


Visual Abstract

Abstract
Our objective was to investigate the clinical value of 68Ga-pentixafor PET/CT in subtype diagnosis of primary aldosteronism (PA) patients with adrenal micronodules less than 1 cm in diameter and compare it with the routine clinical methods. Methods: We used prospective enrollment of PA patients with adrenal micronodules identified by adrenal CT scans to undergo 68Ga-pentixafor PET/CT. Patients were divided into surgically eligible and ineligible groups based on surgical pathology and postoperative follow-up or adrenal venous sampling (AVS) results. Patient management was discussed by a multidisciplinary team. The semiquantitative parameters of PET/CT included SUVmax for adrenal lesion and SUV ratios for lesion to liver and lesion to normal adrenal gland. Results: In total, 123 PA patients with adrenal micronodules were examined using 68Ga-pentixafor PET/CT, and 104 patients who underwent surgery or successful AVS were included in the analysis (48 ± 10 y old). The sensitivity, specificity, and accuracy of visual analysis using 68Ga-pentixafor PET/CT to identify surgically eligible patients were 90.2%, 72.7%, and 86.5%, respectively, which were significantly higher than those of adrenal CT (73.1%, 53.8%, and 68.3%, respectively) and yielded consistent results in different CT morphologic or age subgroups. In 36 patients who had both AVS and 68Ga-pentixafor PET/CT, the tests showed a 66.7% concordance rate. However, PET/CT was significantly more concordant with surgical outcomes than was AVS in 17 patients who underwent adrenalectomy (82.4% vs. 68.86%). Among the 183 adrenal micronodules included in the study, the semiquantitative diagnostic thresholds for 92 lesions eligible for surgical treatment were an SUVmax of at least 4.55, an SUV ratio of at least 2.17 for lesion to liver, and an SUV ratio of at least 1.90 for lesion to normal adrenal gland. All patients benefited from surgical removal of 68Ga-pentixafor–avid microlesions. Conclusion: In PA patients with adrenal micronodules, 68Ga-pentixafor PET/CT demonstrated promising diagnostic accuracy in classification and appeared to perform better than adrenal CT. Furthermore, there was also a suggestion of some potential in predicting postoperative efficacy compared with AVS, although these observations require further investigation and verification in larger cohorts.
Primary aldosteronism (PA) is the most prevalent curable form of endocrine hypertension, characterized by low renin and high aldosterone levels (1). PA patients are at an increased risk of cardiovascular and cerebrovascular complications (2), highlighting the importance of early diagnosis and effective treatment for better outcomes.
The most important clinical classification of PA is differentiating between surgically eligible forms (e.g., unilateral/bilateral aldosterone-producing adenoma [APA] and unilateral adrenocortical hyperplasia [UAH]) and ineligible forms (e.g., bilateral adrenocortical hyperplasia [BAH]) (3). Adrenal CT and adrenal venous sampling (AVS) are recommended for PA subtyping by the Endocrine Society practice guidelines (4). However, adrenal CT can provide only morphologic, not functional, information. Around 40% of PA patients had nonconcordant adrenal CT and AVS results (5). Notably, the evaluation of adrenal microadenomas (≤10 mm) in PA patients is the primary limitation of adrenal imaging (3). Besides, AVS is invasive and technically challenging, with only a 50%–80% success rate for right adrenal vein cannulation, and carries the risk of significant complications (6).
Previous studies have explored noninvasive alternatives for PA subtyping, particularly in the field of nuclear functional imaging. However, existing methods such as 131I-NP-59 and 11C-metomidate have significant shortcomings, including time-consuming acquisition protocols, low specificity, and the need for pretreatment dexamethasone (7). Besides, the short half-life of 11C also limits its clinical use. Identifying and classifying adrenal microlesions remain a major limitation of adrenal imaging in PA patients.
C-X-C motif chemokine receptor 4 (CXCR4) is expressed on the surface of cell membranes, and previous studies have shown that it is highly expressed in most APAs (8). 68Ga-pentixafor, a CXCR4-specific ligand, has shown strong diagnostic efficacy in detecting APAs larger than 1 cm in diameter (9,10). However, the performance of 68Ga-pentixafor in characterizing adrenal micronodules remains unclear, and the uptake threshold for identifying the surgically eligible group in PA patients needs to be determined.
Therefore, the present study aimed to evaluate the performance of 68Ga-pentixafor PET/CT in characterizing adrenal micronodules and to compare it with adrenal CT and AVS. The study also aimed to determine the uptake threshold for identifying the surgically eligible group in PA patients. This research will provide valuable insights into the use of 68Ga-pentixafor PET/CT for noninvasive diagnosis of PA and could potentially improve clinical decision-making and patient outcomes.
MATERIALS AND METHODS
Patients
We conducted a prospective study between December 2018 and June 2022 using the following criteria for inclusion: a confirmed diagnosis of PA determined by an endocrinologist with 30 y of experience (the detailed diagnostic criteria are described in our previously published article (10)) and an adrenal CT scan showing unilateral or bilateral adrenal micronodules (≤1.0 cm in length) or small nodular hyperplasia (≤1.0 cm in thickness). Exclusion criteria included pregnancy, breastfeeding, or hypertension resulting from other causes. All included patients underwent 68Ga-pentixafor PET/CT (within 30 d after adrenal CT). The decision whether to perform AVS and the method of patient management were made by a multidisciplinary team comprising members from the departments of endocrinology, urology, and nuclear medicine at our hospital. The study protocol is further outlined in the supplemental materials (available at http://jnm.snmjournals.org). Written informed consent to undergo 68Ga-pentixafor PET/CT imaging was obtained from all patients, and the consent form and study protocol were approved by the Ethical Committee of Peking Union Medical College Hospital (institutional review board protocol ZS-1435). We registered the study at ClinicalTrials.gov (NCT04859959). Only patients who underwent adrenalectomy and had a follow-up time of 6–12 mo or who underwent successful AVS were included in the final analysis.
The following data were collected and calculated at baseline: general clinical information, antihypertensive drug dose (defined daily dose based on World Health Organization collaborating center, https://www.whocc.no/atc_%20ddd_index/%202010), aldosterone-to-renin ratio (plasma renin activity < 0.1 ng/mL/h was considered 0.1 ng/mL/h), and adrenal CT results. Six to 12 mo after adrenalectomy, the change in values was recorded.
Adrenal CT
Two experienced radiologists classified the adrenal CT imaging features of PA patients into the following 5 categories based on the morphologic changes in adrenal glands: unilateral single micronodule, unilateral micronodular hyperplasia, bilateral single micronodule, bilateral micronodular hyperplasia, and unilateral single micronodule with contralateral micronodular hyperplasia. Examples of CT performance are shown in Supplemental Figure 1. The diagnostic rules of CT are listed in the supplemental materials. The adrenal CT scans were plain CT scans.
68Ga-Pentixafor PET/CT
The preparation of 68Ga-pentixafor was previously published (10). The examination and reconstruction methods for 68Ga-pentixafor PET/CT can be found in the supplemental materials.
Two experienced nuclear medicine physicians who were unaware of the clinical information evaluated the 68Ga-pentixafor PET/CT data using MIM Encore (MIM Software). The first step involved categorizing the lesions as positive or negative for uptake through visual assessment. Then, the SUVmax of the adrenal microlesions, the ratio of lesion SUVmax to normal-liver SUVmean (LLR), the ratio of lesion SUVmax to normal-adrenal-tissue SUVmean (LAR), and the ratio of bilateral adrenal SUVmax (SUVmax lateralization index) were calculated. The criteria for visual and semiquantitative analysis are detailed in the supplemental materials.
Postoperative Outcome Assessment
Choice of surgical method can be found in the supplemental materials. The interval between adrenalectomy and 68Ga-pentixafor PET/CT ranged from 15 to 45 d. The median duration of follow-up was 8 mo (range, 6–12 mo). Postoperative clinical and biochemical outcomes were assessed according to the international multicenter PA surgical outcome criteria (11), which include complete success (cured), partial success (improvement), and absence of success (persistence).
AVS Examination for Subtype Diagnosis
AVS was performed without adrenocorticotropic hormone stimulation in our hospital. The supplemental materials describe the examination and calculation methods.
Diagnostic Criteria
Adrenal micronodules were classified as surgically eligible (including unilateral micro-APA, bilateral micro-APA, and micro-UAH) or surgically ineligible (including nonfunctioning micronodule and micro-BAH) on the basis of surgical pathology and postoperative follow-up or AVS results. When a patient underwent both surgical treatment and AVS examination, especially when there was a discrepancy between the 2 results, the follow-up results were considered the gold standard for diagnosis. According to whether there were adrenal micronodules requiring surgical resection, the patients were divided into surgically eligible and surgically ineligible groups.
Statistical Analysis
All data were processed by SPSS Statistics 22.0 (IBM) and GraphPad Prism 9 statistical software. Quantitative values are expressed as mean ± SD. Categoric variables are presented as numbers and percentages. Differences between 2 different groups were compared using the independent t test or the Mann–Whitney U test. The P value among 3 different groups was calculated via 1-way ANOVA and χ2 tests. Receiver-operating characteristic curves were constructed to determine the threshold of semiquantitative parameters of 68Ga-pentixafor PET/CT for the diagnosis of surgically eligible microlesions. The 95% CIs for diagnostic performance measures were calculated using the Wilson score. A P value of less than 0.05 was considered statistically significant.
RESULTS
Clinical Characteristics of Included Patients
A total of 123 PA patients with adrenal micronodules underwent 68Ga-pentixafor PET/CT. Nineteen patients were excluded for lacking a diagnostic basis (Fig. 1). Ultimately, 104 PA patients were included in the final analysis, of whom 82 were deemed surgically eligible and 22 surgically ineligible. Their clinical characteristics are in Table 1.

Flowchart of PA patients included in study. Because of impact of coronavirus disease 2019 pandemic, surgical treatment of 5 patients with lateralization in AVS had been postponed.
Clinical Characteristics of Included 104 PA Patients with Adrenal Micronodules
Inconsistent results between AVS and 68Ga-pentixafor PET/CT led to treatment decisions grounded in providing the greatest likelihood of surgical cure for the patient (details can be found in the supplemental materials). Eighty-five patients finally underwent laparoscopic adrenalectomy, including 76 in the surgically eligible group (56 with unilateral micro-APA, 6 with bilateral micro-APA, and 14 with micro-UAH) and 9 in the surgically ineligible group (9 with micro-BAH). The preoperative and postoperative characteristics of these patients are in Supplemental Table 1.
Efficacy of 68Ga-Pentixafor PET/CT Visual Analysis in Diagnosing Surgically Eligible PA Patients
The sensitivity, specificity, and accuracy of 68Ga-pentixafor PET/CT in diagnosing surgically eligible patients (subtype diagnosis) were 90.2%, 86.3%, and 89.4%, respectively, for all 104 enrolled PA patients. The performance of PET/CT is shown in Figure 2. As for the 85 surgical patients, the diagnostic efficacy of PET/CT in subtyping was significantly higher than that of adrenal CT (Table 2, P < 0.05). Among the 17 surgical patients who underwent both AVS and PET/CT, the accuracy of AVS examination was lower than that of PET/CT, using postoperative efficacy as the standard (Table 2).

Performance of 68Ga-pentixafor PET/CT in PA patients with different adrenal micronodules. MIP = maximum-intensity projection; NFN = nonfunctioning nodule.
Efficacy of 68Ga-Pentixafor PET/CT Visual Analysis in Diagnosing Surgically Eligible PA Patients and Comparison with Adrenal CT and AVS in Patients with Pathology and Postoperative Follow-up
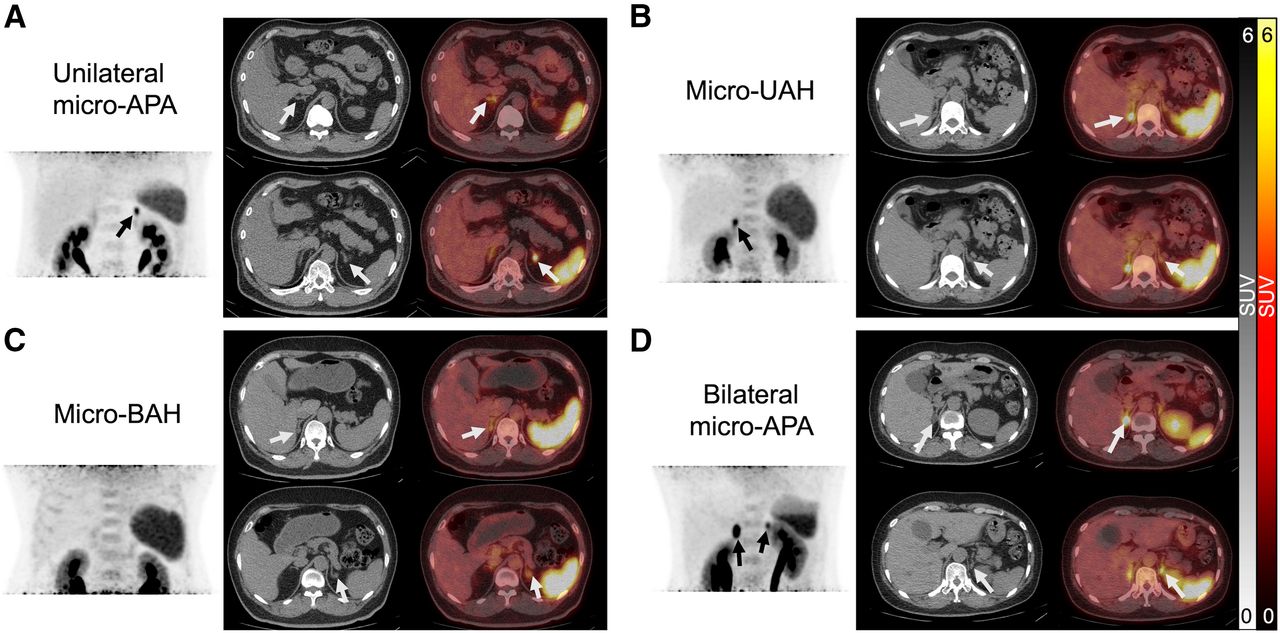
Furthermore, 68Ga-pentixafor PET/CT demonstrated better diagnostic performance than adrenal CT in both younger and older patients. In younger patients with unilateral single micronodules on adrenal CT, PET/CT also exhibited significantly higher diagnostic accuracy than adrenal CT (Supplemental Table 2). Additionally, adrenal CT displayed inferior diagnostic performance across various adrenal lesion morphologic groups, as shown in Supplemental Table 3. Examples of 68Ga-pentixafor PET/CT in PA patients with bilateral adrenal micronodules are shown in Figure 3.

Performance of 68Ga-pentixafor PET/CT in PA patients with bilateral microlesions on adrenal CT: unilateral micro-APA (A), micro-APA (B), micro-BAH (C), and bilateral micro-APA (D).
Patients with Adrenal Micronodules Who Underwent Both AVS and 68Ga-Penxitafor PET/CT
A total of 36 patients successfully underwent both AVS and 68Ga-pentixafor PET/CT, as shown in Table 3. The consistency rate was 66.7%, which was significantly higher (P < 0.05) than the concordance rate between AVS and adrenal CT (47.2%, Supplemental Table 4).
Consistency Evaluation in Patients Undergoing Concurrent AVS and 68Ga-Pentixafor PET/CT (n = 36)
Subsequently, in these 36 patients, the 68Ga-pentixafor SUVmax lateralization index values were 1.8 ± 0.7 for patients with unilateral AVS lateralization and 1.4 ± 0.5 for patients without AVS lateralization (P = 0.06). When the SUVmax lateralization index ratio was given a threshold of at least 1.35, using AVS as the gold standard, the sensitivity and specificity of PET/CT for lateralization were 70.6% and 68.4%, respectively (area under the curve, 0.74; P < 0.05).
Lesional Characteristics and Imaging Manifestations
There were 76 micro-APA lesions, 16 micro-UAH lesions, 51 micro-BAH lesions, and 40 nonfunctioning micronodule lesions among the 104 patients in this study. Micro-APA lesions had the highest 68Ga-pentixafor SUVmax, LLR, and LAR, followed by micro-UAH, whereas micro-BAH and nonfunctioning micronodule had relatively lower uptake values (Table 4). In this study, pathologic results were obtained for 86 adrenal lesions; the uptake of 68Ga-pentixafor in adenomas was significantly higher than that in nodular hyperplastic lesions, and the difference was statistically significant (Supplemental Table 5).
Imaging Variables of 183 Adrenal Micronodules in All PA Patients
Efficacy of 68Ga-Pentixafor PET/CT for Differential Diagnosis of Micronodules
Ninety-two surgically eligible micronodules and 91 ineligible micronodules were identified. Visual analysis of 68Ga-pentixafor PET/CT showed 97 positive and 86 negative micronodules. The thresholds for SUVmax, LLR, and LAR were 4.55, 2.17, and 1.90, respectively. The visual analysis had higher sensitivity, whereas the semiquantitative analysis had higher specificity (Table 5). Supplemental Figure 2 displays examples of surgically eligible microlesions that were positive on visual analysis but negative on semiquantitative analysis for 68Ga-pentixafor PET/CT.
Diagnostic Performance of 68Ga-Pentixafor PET/CT to Distinguish Surgically Eligible and Ineligible Micronodules
Relationship Between Surgical Outcome and 68Ga-Pentixafor PET/CT Performance
Seventy-six surgical patients had biochemical results checked during postoperative follow-up. Among them, 63.5% achieved biochemical cure, 23.7% showed biochemical improvement, and 4.7% had absence of success (persistence). All achieved biochemical cure or improvement after the 68Ga-pentixafor–positive micronodules were resected, with a cure rate of up to 80% (Supplemental Fig. 3). The adrenal micronodules had a higher 68Ga-pentixafor SUVmax, LLR, and LAR in the patients with biochemical cure or improvement than in the persistence group (Fig. 4). Baseline clinical characteristics did not significantly differ among the 3 outcome groups (Supplemental Table 6).

(A) Highest proportion of patients with 68Ga-pentixafor PET/CT–positive adrenal microlesions was observed in biochemical/clinical cure group, followed by biochemical/clinical improvement group, whereas all patients in biochemical/clinical persistence group had negative PET/CT imaging results. (B) Patients in biochemical cure/improvement group had significantly higher 68Ga-pentixafor uptake values than those in biochemical persistence group. (C) Values of SUVmax, LLR, and LAR of removed adrenal micronodules decreased gradually from group of patients with clinical cure to those with clinical improvement and finally to those with clinical persistence. ns = not statistically significant. *P < 0.05. **P < 0.01.
In terms of clinical outcomes in the 85 surgical patients, 34 (40.0%) achieved clinical cure, 47 (55.3%) showed clinical improvement, and 4 (4.7%) had persistent clinical symptoms. All PA patients with positive adrenal micronodules on 68Ga-pentixafor PET/CT achieved clinical cure or improvement after adrenalectomy, with a cure rate of 47.9%. The SUVmax, LLR, and LAR of the resected adrenal micronodules decreased progressively from the clinical cure group to the clinical improvement group to the clinical persistence group, with significant differences among the 3 groups (Fig. 4). Comparison of the baseline characteristics of patients with different clinical outcomes showed that female patients with a lower body mass index, shorter duration of hypertension, nonrefractory hypertension, and lower dose of antihypertensive drugs before surgery were more likely to achieve clinical cure (Supplemental Table 7).
Correlation Between 68Ga-Pentixafor PET/CT Uptake in Positive Lesions and Biochemical/Clinical Values in Surgical Patients
In further analyzing the correlation between PET/CT semiquantitative parameters and clinical indicators in 71 patients who underwent removal of PET-positive adrenal micronodules (Supplemental Table 8), we found that the greater the 68Ga-pentixafor positivity in the adrenal micronodules, the greater was the decrease in postoperative systolic and diastolic blood pressure and postoperative defined daily dose and the greater was the degree of biochemical improvement and increase in blood potassium levels achieved through surgery.
DISCUSSION
The occurrence of adrenal micronodules in PA patients is common, with previous studies reporting that micro-APA lesions comprise approximately 13%–30% of all cases of APA (12). Because of the tendency to miss or misdiagnose these lesions using routine imaging examinations, the functional evaluation of adrenal micronodules has always been challenging in subtype classification of PA (3). There has been considerable interest in exploring noninvasive alternatives, particularly in the field of nuclear functional imaging. This study used 68Ga-pentixafor PET/CT to subtype PA patients with adrenal micronodules and compare this modality with adrenal CT and AVS.
Adrenal CT is often recommended as the first step in the subtype classification of PA but can result in missed opportunities for adrenalectomy in some patients and unnecessary surgery in others (13). In the present study, 68Ga-pentixafor PET/CT improved subtype diagnostic efficacy in PA patients with adrenal micronodules compared with adrenal CT and yielded consistent results in different CT morphologic subgroups. In addition, our study suggested that visual assessment of 68Ga-pentixafor PET/CT images may be sufficient because of the highly specific uptake in functional adrenal micronodules. The fact that semiquantitative analysis of 68Ga-pentixafor PET data had no significant impact on diagnostic performance could be attributed to the variability in uptake across micro-APAs and the inherent limitations of such an analysis due to patient-specific, technical, and methodologic factors.
The incidence of nonfunctional adrenal adenoma decreases in individuals under 40 y old (14). Guidelines suggest that PA patients under 35 y old with unilateral adrenal nodules detected on adrenal CT may consider surgery without AVS (15). However, our study found that relying solely on adrenal CT results for subtyping diagnosis in such patients remains inaccurate and that surgery may be recommended directly only when 68Ga-pentixafor–positive adrenal nodules are present.
A clinical study (16) comparing the diagnostic performance of 68Ga-pentixafor PET/CT and AVS in the subtyping of 100 PA patients found a diagnostic consistency rate of 90%. However, adrenal micronodules were not analyzed further, and diagnoses were not confirmed on the basis of postsurgical follow-up. However, the consistency rate in our study was lower than in the aforementioned study, potentially because of inclusion of only patients with microlesions. Our study suggested that the results of 68Ga-pentixafor PET/CT may be more consistent with postoperative efficacy than is AVS. Nevertheless, further research is necessary to substantiate these preliminary findings.
There have been studies indicating that the level of CYP11B2 is higher in micro-APA than in macro-APA (12). Considering the positive correlation between the expression level of CXCR4 and CYP11B2, the expression density of CXCR4 should theoretically be higher in micro-APA than in macro-APA. Nevertheless, on comparing our team’s previous research (17), we found that the uptake of 68Ga-pentixafor PET/CT is higher in macro-APA than in micro-APA (SUVmax, 15.3 ± 7.7 (17) vs. 8.4 ± 4.2). We suspect that this difference may be attributed to the limited spatial resolution of 68Ga-pentixafor PET/CT. With smaller lesion volumes, partial-volume effects may be more prominent, leading to lower measured SUVs than the actual values. The smallest micro-APA lesion that could be identified in this study had a diameter of 0.6 cm. In future research, it could be beneficial to explore the potential of other technologies, such as 68Ga-pentixafor PET/MRI, or more specific radiotracers in assessing uptake in small adrenal lesions.
In our study, all patients whose 68Ga-pentixafor–positive microlesions were removed achieved complete or partial biochemical/clinical success postoperatively. Higher uptake of 68Ga-pentixafor in the removed microlesions was associated with better surgical outcomes. We also found that female patients with a lower body mass index, shorter duration of hypertension, nonrefractory hypertension, and less antihypertensive drug use before surgery had a higher probability of achieving clinical cure after surgery, as is consistent with previous literature (12).
There were some limitations in this study. Because our institution did not routinely perform CYP11B2 staining on PA lesions, the latest international consensus statement on the histopathologic diagnostics of adrenal tumors and hyperplasia published by the International Endocrine Society (18) was not applied. Our single-center study design inherently has certain biases. Additionally, although the adrenal micronodules in our study were detectable on adrenal CT, some microadenomas might have been missed. Moreover, few patients underwent both 68Ga-pentixafor PET/CT and AVS, causing potential bias. Importantly, the decision-making process in our study—to forego the established reference method, AVS, on the basis of the 68Ga-pentixafor PET/CT results in certain scenarios—highlights a potential limitation. Thus, we underline the need for larger, multicenter studies to further validate the efficacy and reliability of 68Ga-pentixafor PET/CT in comparison with AVS.
CONCLUSION
Our findings suggest that 68Ga-pentixafor PET/CT holds promise in outperforming adrenal CT for classifying different morphologic subtypes of PA patients with adrenal micronodules. Moreover, this technique seems to offer improved consistency in predicting postoperative efficacy in PA patients compared with AVS examination. However, larger controlled clinical trials are necessary to confirm this observation. The level of 68Ga-pentixafor uptake in adrenal micronodules appears to be a valuable guide for recommending appropriate surgical treatments for PA patients, thereby facilitating the implementation of personalized management strategies.
DISCLOSURE
This work was sponsored in part by the National Natural Science Foundation of China (grant 82071967), the National Key Research and Development Program of China (grant 2020YFC2002702), the Tsinghua University–Peking Union Medical College Hospital Initiative Scientific Research Program (grant 52300300519), and the National Natural Science Foundation of China (grant 81770427). No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: How well does 68Ga-pentixafor PET/CT perform in subtype diagnosis of PA patients with adrenal micronodules less than 1 cm in diameter, and how does 68Ga-pentixafor PET/CT compare with standard diagnostic methods such as adrenal CT and AVS?
PERTINENT FINDINGS: 68Ga-pentixafor PET/CT showed superior sensitivity, specificity, and accuracy in identifying surgically eligible PA patients compared with adrenal CT. It was also more concordant with surgical outcomes than AVS.
IMPLICATIONS FOR PATIENT CARE: This study showed that a new imaging technique, 68Ga-pentixafor PET/CT, can accurately classify adrenal micronodules in PA patients, helping doctors make better treatment decisions and predict treatment outcomes.
Footnotes
↵* Contributed equally to this work.
Published online Nov. 30, 2023.
- © 2024 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication May 24, 2023.
- Revision received October 17, 2023.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Is the Clinical Application of CXCR4 Imaging in the Diagnosis and Management of Primary Aldosteronism Really Happening?
- The Potential Value of Functional Adrenal Imaging in Primary Aldosterone
- Reply: The Potential Value of Functional Adrenal Imaging in Primary Aldosterone
- Comparison of Different Diagnostic Criteria of 68Ga-Pentixafor PET/CT for the Classification of Primary Aldosteronism