


Abstract
The coronary artery calcium (CAC) score is a readily and widely available tool for the noninvasive diagnosis of atherosclerotic coronary artery disease (CAD). The aim of this study was to investigate the added value of the CAC score as an adjunct to gated SPECT for the assessment of CAD in an intermediate-risk population. Methods: Seventy-seven prospectively recruited patients with intermediate risk (as determined by the Framingham Heart Study 10-y CAD risk score) and referred for coronary angiography because of suspected CAD underwent stress 99mTc-tetrofosmin SPECT myocardial perfusion imaging (MPI) and CT CAC scoring within 2 wk before coronary angiography. The sensitivity and specificity of SPECT alone and of the combination of the 2 methods (SPECT plus CAC score) in demonstrating significant CAD (≥50% stenosis on coronary angiography) were compared. Results: Forty-two (55%) of the 77 patients had CAD on coronary angiography, and 35 (45%) had abnormal SPECT results. The CAC score was significantly higher in subjects with perfusion abnormalities than in those who had normal SPECT results (889 ± 836 [mean ± SD] vs. 286 ± 335; P < 0.0001). Similarly, with rising CAC scores, a larger percentage of patients had CAD. Receiver-operating-characteristic analysis showed that a CAC score of greater than or equal to 709 was the optimal cutoff for detecting CAD missed by SPECT. SPECT alone had a sensitivity and a specificity for the detection of significant CAD of 76% and 91%, respectively. Combining SPECT with the CAC score (at a cutoff of 709) improved the sensitivity of SPECT (from 76% to 86%) for the detection of CAD, in association with a nonsignificant decrease in specificity (from 91% to 86%). Conclusion: The CAC score may offer incremental diagnostic information over SPECT data for identifying patients with significant CAD and negative MPI results.
Myocardial perfusion imaging (MPI) with gated SPECT is a well-established and widely accepted test for the diagnostic and prognostic evaluation of patients with known or suspected coronary artery disease (CAD) (1,2). Recently, there has been growing interest in the use of coronary artery calcium (CAC) imaging to diagnose early subclinical atherosclerosis and to improve risk stratification in asymptomatic individuals (3–5). Although not promoted as a means to identify the presence of coronary stenoses (6–8), higher CAC scores are associated with increased plaque burden and increased cardiovascular risk (4,9). Recent data provide support for the concept that the CAC score is most useful in terms of the incremental prognostic value for populations with intermediate risk (10,11). Previous studies demonstrated that a large discrepancy exists between the anatomic extent of CAD and ischemia and that a considerable number of stenoses do not result in abnormal perfusion on MPI (3,12–14). As a consequence, combining morphoanatomic information (CAC) with functional information obtained from SPECT may allow for improved risk stratification and provide additional information for the clinician. CAC imaging may be useful for identifying patients with extensive atherosclerosis but without stress-induced ischemia and who may be referred for risk factor modification and aggressive medical treatment. Furthermore, CAC imaging could help in guiding decision making for patients with equivocal MPI results.
The aims of this study were to investigate the added value of the CAC score as an adjunct to gated SPECT for the assessment of CAD in an intermediate-risk population and to define an optimal CAC score cutoff for this purpose.
MATERIALS AND METHODS
Patients and Study Protocol
The initial study group consisted of 119 prospectively recruited patients who were scheduled for elective coronary angiography because of suspected CAD and who consented to undergo gated SPECT and CAC imaging within 2 wk before invasive catheterization. Medical history, including cardiovascular risk factors, height, weight, blood pressure, lipid profile, a 12-lead electrocardiogram (ECG), and the 10-y absolute CAD risk predicted on the basis of the Framingham Heart Study risk function, was obtained for all patients. Diabetes mellitus was defined as a fasting glucose level of ≥140 mg/dL or the need for insulin or oral hypoglycemic agents. Hypercholesterolemia was defined as a total cholesterol level of ≥200 mg/dL or treatment with lipid-lowering medications. Hypertension was defined as a blood pressure of ≥140/90 mm Hg or the use of antihypertensive medications. Of the 119 patients, 77 patients (45 men and 32 women; age [mean ± SD], 66 ± 9 y; range, 42–82 y) fulfilled the following inclusion criteria: no previously known CAD; typical or atypical chest pain, dyspnea, or signs of myocardial ischemia on a resting ECG or bicycle stress test; and intermediate risk (10%–20%), as determined on the basis of the Framingham Heart Study 10-y CAD risk score. The mean time delays between coronary angiography and CT examination and between coronary angiography and gated SPECT were 7 ± 14 and 4 ± 14 d, respectively. All patients were in a clinically stable condition at the time of the study. The MPI and CAC score results were not communicated to the interventional cardiologists. The study protocol was approved by the local ethics committee, and written informed consent was obtained from all patients. The characteristics of the study population are summarized in Table 1.
Clinical Characteristics of Study Population With and Without Significant CAD (n = 77)*
Gated SPECT
All patients underwent a 1-d stress (intravenous adenosine at 0.14 mg/kg/min)–rest MPI protocol with doses of 350 and 900 MBq of 99mTc-tetrofosmin, respectively. Patients were instructed to refrain from caffeine-containing beverages for at least 12 h, nitrates for 24 h, and β-blockers for 48 h before the study. Data acquisition was performed by use of a hybrid SPECT/CT dual-head camera with the Hawkeye facility (Infinia; GE Healthcare) and the following parameters: a low-energy, high-resolution collimator; a 20% symmetric window at 140 keV; a 64 × 64 matrix; an elliptic orbit; and step-and-shoot acquisition at 3° intervals over 180°. SPECT images were reconstructed with an iterative ordered-subsets expectation maximization algorithm (2 iterations, 10 subsets) into short-axis, vertical long-axis, and horizontal long-axis slices encompassing the entire left ventricle. A low-dose CT scan for attenuation correction was performed as previously reported (15). ECG gating was performed at rest.
A semiquantitative visual interpretation of the attenuation-corrected stress and rest images was performed by consensus of 2 experienced nuclear cardiologists who were unaware of the results of the CT examination and coronary angiography findings. With a 20-segment model, each segment was assigned to one of the major vascular territories (16). The short-axis data were displayed in polar map format and normalized to peak myocardial activity (100%) with a commercially available quantitative gated and perfusion SPECT software package (Cedars QGS/QPS; Cedars-Sinai Medical Center) (17). Segments were scored for radiotracer uptake with a 5-point score (0 = normal, 1 = equivocal, 2 = moderately reduced, 3 = severely reduced, and 4 = absent). Fixed perfusion defects (scar) and reversible defects (ischemia) were considered abnormal findings, as previously reported (18). The extent of reversible defects was categorized as mild (≤5%), moderate (>5 and ≤10%), or large (>10%) (19). We did not consider mild or moderate fixed perfusion defects to be abnormal if there was normal segmental contraction or thickening (20).
CAC Imaging
For CAC imaging, a nonenhanced, retrospectively ECG-gated scan was obtained by use of a 64-slice CT scanner (Siemens Somatom Sensation 64) with a collimation of 32 × 0.6 mm, a tube voltage of 120 kV, and an effective tube–current time product of 60 mAs. The estimated effective radiation dose (with ECG-controlled dose modulation) for this protocol is in the range of 1–3 mSv. Patients with a heart rate of greater than 65 beats per minute received metoprolol at 5–20 mg intravenously before the CT scan. Image reconstruction was performed at 55% of the R-R interval, with a nonoverlapping effective slice thickness of 3 mm and a dedicated convolution kernel (B35f). The total calcium burden in the coronary arteries was manually measured by planimetry by a single masked investigator according to the scoring algorithm of Agatston et al. (21). On the basis of the total Agatston score, patients were placed into 5 categories, as previously reported (22): less than or equal to 10 (minimal or insignificant CAC), 11–100 (mild CAC), 101–400 (moderate CAC), 401–1,000 (severe CAC), and greater than 1,000 (extensive CAC).
Quantitative Coronary Angiography
Invasive coronary angiograms were evaluated by consensus of 2 interventional cardiologists who were unaware of the SPECT and CAC imaging results. Coronary arteries were subdivided into 15 segments, as proposed by the guidelines of the American Heart Association (23). Segments were classified as normal, as having nonobstructive disease (luminal irregularities or <50% stenosis), or as having significant stenosis. Stenosis was evaluated in 2 different views and classified as significant if the mean lumen diameter reduction was 50% or greater, as depicted with commercial quantitative coronary angiography software and hardware (Xcelera; Philips) as previously reported (24).
Data Interpretation
Significant CAD was defined as the presence of at least 1 coronary vessel stenosis of 50% or greater in a major epicardial coronary vessel by the gold standard of quantitative coronary angiography. SPECT images were categorized visually by consensus of 2 experienced readers with a 5-point scale (1 = definitely normal, 2 = probably normal, 3 = equivocal, 4 = possibly abnormal, and 5 = definitely abnormal). Results described as equivocal were always considered incorrect. To investigate whether a high CAC score could be used to detect significant CAD missed by MPI, a receiver-operating-characteristic (ROC) analysis was performed for the subgroup of patients with normal SPECT findings (scores of 1 and 2). The optimal CAC score threshold was determined as the cutoff that on ROC analysis resulted in the best sensitivity for the detection of significant CAD with an associated specificity of greater than 90%. Subsequently, this CAC score threshold was used to evaluate the diagnostic performance of SPECT alone and of SPECT combined with the CAC score for the prediction of significant CAD in the entire study population with the following rules: Abnormal SPECT results (scores of 3–5) were always classified as abnormal findings, regardless of the CAC score. If the SPECT score was 1 or 2 and the CAC score was above the cutoff defined by ROC analysis, then the results also were classified as abnormal findings; that is, CAC score results overruled SPECT results.
Statistical Analysis
Statistical analysis was performed with a commercially available software package (SPSS version 12.0 for Windows; SSPS Inc.). Data were expressed as mean ± SD for continuous variables and as frequencies and percentages for categoric variables. Comparisons were performed with t tests, Mann–Whitney U tests, or χ2 tests, as appropriate. Linear regression analysis was used to determine whether there was a correlation between the CAC score and perfusion abnormalities on SPECT. Regression results were also presented as odds ratios (ORs) and their respective 95% confidence intervals (CIs). Differences in sensitivity and specificity were compared with the McNemar test. Multivariate stepwise logistic regression analysis was performed with factors that had a significant relationship in univariate analysis to detect independent predictors of angiographic CAD. A P value of less than 0.05 (2-sided) was considered statistically significant for all tests.
RESULTS
Quantitative Coronary Angiography
Forty-two (55%) of the 77 patients had significant CAD. The distributions of single-vessel, 2-vessel, and 3-vessel disease were 17 patients (41%), 14 patients (33%), and 11 patients (26%), respectively. Left main stem stenosis was found in 1 patient. Moderate stenosis (stenosis grade of 50%–75%) was detected in 4 patients, and severe stenosis (stenosis grade of >75%) was found in 38 patients. Nine (26%) of the 35 patients without significant CAD had a normal angiogram, and 26 (74%) of the 35 patients had nonobstructive disease (luminal irregularities or <50% stenosis).
Gated SPECT
Visual analysis revealed 25 reversible, 9 fixed, and 10 mixed (reversible and fixed) perfusion defects in 35 (45%) of 77 patients. Of the 25 reversible defects, 11 were allocated to the left anterior descending artery (LAD), 4 were allocated to the left circumflex artery (LCX), and 10 were allocated to the right coronary artery territory (RCA). The distributions of mild, moderate, and large reversible defects were 13 patients (52%), 8 patients (32%), and 4 patients (16%), respectively. Two of the 9 fixed defects were allocated to the LAD, 2 were allocated to the LCX, and 5 were allocated to the RCA. SPECT images were categorized as abnormal in 35 patients.
CAC Imaging
Overall, the CAC score was deemed assessable in 304 (99%) of 308 coronary arteries in 77 patients. Four coronary vessels were affected by motion artifacts and were excluded from further analysis. The heart rate (mean ± SD) during the scan was 63 ± 9 beats per minute. The 77 subjects had a CAC score (mean ± SD) of 560 ± 682 (range, 0−3,968). Twelve (16%) of the 77 patients had minimal or insignificant CAC (≤10), 10 patients (13%) had mild CAC (11–100), 20 patients (26%) had moderate CAC (101–400), 20 patients (26%) had severe CAC (401–1,000), and 15 patients (19%) had extensive CAC (>1,000). Calcium was present in the left main artery in 10 patients (13%) and in the LAD, LCX, and RCA in 66 patients (86%), 49 patients (64%), and 52 patients (68%), respectively. The average calcium score in the LAD (250 ± 272) was significantly higher than those in the LCX (120 ± 443) and in the RCA (176 ± 289) (both Ps < 0.05).
Relationship Between CAC Imaging and Gated SPECT
The relationship between the prevalence and severity of myocardial perfusion abnormalities and the extent of CAC is shown in Figure 1. None of the 12 patients with a CAC score of less than or equal to 10 had perfusion defects. In contrast, 4 of the 10 patients with mild CAC, 8 of the 20 patients with moderate CAC, 10 of the 20 patients with severe CAC, and 13 of the 15 patients with extensive CAC had abnormal perfusion. The mean CAC score was significantly higher in subjects with perfusion abnormalities than in those who had normal SPECT results (889 ± 836 vs. 286 ± 335; P < 0.0001). The fraction of patients with significant CAD gradually increased with rising CAC scores (Fig. 2). Of the 42 patients with normal SPECT results, 31 (74%) showed atherosclerosis on CAC imaging (CAC score of >0), with 21 patients showing nonobstructive CAD (<50% stenosis) and 10 patients showing obstructive CAD (≥50% stenosis) on quantitative coronary angiography. The mean CAC score was higher in patients with CAD than in patients without CAD (856 ± 771 vs. 205 ± 289; P < 0.0001). A modest but statistically significant correlation between the total CAC score and myocardial perfusion abnormalities on SPECT was found (r = 0.444; P < 0.0001).
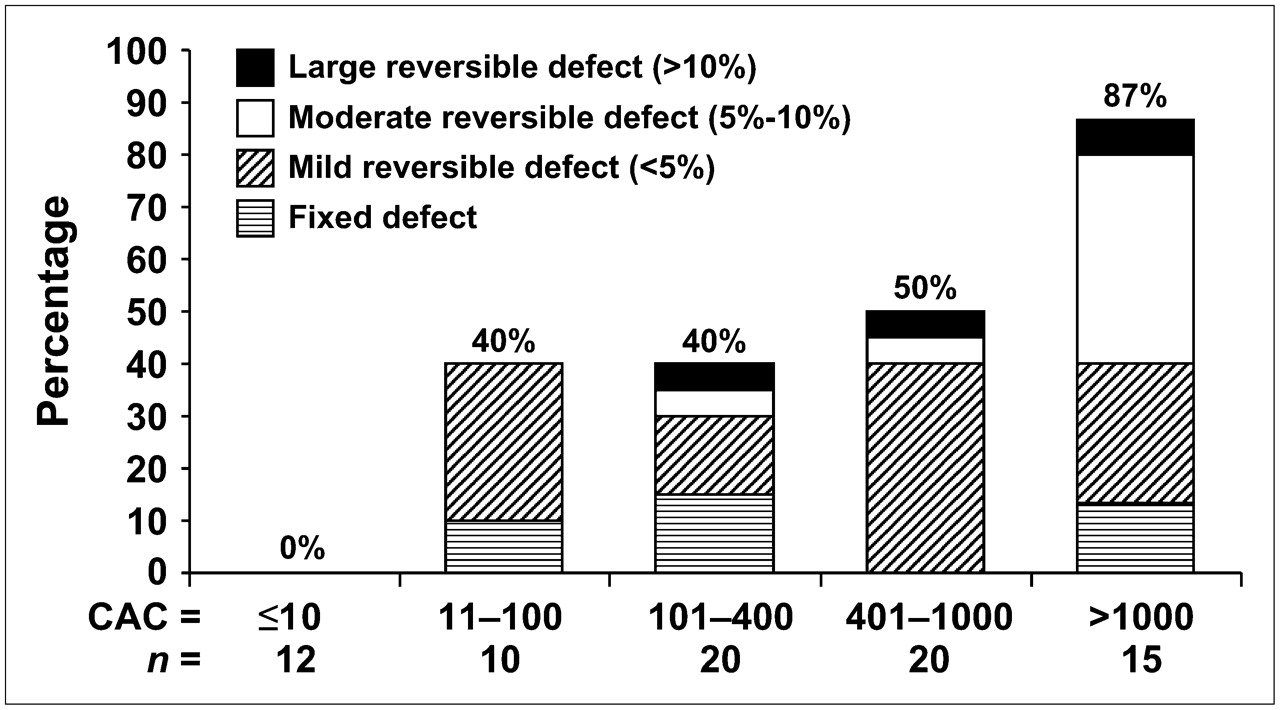
Relationship between prevalence and severity of myocardial perfusion abnormalities and extent of coronary artery calcification. n = number of patients in each CAC category who underwent gated SPECT.
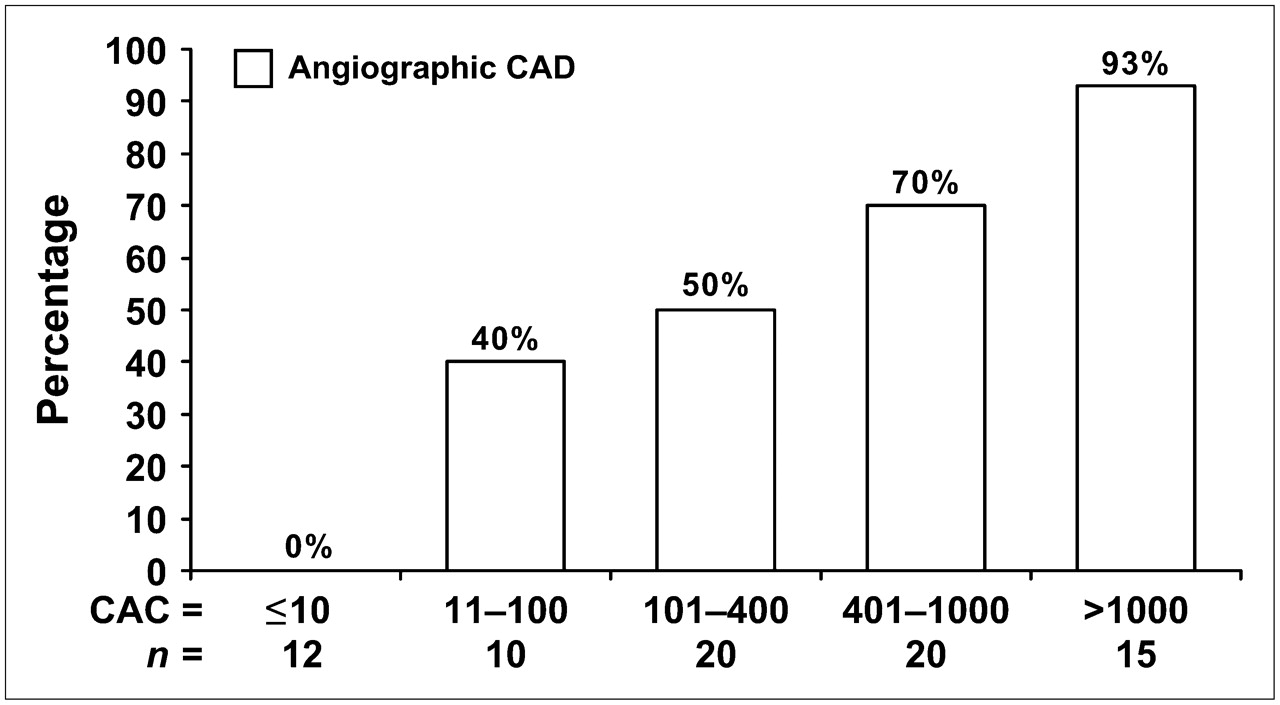
Relationship between extent of coronary artery calcification and prevalence of significant CAD detected by quantitative coronary angiography (angiographic CAD). n = number of patients in each CAC category who underwent invasive catheterization.
Gated SPECT Alone Versus Quantitative Coronary Angiography
The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of SPECT alone for the detection of significant CAD in patients were 76%, 91%, 91%, and 76%, respectively. There were 10 patients with false-negative findings. Six of these 10 patients had single-vessel disease, 2 patients had 2-vessel disease, and 2 patients had 3-vessel disease. There were 3 patients with nonobstructive disease and false-positive findings related to artifacts (1 apical and 2 anterior artifacts).
Gated SPECT Plus CAC Score Versus Quantitative Coronary Angiography
The optimal CAC score threshold was determined as the cutoff that on ROC analysis resulted in the best sensitivity for the detection of significant CAD with an associated specificity of greater than 90%. Figure 3 shows that a CAC score of greater than or equal to 709 was the optimal cutoff for detecting patients with CAD missed by SPECT. When this threshold was used, SPECT and the CAC score combined had a sensitivity of 86% and a specificity of 86% for the detection of patients with CAD. The addition of the CAC score thus improved the sensitivity of SPECT from 76% to 86% without a significant decrease in specificity (from 91% to 86%). Accordingly, the NPV increased from 76% to 83% and the PPV decreased from 91% to 88% when the combined approach was used (Table 2). The combination of data from the CAC score and SPECT corresponded to the correct reclassification of 4 of 10 patients with false-negative SPECT results.

ROC curve for detection of significant CAD (≥50% stenosis) in patients with normal MPI results (n = 42) by use of CAC score. CAC score of greater than or equal to 709 was optimal cutoff for detecting patients with CAD missed by SPECT (arrow). AUC = area under curve.
Diagnostic Performance of Gated SPECT Alone and of SPECT Plus CAC Score for Detection of Significant CAD (n = 77)
Predictors of Significant CAD
Univariate analysis revealed that the following factors were associated with significant CAD: age, Framingham Heart Study risk score, CAC score, and SPECT abnormalities. From these factors, multivariate stepwise logistic regression analysis selected SPECT abnormalities (OR, 17.5; 95% CI, 2.3–133.2; P = 0.001) and CAC (OR, 6.5; 95% CI, 0.8–54.6; P = 0.012) as independent predictors of the presence of CAD.
DISCUSSION
The present study indicates that the CAC score may have the potential to improve the diagnostic performance of MPI in detecting significant CAD in an intermediate-risk population. Combining morphoanatomic information (CAC) with functional information obtained from SPECT provides complementary information, because the 2 modalities reflect different pathophysiologic aspects of CAD. We found that a CAC score of greater than or equal to 709 was the optimal cutoff for detecting patients with CAD despite normal MPI results. With this threshold, the combination of the CAC score and SPECT improved sensitivity and NPV in detecting patients with coronary stenosis over those of SPECT alone without a significant decrease in specificity. This technique may improve the identification of patients requiring further investigation with conventional coronary angiography. On the other hand, all patients with a CAC score of less than or equal to 10 had normal angiography findings. Because these patients also had normal perfusion on SPECT, the CAC score did not provide additional information for them.
The vast majority of patients for whom true-negative findings were obtained by the combination of SPECT and the CAC score nevertheless had substantial calcifications, although the CAC score was below the cutoff. This finding highlights the fact that the presence of atherosclerosis does not necessarily result in perfusion abnormalities on MPI. Conversely, normal perfusion on SPECT does not exclude subclinical or obstructive CAD. With increasing severity of the CAC score, more patients had abnormal SPECT results as well as more severely abnormal SPECT results. These findings are in line with those of previous studies that compared the relationship between stress-induced perfusion abnormalities on SPECT and the extent of CAC (3,12,13). Anand et al. (25) observed a high prevalence of silent ischemia on MPI in 18% of individuals with a CAC score of 100–400, and 45% of patients with a CAC score of greater than or equal to 400 had abnormal SPECT results. Similar results were obtained by Berman et al. (3). They emphasized that patients with normal SPECT results frequently have extensive atherosclerosis on the basis of CAC criteria. This nonobstructive form of atherosclerosis is generally perceived as subclinical CAD. Recent data, however, suggest that this condition instead should be recognized as a preclinical state with strong predictive value for the development of CAD (26). According to the recommendations of the National Cholesterol Education Program (Adult Treatment Panel III), preclinical CAD should prompt aggressive risk factor modification (27). This information cannot be gained from SPECT alone, indicating a further added value of SPECT and the CAC score combined (27).
The use of CAC imaging is likely to increase in the near future because of the widespread availability of multislice CT scanners. This scenario is particularly true with the integration of the latter into hybrid SPECT/CT scanners, so that multislice CT data from the CAC score may be used for attenuation correction of myocardial perfusion SPECT images (28). Thus, the CAC score may offer incremental diagnostic information over SPECT data alone, with no additional radiation, if a low-dose CT attenuation scan (1–2 mSv) is also used for CAC imaging. Nevertheless, the diagnostic impact, cost-effectiveness, and clinical outcome of such multimodal imaging algorithms need to be evaluated in future prospective trials to better understand the short- and long-term risk for cardiac events among patients with normal MPI and high CAC scores.
In the present study, the sensitivities of SPECT alone were somewhat lower and the specificities were slightly higher than values usually reported in the literature, in which MPI was shown to have an average sensitivity of 89% and an average specificity of 75% in vasodilator stress studies (1). However, ECG gating and the use of x-ray-based attenuation correction, as performed for our patients, have been reported to improve the specificity of cardiac SPECT without affecting sensitivity (1,29). The interpretation of fixed perfusion defects as normal if there was normal contraction may have further contributed to this result in our study. Finally, in contrast to most of the literature, in which patients generally did not undergo angiography when SPECT results were normal, the present study was not subject to such referral bias, because all patients underwent diagnostic angiography regardless of SPECT results. Thus, the results of the present study, including a relatively high specificity, are likely to reflect more closely the real-life situation.
The influence of selection bias represents a potential limitation of our study. Because we selected a population that was already scheduled for coronary angiography, this cohort was expected to have a higher likelihood of CAD than a population referred for noninvasive testing. Consequently, the reported accuracies in our study are affected by the pretest likelihood of CAD in the patients examined. However, this limitation is common in studies in which coronary anatomy is used as an endpoint for assessing the value of noninvasive imaging for diagnosing CAD. A further limitation was that the definition of the optimal CAC threshold for the detection of significant CAD was extracted from the same study population that was then analyzed with the combined approach and not from a separate group of patients. Finally, the sample size of the present study was relatively small; a larger patient population needs to be studied to confirm our findings.
CONCLUSION
The CAC score may offer incremental diagnostic information over SPECT data for identifying patients with significant CAD and negative MPI results.
Acknowledgments
Philipp A. Kaufmann was supported by a grant from the Swiss National Science Foundation (SNSF-professorship grant no. PP00A-68835). Hatem Alkadhi was supported by the National Center of Competence in Research, Computer Aided and Image Guided Medical Interventions (NCCR CO-ME) of the Swiss National Science Foundation.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication February 19, 2007.
- Accepted for publication June 8, 2007.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Deep Learning Coronary Artery Calcium Scores from SPECT/CT Attenuation Maps Improve Prediction of Major Adverse Cardiac Events
- Radiomics Analysis of Clinical Myocardial Perfusion Stress SPECT Images to Identify Coronary Artery Calcification
- CACS and the Frequency of Stress-Induced Myocardial Ischemia During MPI: A Meta-Analysis
- Combined Quantitative Assessment of Myocardial Perfusion and Coronary Artery Calcium Score by Hybrid 82Rb PET/CT Improves Detection of Coronary Artery Disease
- SNMMI/ASNC/SCCT Guideline for Cardiac SPECT/CT and PET/CT 1.0
- Prognostic Interplay of Coronary Artery Calcification and Underlying Vascular Dysfunction in Patients With Suspected Coronary Artery Disease
- Does Rubidium-82 PET Have Superior Accuracy to SPECT Perfusion Imaging for the Diagnosis of Obstructive Coronary Disease?: A Systematic Review and Meta-Analysis
- Myocardial perfusion scintigraphy: technical innovations and evolving clinical applications
- Very high coronary calcium score unmasks obstructive coronary artery disease in patients with normal SPECT MPI
- Validation of CT Attenuation Correction for High-Speed Myocardial Perfusion Imaging Using a Novel Cadmium-Zinc-Telluride Detector Technique
- The evolving role of molecular imaging for coronary artery disease: where do we stand today?