Study
- Prediction of Posttransplantation Recurrence of Hepatocellular Carcinoma Using Metabolic and Volumetric Indices of 18F-FDG PET/CT
- 18F-FDG PET and Combined 18F-FDG-Contrast CT Parameters as Predictors of Tumor Control for Hepatocellular Carcinoma After Stereotactic Ablative Radiotherapy
- 11C-Acetate and 18F-FDG PET/CT for Clinical Staging and Selection of Patients with Hepatocellular Carcinoma for Liver Transplantation on the Basis of Milan Criteria: Surgeon's Perspective