


Abstract
The 2 main causes of primary aldosteronism (PA) are aldosterone-producing adenoma (APA) and idiopathic adrenal hyperplasia (IAH). Dexamethasone-suppression 131I-6β-iodomethyl-19-norcholesterol (NP-59) adrenal scintigraphy can assess the functioning of the adrenal cortex. This study evaluated the diagnostic usefulness of NP-59 SPECT/CT in differentiating APA from IAH and in predicting postadrenalectomy clinical outcome for PA patients who had inconclusive adrenal venous sampling (AVS) and CT results. Methods: We retrospectively reviewed the 31 adrenal lesions of 27 patients (age range, 33–71 y; mean age ± SD, 50.4 ± 10.9 y) who had been clinically confirmed (by saline infusion and captopril tests) to have PA, had inconclusive CT and AVS test results, and had undergone NP-59 imaging before adrenalectomy. The accuracy of NP-59 imaging was determined by comparison with histopathologic findings. Results: NP-59 SPECT/CT gave us 18 true-positive, 3 false-positive, 6 true-negative, and 4 false-negative results. Compared with planar imaging, SPECT/CT significantly improved diagnostic accuracy and prognostic predicting ability (P = 0.0390 and P = 0.0141, respectively). The NP-59 results were negative for 7 of the 23 patients with unilateral adrenal lesions, and none of these 7 patients had shown postsurgical clinical improvement. Conclusion: NP-59 SPECT/CT is an effective imaging tool for differentiating APA from IAH in PA patients whose CT and AVS results are inconclusive. Our results suggest that patients with presurgically negative NP-59 results should be treated medically and that noninvasive NP-59 SPECT/CT may be suited for use as the first lateralization modality after CT in patients with clinically confirmed PA.
Hypokalemia and refractory hypertension usually lead to an increased likelihood of primary aldosteronism (PA), which is the most common cause of secondary hypertension. The prevalence of PA among hypertensive patients has been reported to range from 1% to 20% (1). The main causes of PA are aldosterone-producing adenoma (APA) and idiopathic adrenal hyperplasia (IAH). Unilateral laparoscopic adrenalectomy is usually the treatment of choice for patients with APA, whereas patients with IAH are normally treated with medicines (2–4).
Radiologic imaging modalities such as CT or MRI, via detecting abnormally large adrenal glands, are currently the default imaging tools for diagnosing APA. However, the diagnostic performance of CT (sensitivity, 40%−100%) and MRI (sensitivity, 70%−100%) has been reported to vary widely (5). This deficiency of CT and MRI may be attributed to the fact that hormonal hyperfunction may not be directly inferred from the presence of a nodule; small APAs may exist in normal-appearing adrenal glands, and bilateral nodularity may not be interpreted as bilateral APA or IAH (6,7). Furthermore, IAH adrenal glands may be noted as nodular changes on CT or MR images, hence leading to unnecessary adrenalectomy (8). Thus, it does not appear that CT or MRI findings alone are sufficiently reliable to differentiate APA from IAH.
The assessment of physiologic functioning by adrenal venous sampling (AVS) leads to a better diagnosis (8,9). It is now widely accepted that AVS provides the best lateralization for PA etiology (9). However, occasionally the AVS results are inconclusive or contradict the CT results. Under these circumstances, adrenal scintigraphy with 131I-6β-iodomethyl-19-norcholesterol (NP-59), as demonstrated in this study, may be used as a supplementary diagnostic tool.
Dexamethasone-suppression NP-59 scintigraphy has been used for imaging the adrenal cortex since 1975 (10,11). NP-59 is known to be a marker of adrenocortical cholesterol uptake and can serve as a probe of adrenal cholesterol metabolism. Hence, NP-59 imaging uptake may be used to assess the adrenal cortex spatially and functionally. Administering dexamethasone, which suppresses adrenal cortical hormones, markedly improves the diagnostic usefulness of adrenal scintigraphy (12,13). In 3–5 d after NP-59 administration with this suppression, normal adrenal glands generally do not take up a detectable amount of tracer. Unilateral adrenal uptake on NP-59 scintigraphy most likely indicates APA, but bilateral, simultaneously symmetric uptake is usually attributed to IAH instead of APA (10,11).
NP-59 scintigraphy, being limited by the resolution of planar scintigraphy, has had a reported sensitivity of as low as 47% for localizing APA (14). The technology of SPECT significantly improves the resolution of scintigraphy. In addition, the integrated SPECT/CT system is capable of localizing the adrenal glands with greatly enhanced precision.
This study evaluated the diagnostic usefulness of NP-59 SPECT/CT in differentiating APA from IAH and in predicting postadrenalectomy clinical outcome for PA patients who had inconclusive AVS and CT results.
MATERIALS AND METHODS
Patients
We retrospectively studied the 31 adrenal lesions of 27 patients (11 men and 16 women; age range, 33–71 y; mean age ± SD, 50.4 ± 10.9 y) from the Taiwan Primary Aldosteronism Investigation (TAIPAI) database. Between July 2002 and September 2007, these 27 patients had been clinically confirmed (by saline infusion and captopril tests) to have PA (15), had inconclusive abdominal contrast-enhanced CT (CECT) and AVS test results, and had undergone NP-59 imaging studies before surgical intervention. During the study period, 24 patients had been diagnosed with negative NP-59 results and did not undergo adrenalectomy; these patients were not included in this study. All 27 study patients had undergone CECT, and 8 had also undergone AVS before NP-59 imaging. NP-59 studies had been ordered for these 27 patients for several reasons: inconsistent AVS and CT results (patients 1, 5, 12, 18, and 21); consistent AVS and CT results in patients who had tiny lesions (patient 23), multiple nodular lesions (patient 13), or bilateral lesions (patient 24) on CT; and unsuccessful AVS or unavailable AVS results (the remaining 19 patients). The characteristics of these 27 patients and their 31 adrenal lesions (22 APA and 9 IAH) are listed in Table 1.
Patient and Lesion Characteristics
Patient Preparation Before NP-59 Imaging
Patients taking glucocorticoids, diuretics, spironolactone, β-blockers, calcium channel blockers, or α-blockers as antihypertensive medications had been switched to other antihypertensive agents for 3 wk before their NP-59 studies (12). For 3 d before and 5 d after the NP-59 intravenous injection, each patient took 8 mg of oral dexamethasone daily in divided doses to suppress normal adrenal uptake of NP-59 and 1 mL of diluted Lugol solution daily to block thyroidal uptake of free 131I (13). To reduce the intestinal background activity of radiocholesterol, each patient also took mild laxatives every night before NP-59 imaging.
NP-59 Planar Imaging and SPECT/CT
Each patient received a slow intravenous injection of 37 MBq (1 mCi) of NP-59. Both anterior and posterior planar images for each patient were taken 72 h after tracer injection. If any focal lesion was noted on the 72-h planar images, SPECT/CT was performed subsequently. Each patient also underwent repeated anterior and posterior planar imaging followed by SPECT/CT 96 h after tracer injection. Furthermore, each patient underwent final anterior and posterior planar imaging 120 h after tracer injection.
The planar and SPECT/CT images of the lumbar region were taken using a dual-head SPECT/CT γ-camera (Hawkeye; GE Healthcare) equipped with medium-energy, general purpose, parallel-hole collimators. The energy window was set at the 364 (±10%) keV peak of 131I. Planar images were acquired at a rate of 20 min per image and were stored in 256 × 256 matrices. The average counts per image were 1,000,000 for 72-h, 800,000 for 96-h, and 700,000 for 120-h images. SPECT/CT was performed using 60 projections over a circular orbit of 360° (40 s/angle), and the data were stored in 128 × 128 matrices. Transmission CT was performed after the emission acquisition, using 140 kVp, 2.5 mA, a slice time of 13.84 s, and a slice step of 10 mm. Emission data were reconstructed iteratively with CT-derived attenuation correction using ordered-subsets expectation maximization.
Image Interpretation
The CECT images for each patient were interpreted by a single radiologist who was experienced in adrenal imaging and did not know the patient's NP-59 and pathologic results. Each gland was then categorized as being normal, being hyperplastic, or having a nodule.
The NP-59 planar, SPECT, and SPECT/CT images were reviewed by 3 experienced nuclear medicine physicians without knowledge of the patient's pathologic results. Each patient's NP-59 images were examined on the review station of the manufacturer (Xeleris; GE Healthcare) in the following order: first planar, then SPECT, and finally SPECT/CT. In the SPECT/CT interpretation, both CT and fused SPECT/CT images were studied for better localization of the adrenal gland.
For visual interpretation of adrenal uptake on NP-59 images, a 5-point visual scale was used—0, no uptake; 1, faint uptake less than or equal to that in the liver; 2, bilaterally symmetric uptake mildly greater than that in the liver; 3, focal unilateral or asymmetric uptake greater than that in the liver; and 4, intense unilateral or asymmetric uptake significantly greater than that in the liver. An adrenal lesion was considered APA if its visual scale was 3 or 4.
Adrenalectomy and Pathologic Correlation
All 27 patients underwent laparoscopic adrenalectomy via the lateral transperitoneal approach (16) by an experienced surgeon less than 3 mo after the completion of the NP-59 scintigraphy. Twenty-three patients underwent unilateral adrenalectomy because of consistent diagnostic results from 2 or more lateralization modalities (15 patients) or poor medical control (8 patients). Four patients underwent bilateral partial adrenalectomy because of bilateral NP-59 uptake (patient 24) or unilateral NP-59 uptake with CT showing obvious nodules (20, 20, and 10 mm for patients 25, 26, and 27, respectively) in the contralateral adrenal gland. All 27 patients had been clearly informed of the risks and benefits of their surgical procedures and gave written consent. None had intraoperative complications, conversions, or reoperations, and none died. Each surgical specimen was then evaluated by an experienced pathologist (15). The accuracy of NP-59 planar and SPECT/CT images was determined in accordance with the corresponding histopathologic results.
Outcome Evaluation
All patients were followed up postsurgically by PA specialists. Blood pressure and the levels of serum aldosterone, renin, and potassium were checked periodically. Postadrenalectomy clinical outcomes were judged on the basis of improvement of hypertension and hypokalemia (17). Hypertension was considered cured if blood pressure decreased to 140/90 mm Hg or less shortly after adrenalectomy and antihypertensive medications were not required during the first year after adrenalectomy (18). Patients whose hypertension subsided within the first year but later returned were still classified as cured. Hypokalemia was considered resolved if serum potassium levels remained normal without potassium supplementation.
Statistical Analysis
All data are expressed as mean ± SD. To compare the diagnostic accuracy of the imaging modalities, we performed receiver-operating-characteristic curve analysis. The area under the curve (AUC) for each modality was calculated and compared statistically. A result was deemed statistically significant if the P value was less than 0.05. This statistical analysis was performed using Stata software (version 8; Stata Press) for Microsoft Windows.
RESULTS
Pathologic examination showed that 14 of the 27 patients had unilateral APA, 9 had IAH, and 4 had bilateral APA.
Diagnostic Accuracy
NP-59 planar imaging produced 9 true-positive, 3 false-positive, 6 true-negative, and 13 false-negative results; NP-59 SPECT produced 15 true-positive, 3 false-positive, 6 true-negative, and 7 false-negative results; and NP-59 SPECT/CT produced 18 true-positive, 3 false-positive, 6 true-negative, and 4 false-negative results. Table 2 cross-references the CECT, NP-59 planar, NP-59 SPECT, and NP-59 SPECT/CT results relative to the pathologic results. The respective sensitivity, specificity, positive predictive value, negative predictive value, accuracy, and AUC of each imaging modality are listed in Table 3. The CECT results for the selected patients in this study were not a faithful representation of the diagnostic effectiveness of CECT in typical PA patients. Patients with a definite diagnosis of CECT and AVS usually began medical or surgical treatment immediately thereafter and, in general, would not require NP-59 scanning for further diagnosis.
CECT and NP-59 Results Relative to Pathologic Results
Statistical Results for CECT and NP-59 Imaging in Diagnosing Lesions and Predicting Postsurgical Improvement
Table 3 shows that SPECT (AUC, 0.6742; SE, 0.0976) and SPECT/CT (AUC, 0.7424; SE, 0.0934) are more accurate than planar imaging (AUC, 0.5379; SE, 0.0991) in the detection of adrenal adenoma (the P value for SPECT/CT [0.0390] is statistically significant whereas that for SPECT [0.1575] is not).
NP-59 SPECT/CT correctly identified 18 adenomas (average size, 15.1 ± 5.2 mm; range, 6−24 mm) in 17 patients. Of these 18 adenomas, 9 were not detected on planar images (mean size, 12.0 ± 4.5 mm; range, 6–18 mm), and 3 were not detected on SPECT images (mean size, 9.3 ± 3.2 mm). Figure 1 shows a 6-mm adrenal adenoma that was missed on planar imaging but was detected on SPECT and SPECT/CT.

A 45-y-old man (patient 3) with initial presentation of refractory hypertension and hypokalemia, whose planar imaging findings were false-negative for adrenal lesions but whose SPECT and SPECT/CT findings were true-positive. (A) Abdominal CECT shows equivocal lesion in left adrenal gland (arrow). (B) Planar image obtained 96 h after NP-59 injection shows no definite tracer uptake in either left or right adrenal region (visual scale, 0). (C) Focal hot spot (visual scale, 4) is well demonstrated in SPECT/CT images. Left adrenalectomy was performed, and pathologic examination revealed 6-mm adenoma. Patient's hypertension persisted after surgery.
Four APA lesions were false-negative on planar, SPECT, and SPECT/CT NP-59 imaging. Three of these four occurred in 3 patients with bilateral APA. For these 3 patients, the left APA was true-positive and the right APA was false-negative on SPECT/CT. Planar imaging and SPECT failed to identify the 2 subcentimeter left APAs in 2 of these 3 patients (Fig. 2). Three false-positive lesions were detected on SPECT and SPECT/CT, but 1 turned out to be true-negative on planar imaging (a 6-mm nodular hyperplasia lesion). Only 1 of the 4 patients with bilateral adenoma showed bilateral uptake (Fig. 3).
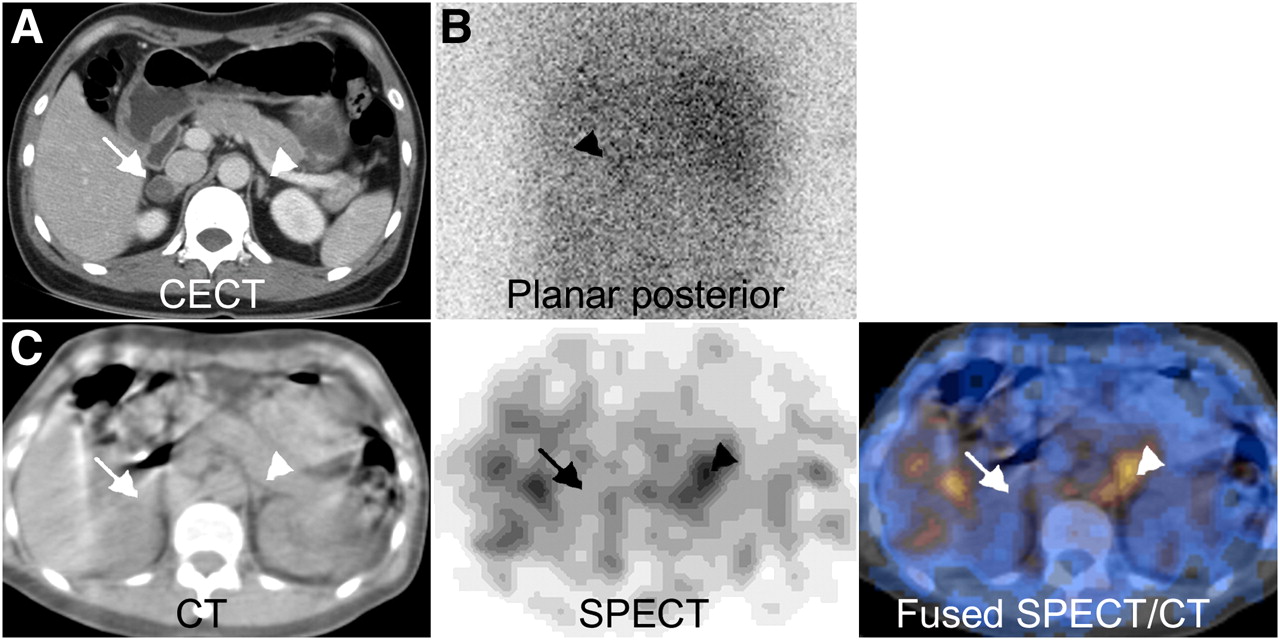
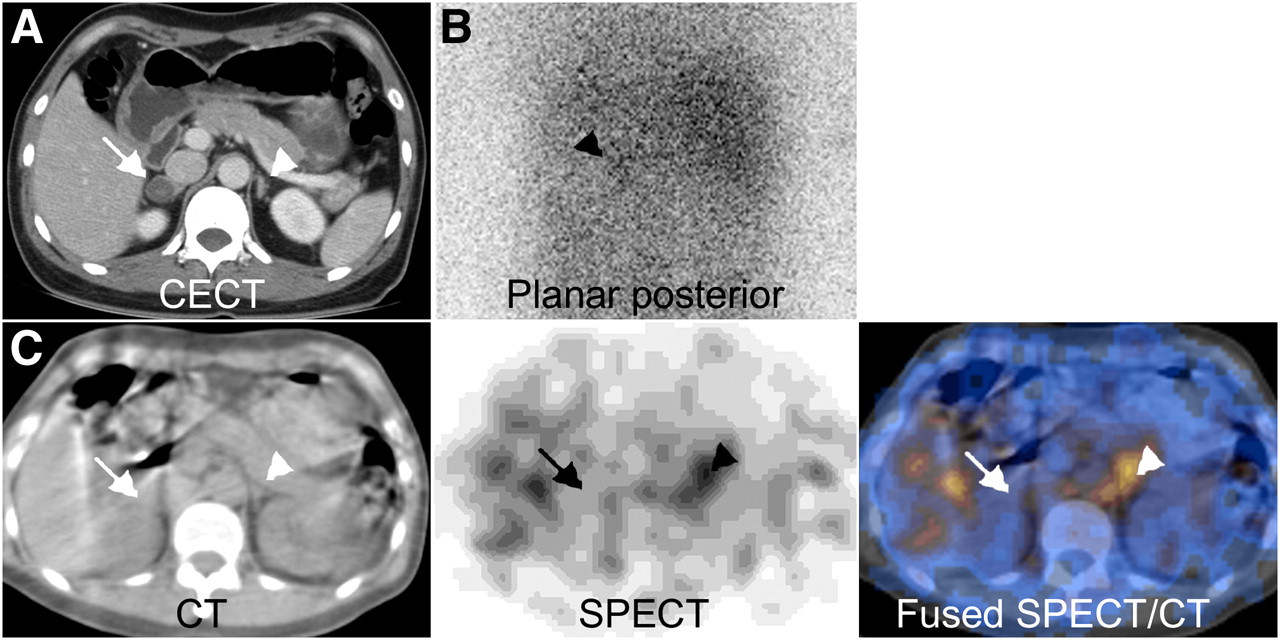
A 66-y-old woman (patient 26) with hypertension and intermittent tachycardia due to bilateral APA, whose left adrenal lesion was false-negative on planar imaging and SPECT but true-positive on SPECT/CT and whose right adrenal lesion was false-negative on all 3 imaging methods. PA was diagnosed on the basis of serum potassium level of 3.2 mmol/L (reference range, 3.5–5.3 mmol/L) and serum aldosterone level of 76.6 ng/dL (reference range, 5–30 ng/dL). (A) CECT shows 2.0-cm well-defined nodular lesion in right adrenal gland (arrow) and minimal nodular change in left adrenal gland (arrowhead). (B) NP-59 96-h planar posterior image shows faint tracer uptake in left adrenal region (arrowhead; visual scale, 1). (C) SPECT/CT shows clear hot spot in left adrenal gland (arrowheads; visual scale, 4). Although no radiocholesterol uptake on right side (arrows) was noted, obvious nodule on right side was detected with CECT. Bilateral adrenalectomy was performed, and pathologic examination revealed bilateral adenoma. Patient's aldosterone-renin ratio, hypokalemia, and blood pressure returned to normal after surgery.
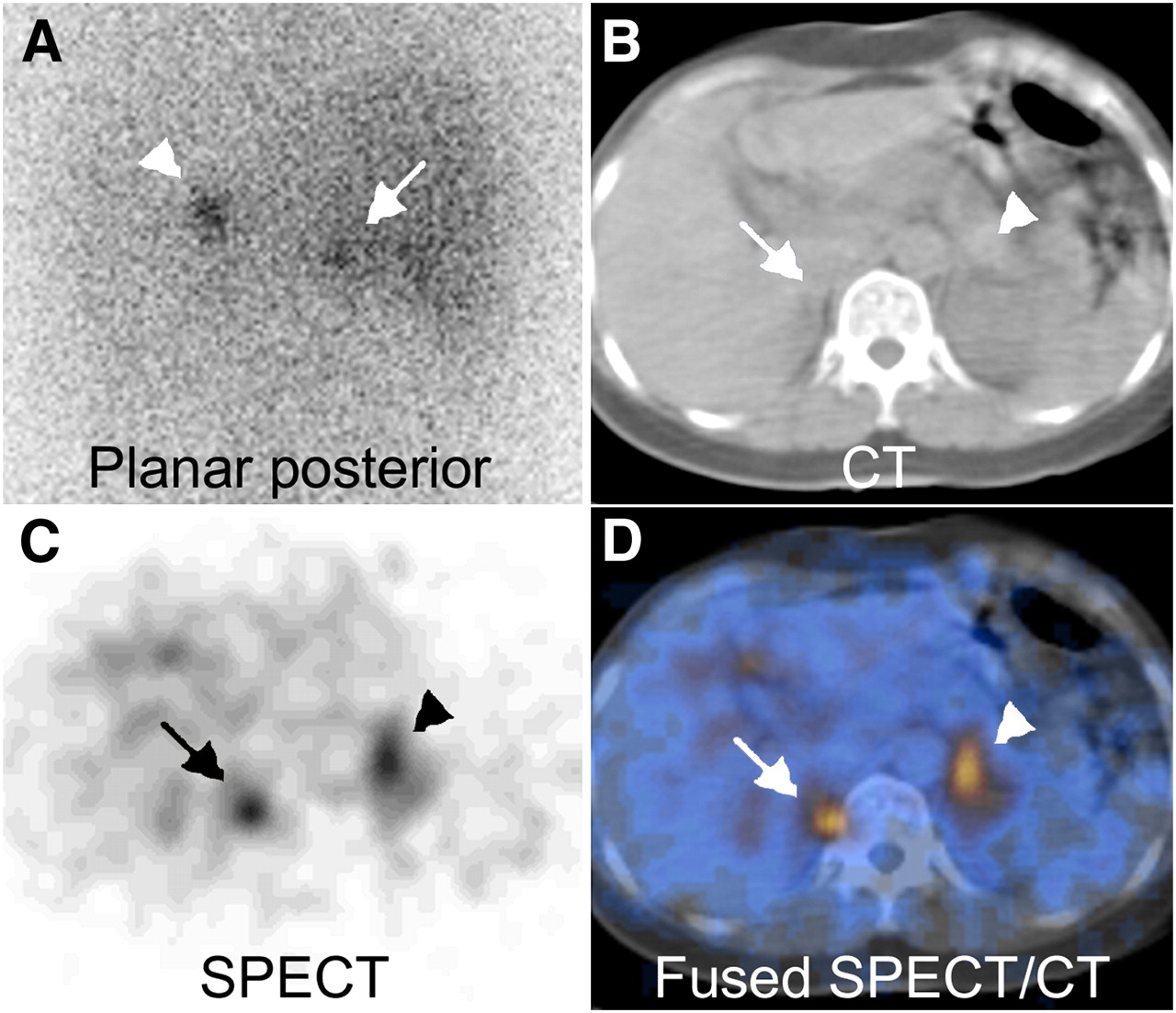
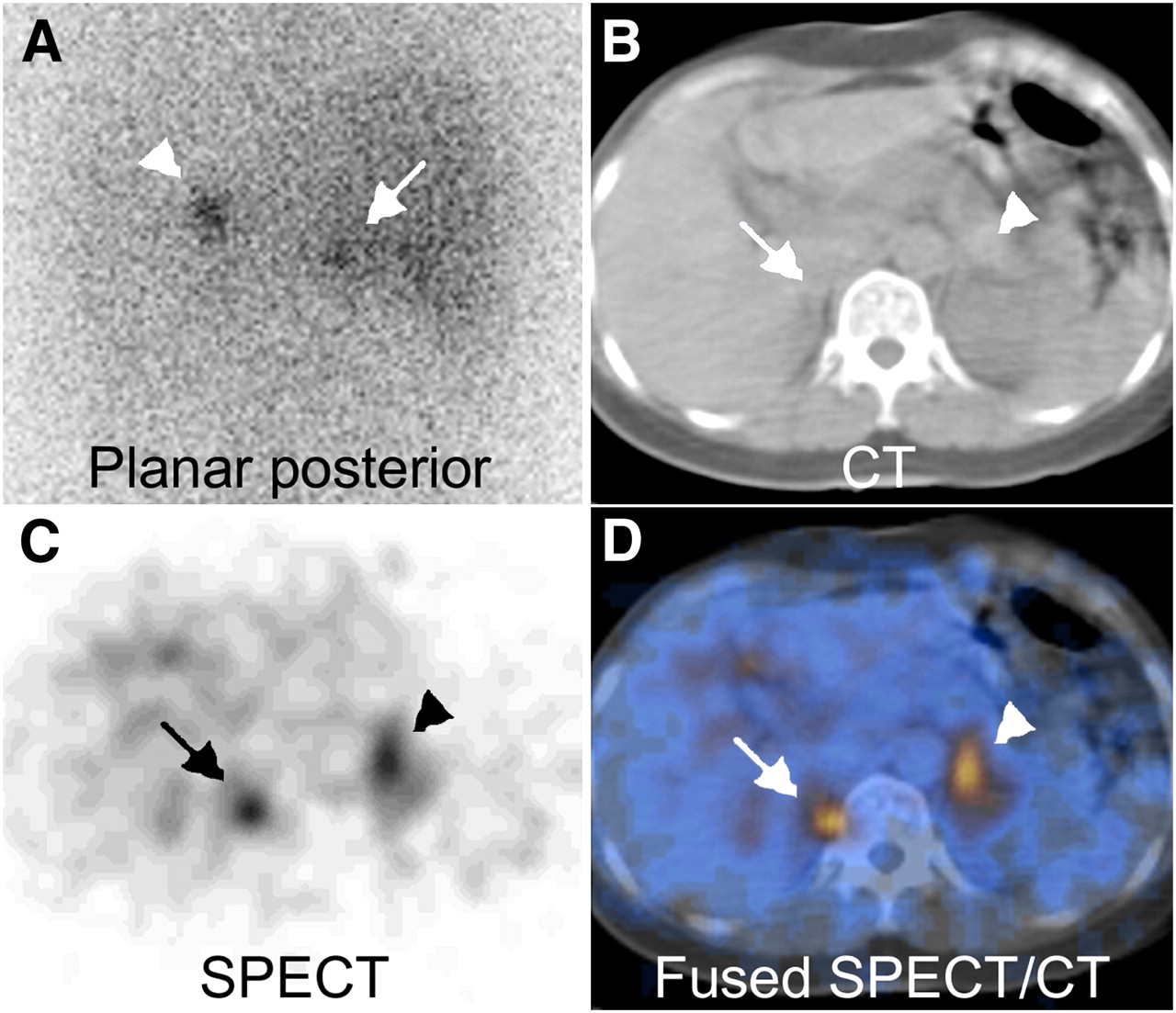
A 46-y-old woman (patient 24) with hypertension for more than 10 y due to bilateral APA, whose planar, SPECT, and SPECT/CT findings were true-positive for bilateral adrenal lesions. PA was diagnosed on the basis of hyperaldosterone level (700 ng/dL; reference range, 5–30 ng/dL). CECT showed 1.5-cm nodular lesion in right adrenal gland and 1.8-cm nodule in left adrenal gland. (A) NP-59 96-h planar posterior image shows bilaterally intense and symmetric uptake in adrenal region (visual scale, 4). (C and D) SPECT (C) and SPECT/CT (D) also show bilateral hot spots in adrenal gland (visual scale, 4). Bilateral adrenalectomy was performed, and pathologic examination revealed bilateral adenoma. Patient's aldosterone-renin ratio, hypokalemia, and blood pressure returned to normal after surgery.
NP-59 Results and Clinical Outcome
Thirteen of the 18 APA patients (72%) demonstrated postsurgical improvement of blood pressure, serum potassium level, or aldosterone level. In contrast, only 1 of the remaining 9 IAH patients (11%) showed postsurgical improvement of blood pressure, hypokalemia, or hyperaldosterone (Table 1).
Cross-referencing of the CECT, NP-59 planar imaging, NP-59 SPECT, and NP-59 SPECT/CT results relative to postsurgical clinical improvement in the 23 patients with unilateral adrenal lesions is shown in Table 4. The respective sensitivity, specificity, positive predictive value, negative predictive value, accuracy, and AUC of each imaging modality are listed in the lower compartment of Table 3, which shows that NP-59 SPECT/CT has the best predictive ability.
CECT and NP-59 Results Relative to Clinical Outcome After Adrenalectomy
For 17 of the 23 patients with unilateral adrenal lesions, the postsurgical clinical outcome was consistent with the presurgical NP-59 SPECT/CT results (74%, Table 3). Sixteen of the 23 patients showed unilateral NP-59 uptake, and 10 of these 16 (62.5%) showed postsurgical improvement. None of the 7 patients with negative NP-59 SPECT/CT results showed postsurgical clinical improvement.
NP-59 SPECT/CT Lateralization Results and Clinical Management
Of the 27 patients in this study, 19 had a unilateral concentration of NP-59 on SPECT/CT, 1 had a bilateral concentration, and 7 had no concentration. If we adopt the criterion that unilateral NP-59 uptake calls for unilateral adrenalectomy, the 13 patients with unilateral APA would have received the appropriate treatment (68%) but the 3 patients with bilateral APA would not have received optimal treatment and the 3 patients with IAH would have received unnecessary adrenalectomy.
If we adopt the additional guideline that medical treatment without adrenalectomy is applied for a patient with bilateral uptake or no uptake on NP-59 SPECT/CT, 6 IAH patients would have received the appropriate treatment (75%) but one patient with unilateral APA and another with bilateral APA would not have received optimal treatment. In total, 19 of 27 patients (70%) would have received the appropriate treatment if based on the NP-59 SPECT/CT results.
DISCUSSION
PA is now recognized as the most common form of secondary hypertension and is potentially curable (1). Cardiovascular complications have been shown to occur significantly more often in PA patients (19). Accurate identification and early intervention of APA may help to avoid excessive cardiovascular damage due to prolonged hyperaldosteronism (19). After PA has been initially suggested by clinical and biochemical features, subtype evaluation is usually performed via anatomic imaging (CT or MRI) and AVS. Nevertheless, AVS may be unavailable occasionally, or the AVS result may be inconclusive or inconsistent with CT findings. Under these circumstances, NP-59 scintigraphy is an ideal noninvasive test that may be explored to diagnose APA.
Dexamethasone-suppression NP-59 scintigraphy has the ability to localize APAs with excessive hormone production. But the accuracy of differentiating adenoma from hyperplasia by NP-59 scintigraphy varies from 47% to 94% in the published data (11,20–25) from studies in which planar imaging was used. The resolution limit of planar imaging may prevent the detection of small lesions, and adenomas less than 1.5 cm in diameter may not be visible on planar scintigraphy (26). This deficiency may be remedied by SPECT, which bears better contrast and improves image resolution. NP-59 SPECT has been suggested to be useful in evaluating the functional status of adrenal cortical lesions (27,28). Nevertheless, the lack of anatomic landmarks may cause gastrointestinal or gallbladder activity to be misinterpreted as hyperfunctioning adrenal adenoma.
The integrated SPECT/CT system provides both functional and anatomic information. The fact that NP-59 activity may be mapped anatomically on SPECT/CT fused images is helpful in preventing misidentification of gastrointestinal activity as adrenal uptake and improves the specificity of NP-59 scanning. SPECT/CT is also capable of localizing small foci of activity in the adrenal gland and hence improves sensitivity. In this study, 12 of 22 adrenal adenomas were 1.5 cm or smaller. Ten of these 12 small lesions (83.3%) were discovered and identified on SPECT/CT images.
On the other hand, NP-59 scintigraphy requires additional preparation, in contrast to ordinary nuclear medicine studies. Concurrent antihypertensive medications that may affect NP-59 accumulation should be withdrawn for a sufficient period before the scanning (12). Furthermore, the dose and duration of dexamethasone suppression must be sufficient to inhibit uptake by normal adrenal glands during a 3- to 5-d period after NP-59 injection (13). Another major disadvantage of a NP-59 study is the requirement for multiple imaging sessions during the prolonged interval after NP-59 injection. Planar images are normally acquired on days 3, 4, and 5 after tracer injection. One study has suggested that data acquisitions of SPECT, which has better resolution than planar imaging, may be required only on day 3 or 4 after tracer injection (29). It turns out that this assertion is validated by the results of our study.
Three of the 9 IAH patients were diagnosed with unilateral NP-59 uptake, which was found to correspond pathologically to 1 case of hyperplasia and 2 of nodular hyperplasia. Only 1 of these 3 patients showed an improvement of clinical outcome after adrenalectomy. The 33% false-positive interpretations for IAH patients in this study seem to imply some disadvantage to NP-59 imaging.
Patients with bilaterally hyperfunctioning adenomas are rare. Only a few cases have been reported (15,30). In this study, only 1 of the 4 patients with confirmed bilateral adrenal adenoma had bilateral NP-59 uptake. The NP-59 results for the other 3 patients with bilateral adrenal adenoma were true-positive for the left adrenal adenoma and false-negative for the right one. Since pathologic results alone are not capable of differentiating functioning from nonfunctioning adenomas, these 3 patients might in fact have had left aldosteronomas but nonfunctioning right adenomas despite the bilateral adenomas indicated on the pathologic reports.
Finally, we would like to call attention to the fact that none of the NP-59–negative patients in this study showed postsurgical clinical improvement. This suggests that patients without NP-59 uptake should be treated medically rather than surgically.
This study had some limitations. Because it was retrospective, AVS was not available for every patient. Hence, we could not directly compare the lateralization ability of AVS and NP-59. In addition, patients with negative lateralization results and a good response to medical treatments were not sampled for this study. As a result, the actual diagnostic specificity of NP-59 scintigraphy for IAH was not established.
CONCLUSION
Our study suggested that NP-59 SPECT/CT, with its high resolution and lesion localization ability, significantly improves the diagnostic accuracy of adrenal cortical scintigraphy in detecting adrenal adenoma and significantly improves prognostic accuracy in predicting postsurgical clinical outcome. Our results also suggest that patients with negative NP-59 imaging results may be precluded from surgical intervention. In our opinion, the advantage shown by this study for noninvasive NP-59 imaging using SPECT/CT also suggests that NP-59 may be used as the first lateralization modality after initial CECT for a clinically confirmed PA patient. We believe that this opinion will be reinforced by future studies with larger samples.
Acknowledgments
We acknowledge the support of the TAIPAI study group: Drs. Vin-Cent Wu, Yen-Hung Lin, Yi-Luwn Ho, Hung-Wei Chang, Lian-Yu Lin, Fu-Chang Hu, Kao-Lang Liu, Shuo-Meng Wang, Kuo-How Huang, Yung-Ming Chen, Chin-Chi Kuo, Shih-Chieh Chueh, Ching-Chu Lu, Fang-Chi Chang, Shih-Cheng Liao, Ruoh-Fang Yen, Wei-Chou Lin, Bor-Sen Hsieh, and Kwan-Dun Wu.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication April 3, 2009.
- Accepted for publication June 29, 2009.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Primary Aldosteronism and Long-term Outcomes Using PAMO Definition
- Clinical Value of 68Ga-Pentixafor PET/CT in Subtype Diagnosis of Primary Aldosteronism Patients with Adrenal Micronodules
- Development of Fluorinated NP-59: A Revival of Cholesterol Use Imaging with PET
- Functional Characterization of Adrenocortical Masses in Nononcologic Patients Using 68Ga-Pentixafor
- U-shaped relationship between left ventricular mass index and estimated glomerular filtration rate in patients with primary aldosteronism
- The relation among aldosterone, galectin-3, and myocardial fibrosis: a prospective clinical pilot follow-up study
- Aldosterone Induces Tissue Inhibitor of Metalloproteinases-1 Expression and Further Contributes to Collagen Accumulation: From Clinical to Bench Studies
- The Relation Between the Degree of Left Ventricular Mass Regression and Serum Potassium Level Change in Patients With Primary Aldosteronism After Adrenalectomy