


Abstract
Several radiopharmaceuticals such as 18F-FDG, 123I-metaiodobenzylguanidine (MIBG), and 99mTc-tetrofosmin have demonstrated uptake in brown adipose tissue (BAT). It is important to recognize these normal variants so that they are not misinterpreted as a significant pathologic state. In addition, these radiopharmaceuticals may shed light on BAT physiology. 18F-6-fluorodopamine (F-DA) is being used as a PET radiopharmaceutical to image adrenergic innervation and suspected pheochromocytoma. Past reports have suggested that BAT is increased in pheochromocytoma patients. Methods: The images of 96 patients evaluated with 18F-F-DA or 18F-FDG PET/CT for known or suspected pheochromocytoma were reviewed retrospectively to determine whether localized uptake of a pattern typically associated with BAT was present. When available, contemporaneous images obtained using 123I-MIBG were also reviewed for the presence of BAT. Results: Of 67 patients imaged with 18F-F-DA, BAT was found in 17.9%. Of 83 patients imaged with 18F-FDG, 19.2% had BAT. Discordant findings related to uptake in BAT were often seen in patients studied with 18F-FDG, 18F-F-DA, or 123I-MIBG. Overall, 26 (27.0%) of 96 patients showed BAT on at least 1 of the 3 imaging modalities. Conclusion: 18F-F-DA can image BAT, most likely by localizing to sympathetic innervations in a manner similar to 123I-MIBG. Patients with pheochromocytoma may have a greater BAT tissue mass or activation because of elevated levels of circulating catecholamines. Quantitative PET with 18F-FDG and 18F-F-DA may have a role in in vivo studies of BAT physiology in humans or animal models.
A variety of radiopharmaceuticals used in nuclear medicine, such as 18F-FDG, 99mTc-tetrofosmin, and 123I-metaiodobenzylguanidine (MIBG), have been reported to localize in brown adipose tissue (BAT) (1–7). It is important for the physician interpreting these images to recognize these patterns so as not to confuse them with a pathologic state. Furthermore, identifying which radiopharmaceuticals localize in BAT may give insights as to their mechanism of localization and BAT physiology. BAT has an abundant supply of sympathetic nerves that are important in its physiology and that may be amenable to imaging with 18F-6-fluorodopamine (F-DA), and various studies have documented increased glucose metabolism in BAT (8). The study of BAT has attracted interest in the field of obesity (9–13) and glucose homeostasis (14). Thus, radiopharmaceuticals that can assess pathways important in BAT physiology may be useful.
It has been suggested that the incidence of BAT may be higher in patients with pheochromocytoma than in patients without (15–18). After identifying an index patient studied with 18F-F-DA who had a neck and supraclavicular activity distribution similar to that described for 18F-FDG as typical of BAT, we searched for similar 18F-F-DA, 18F-FDG, or 123I-MIBG uptake in a group of patients we had previously evaluated for pheochromocytoma. To our knowledge, this report is the first of uptake in BAT of 18F-F-DA, which is a radiopharmaceutical that has been used to image sympathetic innervations (19) and localize pheochromocytomas (20).
MATERIALS AND METHODS
This study was a retrospective review evaluating the presence of BAT in patients undergoing 18F-F-DA PET/CT imaging. 18F-F-DA was used under an investigational new drug application approved by the Food and Drug Administration. Patients were evaluated for suspected or proven pheochromocytoma in a protocol approved by the National Institute of Child Health and Human Development Institutional Review Board. All patients gave written informed consent for 18F-F-DA scans. When these patients also underwent 18F-FDG PET/CT or 123I-MIBG for clinical indications, the contemporaneous studies were also evaluated for the presence of BAT. Contemporaneous imaging studies were defined as those performed within 30 d of each other, without major intervening therapy or surgery.
We reviewed the studies of 96 patients (39 male and 57 female) who were referred for evaluation of suspected or proven pheochromocytoma. These patients underwent 18F-F-DA PET/CT or 18F-FDG PET/CT between February 2004 and May 2006 at the National Institutes of Health (NIH) Clinical Center. Their mean age was 46.6 y (range, 13–89 y). Only 2 patients were less than 18 y old. In these 96 patients, we reviewed a total of 84 18F-F-DA PET/CT studies, 93 18F-FDG PET/CT studies, and 62 123I-MIBG studies that were contemporaneous with either of the PET/CT studies. All 62 123I-MIBG studies were contemporaneous with an 18F-FDG PET/CT study, and in 34 patients, the 18F-FDG and 18F-F-DA PET/CT studies were contemporaneous. Twenty-four patients had a 123I-MIBG study contemporaneous with the 18F-F-DA study, and in 23 patients, all 3 studies were contemporaneous.
Scanning Protocols
18F-F-DA and 18F-FDG PET/CT were performed using a Discovery LS PET/CT camera (GE Healthcare) after a fast of at least 6 h (typically overnight), with approximately 37 MBq (1 mCi) of 18F-F-DA and 555 MBq (15 mCi) of 18F-FDG injected intravenously. Imaging from the skull to the proximal thigh was performed starting 10 min after radiopharmaceutical injection for 18F-F-DA and 1 h after injection for 18F-FDG. For 123I-MIBG, planar whole-body imaging and SPECT were performed at 24 h for all patients and at 48 h for selected patients after injection of about 370 MBq (10 mCi) of 123I-MIBG, on either a dual-head e-Cam γ-camera (Siemens Medical Systems), a triple-head Triad XLT γ-camera (Trionix Inc.), or a dual-head Vertex γ-camera (Philips) using a low-energy all-purpose collimator. All patients received a saturated solution of potassium iodide for thyroid blockade before 123I-MIBG injection.
Image Processing and Review
All PET data was acquired in 2-dimensional mode and reconstructed iteratively using the manufacturers' software. CT was used for attenuation correction. 123I-MIBG SPECT studies were reconstructed using filtered backprojection. All 123I-MIBG and PET datasets were reviewed in 3 orthogonal views and as rotating maximum-intensity-projection data using a MedView workstation (MedImage). Two nuclear medicine physicians reported the presence or absence of BAT in the nuchal, supraclavicular, and paravertebral regions, using the CT scan to confirm localization to adipose tissue. For 123I-MIBG studies lacking CT for coregistration, the presence of BAT was inferred from the characteristic distribution pattern. Discordance was resolved by consensus. When, occasionally, a consensus could not be achieved, a third nuclear medicine physician was consulted to resolve the findings. All readers reviewed the images of a given modality independently of the other 2 modalities and unaware of plasma catecholamine levels and final diagnosis.
The voxel values of the 18F-F-DA and 18F-FDG images were converted to standardized uptake values (SUVs) corrected for lean body mass (21), as follows: SUV = voxel activity (in Bq/mL)/[injected dose (in Bq)/gram of lean body mass].
When BAT was identified, maximum SUVs were obtained from regions of interest manually drawn on representative areas of BAT uptake, because SUVs provide some quantitative measure of the radiopharmaceutical uptake and facilitate comparison with previous 18F-FDG reports.
BAT Findings on 18F-F-DA and 18F-FDG PET/CT
To determine how frequently BAT was observed on 18F-F-DA or 18F-FDG PET/CT, we included only the first study of each type in the analysis when multiple instances of the study were performed on a single patient. The initial study was used, rather than all instances, because the initial studies would be independent of each other and thus would not bias the data through inclusion of multiple follow-up studies of the same patient.
Comparison of BAT Findings in Contemporaneous Studies Using 18F-F-DA, 18F-FDG, and 123I-MIBG
In several cases, 2 or 3 modalities (i.e., 18F-F-DA PET/CT and 18F-FDG PET/CT, 18F-FDG PET/CT and 123I-MIBG, 18F-F-DA PET/CT and 123I-MIBG, or all 3 modalities) were performed contemporaneously, without major intervening therapy or surgery. We studied the concordance of BAT findings in these studies between 18F-F-DA and contemporaneous 123I-MIBG, between 18F-F-DA and contemporaneous 18F-FDG, and between all 3 modalities when contemporaneous.
Comparison of Plasma Norepinephrine and Epinephrine Values with BAT Findings
Because circulating catecholamine levels may reflect sympathetic nervous activity with the possibility of stimulating BAT directly and/or interfering with 18F-F-DA binding, we compared BAT visualization to catecholamine levels. Contemporaneous plasma norepinephrine and epinephrine measurements performed within 3 d before or after either PET/CT study were obtained when available, and the median values were compared in patients with and without visualization of BAT. The differences between distributions of catecholamine levels in these groups were assessed for significance using the Mann–Whitney U test. The proportions of BAT positivity in patients with normal or elevated catecholamine levels were assessed for significance using the Fisher exact test.
Comparison with Final Diagnosis
Pheochromocytoma was confirmed in 65 patients on histopathologic examination. Three patients had prior pheochromocytoma and were in remission, and 1 patient could not be followed up. The remaining patients were classified as not having pheochromocytoma. BAT visualization on the 3 imaging modalities was compared with the final diagnosis and statistically assessed for significance using the Fisher exact test.
RESULTS
Detection of BAT
Review of the 18F-F-DA PET/CT studies performed on 67 patients revealed BAT in 12 studies (17.9%), with a representative study shown in Figure 1. Review of the 18F-FDG PET/CT studies performed on 83 patients revealed the presence of BAT in 16 (19.3%). Eleven (17.7%) of the 62 123I-MIBG studies demonstrated BAT. BAT was visualized on at least 1 of the 3 modalities in 26 patients (27.1%) of the total of 96 (Table 1).

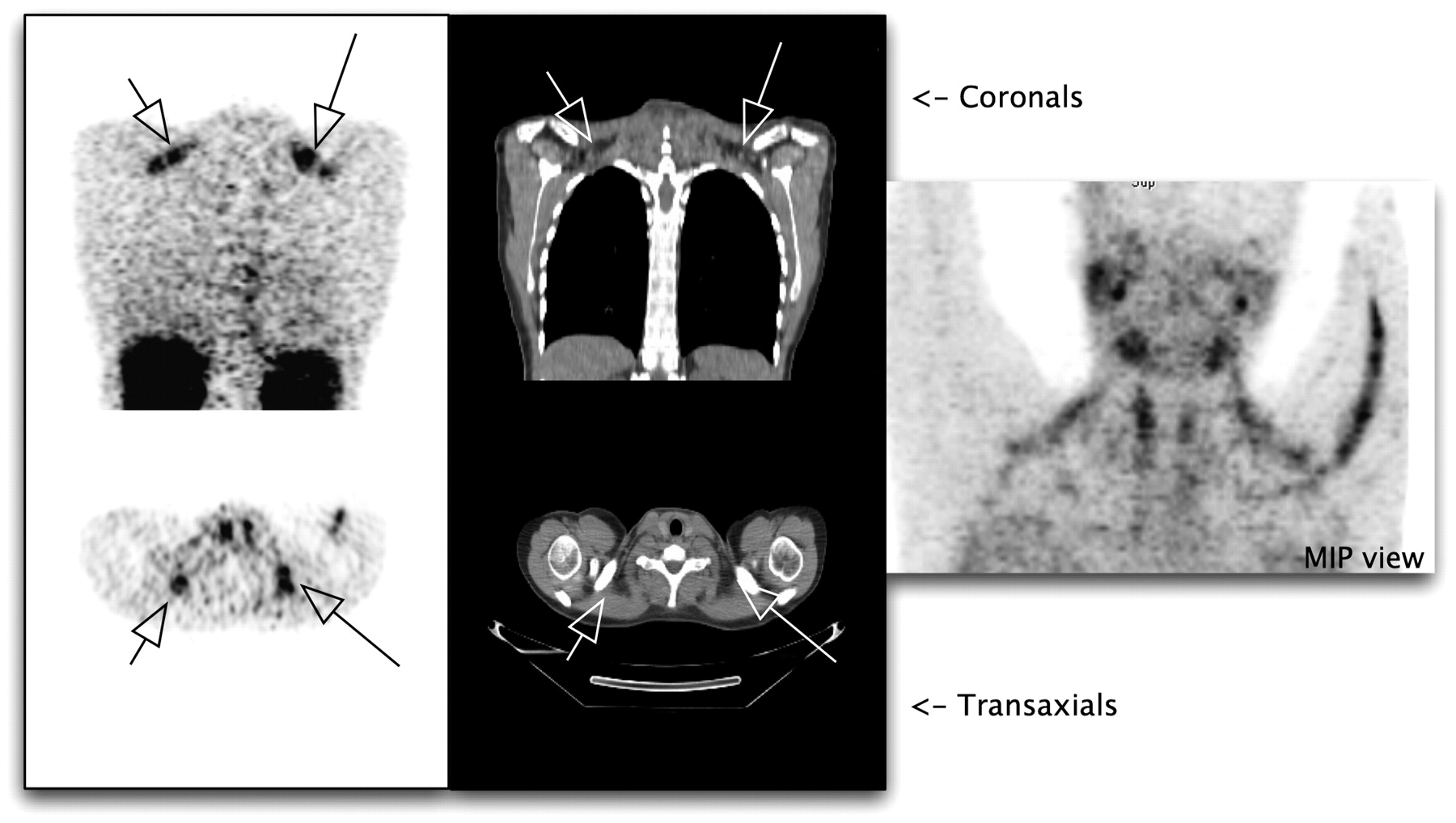
Patient 10 with pheochromocytoma showing 18F-F-DA uptake in supraclavicular BAT (black arrows) that corresponded to fat on coregistered CT (white arrows). At far right is maximum-intensity-projection image showing some uptake typical of 18F-F-DA (salivary gland, thyroid, vein in left upper extremity) and uptake in supraclavicular areas corresponding to BAT.
Patients with BAT Visualization on One or More Studies
Comparison of 18F-F-DA Findings with 18F-FDG and 123I-MIBG
Thirty-four patients underwent contemporaneous 18F-F-DA and 18F-FDG PET/CT. The presence or absence of BAT findings on these studies is depicted in Table 2. Twenty-four patients underwent contemporaneous 18F-F-DA PET/CT and 123I-MIBG; the results are shown in Table 3. Only 23 patients were contemporaneously imaged with all 3 modalities, as shown in Table 4. Of these patients, 11 were concordantly negative for BAT across all 3 modalities, whereas 6, 4, and 2 patients were positive for BAT on 1, 2, or all 3 studies, respectively. Figure 2 shows an example of BAT visualized on all 3 studies.

Maximum-intensity-projection images of patient 18 with pheochromocytoma. 18F-FDG PET (A) shows typical BAT uptake in supraclavicular region extending into axilla and paravertebral regions. 18F-F-DA PET (B) and 123I-MIBG SPECT (C) show BAT uptake in supraclavicular regions. Uptake in paraspinal regions is best seen on 18F-FDG images.
BAT Findings on 18F-F-DA and 18F-FDG Scans
BAT Findings on 18F-F-DA and 123I-MIBG Scans
BAT Findings for Patients with 3 Contemporaneous Imaging Studies
Relationship of Plasma Norepinephrine and Epinephrine Levels to 18F-F-DA and 18F-FDG
Table 5 summarizes the relationship of plasma norepinephrine and epinephrine levels to 18F-F-DA and 18F-FDG. Of patients who were BAT-positive on 18F-FDG, 75% (6/8) had elevated plasma norepinephrine levels, whereas 47% (15/32) who were BAT-negative on 18F-FDG also had elevated norepinephrine levels. However, for 18F-FDG, the median norepinephrine level was significantly higher in BAT-positive patients (P = 0.01). In contrast, 45% (5/11) of patients with BAT-positive and 72% (34/47) of those with BAT-negative 18F-F-DA scans had elevated plasma norepinephrine levels. In addition, the median plasma norepinephrine levels in the 2 groups, although elevated in both, was lower in patients who were BAT-positive on 18F-F-DA studies than in BAT-negative patients. These relationships were found to be statistically nonsignificant.
Comparison of Plasma Catecholamine Levels with BAT Findings on PET/CT
Irrespective of BAT findings in either PET study, median plasma epinephrine levels were within normal limits in all groups.
Comparison of BAT Visualization with Final Diagnosis
BAT visualization in the 65 patients who had pheochromocytoma at the time of imaging, and in 27 patients who never had pheochromocytoma, are summarized in Table 6 for each modality. The proportions were not significantly different for any modality.
BAT Visualization in All Patients, Classified by Imaging Modality and Final Diagnosis
DISCUSSION
BAT is a morphologically and functionally distinct component of the adipose organ in mammals. Histologically, BAT is characterized by small cells, multilocularity, large numbers of mitochondria, increased vascularity, and abundant sympathetic noradrenergic innervations, compared with the more widespread white adipose tissue. Norepinephrine is a key regulator of BAT that stimulates lipolysis, glucose transport, and uncoupling protein–1 expression in brown adipocytes, as well as an increase in BAT adipocyte numbers (8). The amount and distribution of BAT vary with age, nutrition, and environment (22). Thus, a radiopharmaceutical that evaluates adrenergic pathways may be of use in understanding BAT physiology.
Uptake of 18F-FDG in BAT has been well recognized (2,3,23). 18F-FDG localization in BAT can be attributed to noradrenergic stimulation through β3 receptors, resulting in increased expression of uncoupling protein–1 and increased glucose uptake. Uncoupling protein–1 is the uncoupling protein that bypasses proton-flux–driven adenosine triphosphate synthesis in the mitochondria and thereby results in thermogenesis (8). Several imaging studies have suggested the importance of sympathetic innervation in imaging of BAT with 123I-MIBG (16,24–26). Two reports have described 18F-FDG or 123I-MIBG imaging of BAT in patients with extraadrenal pheochromocytoma (27,28). In both cases, repeated imaging studies after surgical resection of pheochromocytoma showed that BAT had disappeared, suggesting that perhaps the lack of uptake on follow-up was due to resolution of the sympathetic stimuli. We postulate that the mechanism of uptake of 18F-F-DA seen in BAT may be similar to that of 123I-MIBG, given that 18F-F-DA and 123I-MIBG have similar mechanisms of uptake (19,29–31).
The incidence of accumulation in BAT in most 18F-FDG PET/CT studies has ranged from 2.3% to 6.7% (1,3,4,23), with a single 18F-FDG PET series showing an incidence of 31% of “neck and upper chest uptake” without coregistered CT (32). For 123I-MIBG, the percentage of patients with BAT visualization was reported to be 12% by Okuyama et al. in a pediatric population with neuroendocrine tumors (7). The overall incidence of BAT visualization was higher in our study than in most of the series reported to date: 19.2% with 18F-FDG, 17.9% with 18F-F-DA, and 17.7% with 123I-MIBG. Although this higher incidence may be related, in part, to our close scrutiny of the images and awareness of the BAT pattern, the 18F-FDG SUVs in our patients were in the range of those reported by Yeung et al. (4), particularly when one considers that our SUVs were corrected for lean body mass rather than body weight, which generally results in lower values for lean body mass. More likely, some of the differences in incidence were due to our patient population, namely patients with diagnosed or suspected pheochromocytoma. Patients with pheochromocytoma have been postulated by others to have an increased incidence of BAT, presumably because of the high circulating norepinephrine levels (15–18).
Although we saw 18F-FDG uptake in BAT in a higher proportion of patients with confirmed pheochromocytoma than of patients who were subsequently found not to have pheochromocytoma, this difference was not statistically significant. Interestingly, elevated catecholamines were found in a higher proportion of patients showing BAT on 18F-FDG than in BAT-negative patients, and the median catecholamine levels were significantly higher in the former group. These findings are consistent with prior reports indicating that norepinephrine activates glucose transport (33,34).
In contrast to 18F-FDG, 18F-F-DA revealed BAT in a higher proportion of patients without pheochromocytoma than of those with pheochromocytoma. Similarly, a higher proportion of patients without than with 18F-F-DA uptake in BAT had elevated norepinephrine levels, and the median norepinephrine levels were higher in the former group. Because the difference between norepinephrine levels in these 2 groups was not statistically significant, we cannot exclude that this reversal occurred by chance alone. That stated, a possible explanation could be that the elevated plasma norepinephrine levels may have competed with 18F-F-DA for norepinephrine transporter, thus reducing the uptake of 18F-F-DA in BAT. A similar inverse relationship has been found with respect to cardiac uptake of 18F-F-DA and 123I-MIBG in the presence of elevated catecholamines (35,36). Also, although pheochromocytoma was excluded in 27 patients, these patients were not necessarily healthy, many having been referred because of signs or symptoms that led to a suspicion of pheochromocytoma. Thus, although we did not see statistically significant differences in BAT visualization using 18F-FDG, 18F-F-DA, or 123I-MIBG between patients with and without pheochromocytoma, we cannot conclude that such a difference does not exist. Comparison with a group of healthy, asymptomatic subjects would be instructive.
As seen in Tables 3 and 4, visualization of BAT with different radiopharmaceuticals was often incongruent. Several factors may have contributed to this finding. Because this study was retrospective, we did not monitor or control room temperature (37) or medication use, variations in either of which could have caused real physiologic differences in BAT status.
The study of BAT has attracted interest related to the study of obesity (9–13) and glucose homeostasis (14). Thus, having 2 PET tracers (18F-FDG and 18F-F-DA) that can image different aspects of BAT physiology may be potentially useful in future in vivo quantitative studies on humans or animal models, as has been proposed by other investigators for 18F-FDG imaging of adipose tissue (38).
CONCLUSION
The fact that 18F-F-DA PET sometimes shows uptake in BAT should be kept in mind when these studies are interpreted. The proportion of our patients showing BAT on 18F-FDG PET/CT was higher than that previously reported (3,4), possibly because of the high incidence of patients with increased sympathetic stimuli and pheochromocytoma in our series. The localization of 18F-F-DA and 18F-FDG is related to 2 important processes in BAT, namely adrenergic innervations and glucose metabolism, and quantitative PET using both agents may be helpful in further understanding the physiology and regulation of brown fat.
Acknowledgments
We acknowledge the support of the technologist and radiochemistry staff of the nuclear medicine and PET departments of Warren Grant Magnusson Clinical Center, NIH. The NIH Intramural Program provided financial support.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication October 28, 2006.
- Accepted for publication April 3, 2007.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Perspectives on Brown Adipose Tissue Imaging: Insights from Preclinical and Clinical Observations from the Last and Current Century
- MECHANISMS IN ENDOCRINOLOGY: Brown adipose tissue in humans: regulation and metabolic significance
- Brown adipose tissue: a potential target in the fight against obesity and the metabolic syndrome
- Combining 123I-Metaiodobenzylguanidine SPECT/CT and 18F-FDG PET/CT for the Assessment of Brown Adipose Tissue Activity in Humans During Cold Exposure
- First Report of Harlequin Syndrome as the Presenting Feature of Carney Triad: A Diagnostic and Imaging Challenge
- Brown Adipose Tissue: Mechanisms and Potential Therapeutic Targets
- Modern Nuclear Imaging for Paragangliomas: Beyond SPECT