


Abstract
Recent studies suggest a somewhat selective uptake of O-(2-[18F]fluoroethyl)-l-tyrosine (FET) in cerebral gliomas and in squamous cell carcinoma (SCC) and a good distinction between tumor and inflammation. The aim of this study was to investigate the diagnostic potential of 18F-FET PET in patients with SCC of the head and neck region by comparing that tracer with 18F-FDG PET and CT. Methods: Twenty-one patients with suspected head and neck tumors underwent 18F-FET PET, 18F-FDG PET, and CT within 1 wk before operation. After coregistration, the images were evaluated by 3 independent observers and an ROC analysis was performed, with the histopathologic result used as a reference. Furthermore, the maximum standardized uptake values (SUVs) in the lesions were determined. Results: In 18 of 21 patients, histologic examination revealed SCC, and in 2 of these patients, a second SCC tumor was found at a different anatomic site. In 3 of 21 patients, inflammatory tissue and no tumor were identified. Eighteen of 20 SCC tumors were positive for both 18F-FDG uptake and 18F-FET uptake, one 0.3-cm SCC tumor was detected neither with 18F-FDG PET nor with 18F-FET PET, and one 0.7-cm SCC tumor in a 4.3-cm ulcer was overestimated as a 4-cm tumor on 18F-FDG PET and missed on 18F-FET PET. Inflammatory tissue was positive for 18F-FDG uptake (SUV, 3.7–4.7) but negative for 18F-FET uptake (SUV, 1.3–1.6). The SUVs of 18F-FDG in SCC were significantly higher (13.0 ± 9.3) than those of 18F-FET (4.4 ± 2.2). The ROC analysis showed significantly superior detection of SCC with 18F-FET PET or 18F-FDG PET than with CT. No significant difference (P = 0.71) was found between 18F-FDG PET and 18F-FET PET. The sensitivity of 18F-FDG PET was 93%, specificity was 79%, and accuracy was 83%. 18F-FET PET yielded a lower sensitivity of 75% but a substantially higher specificity of 95% (accuracy, 90%). Conclusion: 18F-FET may not replace 18F-FDG in the PET diagnostics of head and neck cancer but may be a helpful additional tool in selected patients, because 18F-FET PET might better differentiate tumor tissue from inflammatory tissue. The sensitivity of 18F-FET PET in SCC, however, was inferior to that of 18F-FDG PET because of lower SUVs.
Head and neck carcinoma constitutes approximately 5% of all malignancies, and its frequency is increasing (1). Squamous cell carcinoma (SCC) is the major histologic type of neoplasm arising from the head and neck area (2). The effectiveness of surgical treatment depends on the complete excision of all tumor tissue, and accurate preoperative staging is therefore mandatory. Detection of extension into adjacent tissues and structures is important and is usually done by anatomic imaging techniques, for example, CT and MRI. However, discrimination between tumor and reactive tissue changes may be difficult based solely on morphologic criteria (3). The sensitivity of anatomic imaging ranges from 67% to 88%, and the specificity, from 50% to 75% (4).
PET using 2-18F-FDG has been applied in many studies as an alternative imaging method and has been observed to improve preoperative diagnosis, with a sensitivity of 80%–100% for the detection of primary tumors, tumor recurrences, and occult metastases (4–10). 18F-FDG, however, is not specific for cancer cells and exhibits high uptake in macrophages, fibroblasts, and granulation tissue (11,12). Thus, some studies report a specificity of only 60% for 18F-FDG PET, especially after radiotherapy (6,13–16).
Radiolabeled amino acids such as l-[methyl-11C]methionine (MET) and l-1-[11C]-tyrosine (TYR), which are less avidly metabolized by inflammatory cells (17,18), have been explored as an alternative tracer for PET studies in patients with head and neck cancer. High sensitivity for the detection of these tumors has been reported for both tracers, and a specificity of 100% has been claimed especially for 11C-TYR (18,19). Because of the short physical half-life of the 11C label (20 min), however, 11C-MET and 11C-TYR remain restricted to a few PET centers with a cyclotron on site and cannot become established in routine clinical practice.
Amino acids labeled with 18F (half-life, 110 min), such as O-(2-[18F]fluoroethyl)-l-tyrosine (FET), are presently under investigation in order to overcome the logistic disadvantages of 11C-labeled amino acids. 18F-FET can be synthesized with high radiochemical yields and can be produced on a large scale for clinical purposes (20,21). This artificial amino acid is not incorporated into proteins but exhibits high uptake in tumor cells because of increased transport via the amino acid transport systems L and B0,+ (20,22). 18F-FET has successfully been applied to brain tumors, and convincing results have been reported for imaging the extent of gliomas, detecting recurrences, and differentiating gliomas from benign lesions (23–27). In addition, animal experiments have shown that 18F-FET, in contrast to 18F-FDG and 11C-MET, exhibits no uptake in inflammatory cells or in inflammatory lymph nodes, thus promising a higher specificity for the detection of tumor cells (28,29).
Recently, we studied the diagnostic performance of 18F-FET PET in different types of peripheral tumors (30). Surprisingly, no uptake of 18F-FET could be detected in the majority of peripheral tumors, especially in lymphomas and most adenocarcinomas. This finding is in contrast to the results with other tyrosine derivatives (30). Most peripheral tumors that showed a high accumulation of 18F-FET turned out to be SCC tumors.
The purpose of this study was to further investigate the diagnostic potential of 18F-FET PET in patients with SCC of the head and neck region by comparing that tracer with 18F-FDG PET and conventional morphologic imaging using CT.
MATERIALS AND METHODS
Patients
Twenty-one consecutive patients (3 women and 18 men; age range, 41−80 y; mean, 61 y) with suspected squamous head and neck cancer participated in this study. Data for the individual patients are given in Table 1. The mean size of the carcinoma tumors (n = 20) was 3.3 ± 2.1 cm (range, 0.3–8.3 cm), and that of the lymph node metastases (n = 5) was 1.1 ± 0.6 cm (range, 0.2−1.8 cm). The study was approved by the university ethics committee and by federal authorities. All subjects gave written informed consent to participate in the study.
Data for Individual Patients and SUVs for 18F-FDG and 18F-FET in Primary Lesions
Histopathologic Examination
All resected tissues were exactly localized and documented at each level to allow correlation between histopathologic findings and preoperative imaging results. Classification of the primary tumor and regional lymph node metastases was based on the TNM system (31).
Radiopharmaceuticals
The amino acid derivative 18F-FET was produced via anion-activated nucleophilic 18F-fluorination of N-trityl-O-(2-tosyl-oxyethyl)-l-tyrosine tert-butyl ester and subsequent deprotection. The uncorrected yield was about 35% at a specific radioactivity of greater than 200 GBq/μmol and radiochemical purity of greater than 98% by optimizing our previous method (32). The tracer was administered as an isotonic neutral solution.
18F-FDG was synthesized as previously described (32). The average specific radioactivity was greater than 200 GBq/μmol.
PET
All patients fasted for at least 12 h before the PET studies. PET scanning started 1 h after intravenous injection of 370 MBq of 18F-FET. Within 1 wk, all patients underwent comparative investigations using the same scanning protocol. Blood glucose levels were checked before 18F-FDG injection to ensure that they were less than 130 mg/dL.
The studies were performed on an ECAT EXACT HR+ scanner (CTI; optimum full width at half maximum, 4.5 mm; 15-cm transaxial field of view). For attenuation correction, transmission scans with three 68Ge/68Ga rotating line sources were used. After correction for random and scattered coincidences, dead time, and decay, image data were obtained by iterative reconstruction. Data were reconstructed with the manufacturer-supplied attenuation-corrected ordered-subsets expectation maximization algorithm including attenuation correction as described previously (30).
CT
Contrast-enhanced CT was performed as a routine preoperative procedure in all patients within 1 wk. Using a helical CT scanner (Somatom Plus 4; Siemens; slice thickness, 3 mm; pitch, 1.5; current, 100 mAs; potential, 120 kV), scans were acquired from the base of the skull to the apex of the chest.
Data Analysis
The data were evaluated after coregistration of the 18F-FET PET, 18F-FDG PET, and CT scans using dedicated software (MPI tool, version 3.28; ATV) (33).
First, similarly sized regions of interest were placed over the lesions on coregistered 18F-FDG and 18F-FET PET scans. Standardized uptake values (SUVs) of 18F-FET and 18F-FDG were calculated by dividing the maximum radioactivity (kBq/mL) of the regions of interest by the radioactivity injected per gram of body weight in the corresponding PET scans. For comparison of 18F-FET SUVs with 18F-FDG SUVs, the nonparametric U test of Mann and Whitney was used.
Second, we performed an alternative free-response receiver-operating-characteristic (ROC) analysis, which somewhat reflected the decision process in routine clinical practice and allowed for recording of the degree of confidence in making a decision. 18F-FET PET, 18F-FDG PET, and CT images were presented separately to 3 observers, each of whom was a nuclear medicine and radiology specialist and experienced in CT and PET reading. The images were randomly assigned to each observer, who had no knowledge of clinical information. In the first session, the observers reviewed the CT images, in the second session the 18F-FDG PET images, and in a third session the 18F-FET PET images.
For each patient, the observers evaluated 5 anatomic regions or levels (level 1, nasopharynx; level 2, oropharynx; level 3, hypopharynx/larynx; region 4, right cervical lymph nodes; region 5, left cervical lymph nodes), making 315 decisions on the presence of tumor on the presented images. Each observer recorded suspected lesions and gave each level a confidence rating based on a 6-point scale as follows: 6, definitely positive (when an observer was convinced that a lesion was a tumor); 5, probably positive (when an observer was not convinced that a lesion was a tumor but found it substantially likely to be a tumor); 4, possibly positive (when an observer was nearly undecided but tended to classify a lesion as being a tumor); 3, possibly negative (when an observer was nearly undecided but tended to classify a lesion as not being a tumor); 2, probably negative (when an observer was not convinced that a lesion was not a tumor but found it substantially likely to be nontumor tissue); and 1, definitely negative for tumor tissue (when an observer was convinced that there was no tumor). For the determination of sensitivity, specificity, and accuracy, a rating score of 4 or greater was considered positive for tumor tissue. Composite ROC curves were used to represent the performance of all observers as a group and were calculated by averaging the scores assigned by each of the observers. Alternative free-response ROC curves were generated for each imaging modality. The diagnostic accuracies were determined by calculating the area under the ROC curve (Az) using dedicated ROC evaluation software (Rockit 0.9B; Charles E. Metz, University of Chicago). Differences between ROC curve integrals were tested for significance using the 2-tailed area test (a univariate z score test of the difference between the Az values, with the null hypothesis that the datasets arose from binominal ROC curves with equal areas beneath them). Probability values of less than 0.05 were considered significant.
RESULTS
18F-FET and 18F-FDG Uptake
In 18 of 21 patients, histologic examination revealed SCC, and in 2 of these patients, a second SCC tumor was found at a different anatomic site. In 3 of 21 patients, inflammatory tissue and no tumor were identified by histology. Detailed data for each patient are given in Table 1. Eighteen of 20 SCC tumors were positive for 18F-FDG and 18F-FET uptake (Fig.1). One 0.3-cm tumor was detected neither with 18F-FDG PET nor with 18F-FET PET. In a different patient, histologic examination showed a 0.7-cm tumor in a 4.3-cm inflammatory ulcer (Fig. 2). The 18F-FDG PET scan overestimated the carcinoma as a 4-cm lesion with increased 18F-FDG uptake (SUV, 5.2), and the scan obtained with 18F-FET (SUV, 1.5) missed this small carcinoma. All carcinomas with increased 18F-FET uptake exhibited concordant 18F-FDG accumulation, and no additional lesion could be identified with 18F-FET PET. The SUVs for SCC were higher in all cases with 18F-FDG than with 18F-FET; the mean SUV for 18F-FDG was 13.0 ± 9.3 (range, 1.8–44.3) and that for 18F-FET was 4.4 ± 2.2 (range, 0.9–9.2) (P < 0.001). In the lymph node metastases (n = 5), with an average size of 1.1 ± 0.6 cm, no increased 18F-FET uptake could be identified (mean SUV, 1.4 ± 0.3; range, 1.0–1.9). The corresponding SUV for 18F-FDG uptake ranged from 1.6 to 3.3 (mean, 2.3 ± 0.7); 2 of 5 lymph node metastases had an SUV above 2.5 and 3 of 5 had an SUV below 2.5. Important to note is that inflammatory tissue showed an increased uptake of 18F-FDG, with the SUV increasing from 3.7 to 4.7, which is within the range of 18F-FDG uptake in SCC. In contrast, no increased accumulation of 18F-FET was found in inflammatory tissue (SUV range, 1.3–1.6) (Fig. 3).

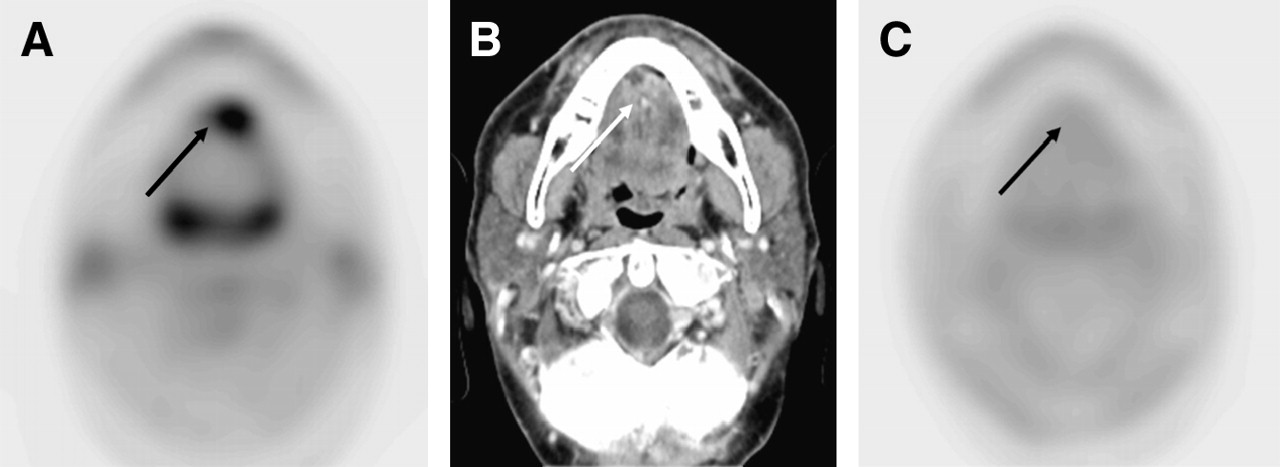
18F-FDG PET (A), CT (B), and 18F-FET PET (C) images of 72-y-old man with SCC of oral cavity (arrows). Tumor exhibits increased uptake of 18F-FDG (SUV, 8.0) and 18F-FET (SUV, 3.6).

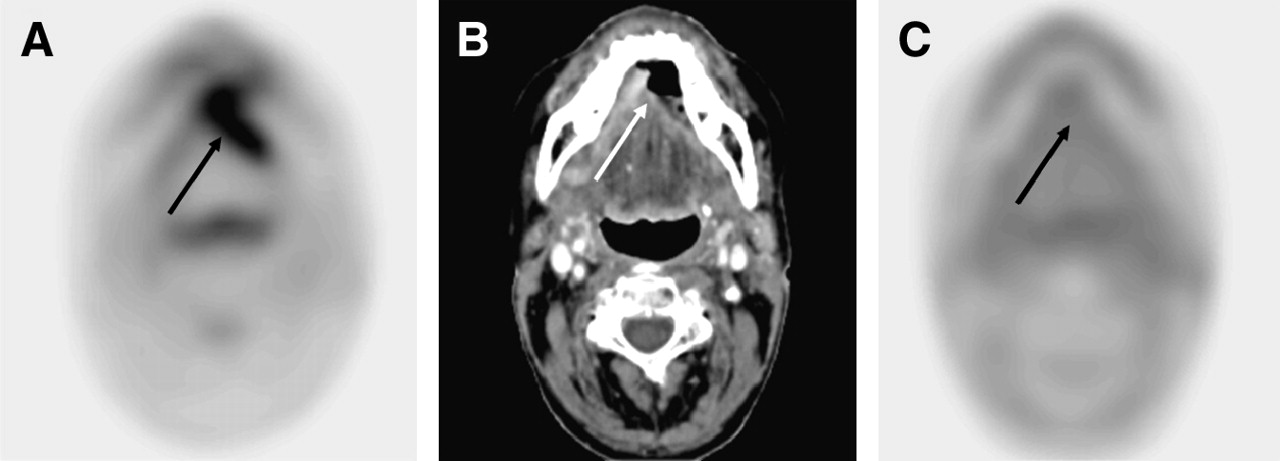
18F-FDG PET (A), CT (B), and 18F-FET PET (C) images of 52-y-old man with 0.7-cm SCC in 4.3-cm ulcer with inflammatory tissue (arrows). 18F-FDG PET scan shows approximately 4-cm lesion with increased 18F-FDG uptake (SUV, 5.2) that allows no discrimination between carcinoma and inflammation. CT scan demonstrates air-filled ulcer, and 18F-FET PET scan reveals no abnormal 18F-FET uptake (SUV, 1.5), missing the small carcinoma.
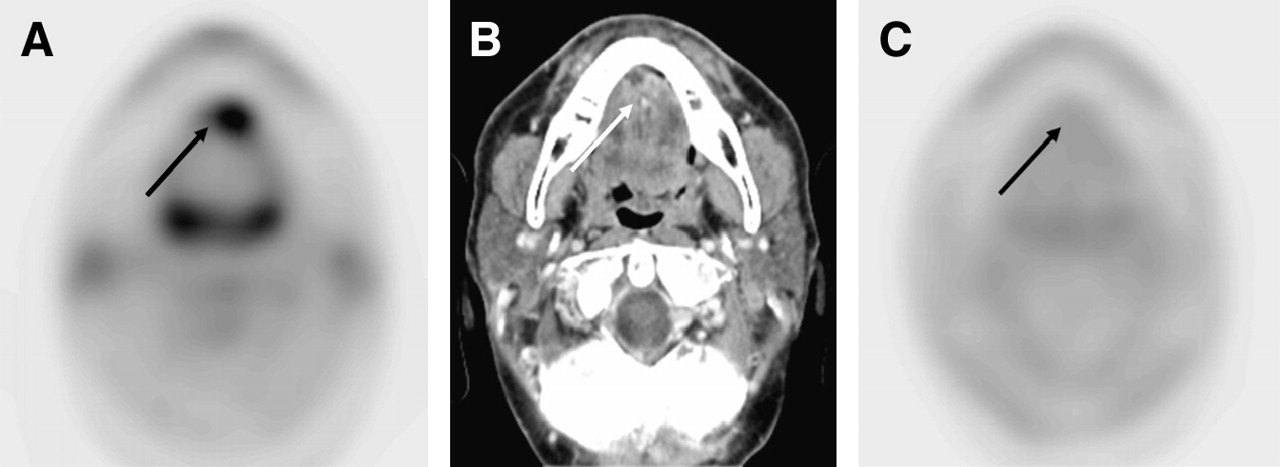
18F-FDG PET (A), CT (B), and 18F-FET PET (C) images of 50-y-old man with chronic inflammatory tissue (arrows). 18F-FDG PET scan shows lesion with increased 18F-FDG uptake (SUV, 4.7) suggesting malignancy. 18F-FET PET was true negative, with no increased 18F-FET uptake (SUV, 1.3).
ROC Analysis
The alternative free-response ROC curves formed on the basis of pooled data from the 3 observers are shown in Figure 4. The Az values for CT, 18F-FET PET, and 18F-FDG PET were 0.82, 0.93, and 0.95, respectively.

Composite ROC curves of the 3 observers. Az values for CT, 18F-FET PET, and 18F-FDG PET were 0.82, 0.93, and 0.95, respectively. Accuracy of observers did not significantly differ (P = 0.71) between 18F-FDG and 18F-FET PET but, in the distinction of carcinomas, was significantly (P < 0.05) greater with either technique than with CT.
Detection of SCC was significantly (P < 0.05) better using 18F-FET PET or 18F-FDG PET than using routine anatomic imaging with CT. For 18F-FDG PET and 18F-FET PET, no significant difference (P = 0.71) in Az values could be identified.
When a rating of 1–3 on the 6-point rating scale was considered negative for tumor tissue and a rating of 4 or higher was considered positive for tumor tissue, the sensitivity of 18F-FDG PET was 93% but specificity was only 79% (accuracy, 83%). 18F-FET PET yielded a lower sensitivity of 75% but a substantially higher specificity of 95% (accuracy, 90%). CT achieved a sensitivity of 64%, a specificity of 86%, and the lowest accuracy, 80%.
DISCUSSION
The aim of this prospective study was to explore the diagnostic potential of 18F-FET PET in patients with primary SCC of the head and neck region by comparing that tracer with 18F-FDG PET and CT. Detection of SCC was not better with 18F-FET PET than with 18F-FDG PET, and no significant difference in accuracy was identified in an ROC analysis. An important finding was that the specificity of 18F-FET PET for the detection of SCC was superior to that of 18F-FDG PET and CT. We suggest that this difference is caused by the increased uptake of 18F-FDG in physiologic tissue of the head and neck region and in inflammatory tissue. In contrast to 18F-FDG, 18F-FET was not taken up by inflammatory tissue—an observation that is in line with the results of animal experiments (28,29) and with our observations in a previous study (30) (Fig. 3). A drawback of 18F-FET PET, however, was the low sensitivity, only 75%, in this series of patients. The differences in sensitivity and specificity may be attributed partly to the relatively low 18F-FET uptake in the tumors. This low uptake leads to a poorer detection rate, especially in small tumors, which are missed because of partial-volume effects. All larger SCC tumors confirmed our previous findings (30) by demonstrating an increased uptake of 18F-FET. However, the higher sensitivity of 18F-FDG in SCC may also be influenced by the high tracer uptake in the concomitant inflammation, as is nicely illustrated in the case of patient 1 (Fig. 2). In that patient, a 0.7-cm tumor was found in a 4.3-cm ulcer and, because of high uptake in the inflammatory process, was rated positive for 18F-FDG uptake whereas 18F-FET PET was negative.
The reason for the somewhat selective accumulation of 18F-FET in certain tumor types and the low uptake in inflammatory tissue has not yet been fully explained. In a previous study, we speculated that a selective transport of 18F-FET via subtype 2 of the L-type amino acid transporter (LAT) might account for this phenomenon (30). A study expressing different subtypes of LAT in Xenopus oocytes has shown that the natural amino acid l-tyrosine is transported by both subtype 1 and subtype 2 (34). Another study demonstrated that 18F-FET influx via subtype 1 is poor, indicating that LAT-like transport may occur mainly via subtype (35). This transporter subtype, however, appears not to be expressed in inflammatory tissue (36), possibly explaining the low uptake of 18F-FET in such tissue.
The observation of a higher selectivity of 18F-FET for certain amino acid transporters compared with its natural parent is a rather interesting finding. A similar phenomenon has been observed for the radioiodinated tyrosine derivative L-3-123I-iodo-α-methyl-tyrosine, which is selectively transported by subtype 1 of LAT (34). The further development of such amino acids may help in the exploration of dysregulations of specific amino acid transporters and their involvement in the pathogenesis of various diseases.
Although the SUVs for 18F-FET were significantly lower than those for 18F-FDG, the uptake values were similar to those reported for 11C-TYR PET, for which a sensitivity and specificity of 100% for the detection of SCC of the head and neck region has recently been claimed by a group of investigators (18,37). An earlier publication on SCC by the same group, however, reported that 11C-TYR accumulated in several lymph nodes that were normal on histopathologic examination (38). Thus, some doubt of the high specificity of 11C-TYR accumulation in SCC appears warranted, and additional uptake in concomitant inflammation has to be considered. Furthermore, high uptake in the salivary glands constitutes a major problem for 11C-TYR PET and 11C-MET PET and makes the detection of tumors near these glands difficult (18,39). Recent studies have reported that, because of high unspecific uptake and overestimation of tumor volumes, 11C-MET PET was not helpful in determining tumor volumes for the planning of radiation therapy for head and neck tumors (40). The high uptake of 11C-TYR and 11C-MET in the salivary glands might be explained by the fact that these tracers are incorporated into proteins that are synthesized in large amounts in these glands. In contrast, 18F-FET is not incorporated into proteins, and no uptake was noted in the salivary glands.
Because uptake and sensitivity are lower for 18F-FET than for 18F-FDG, 18F-FET does not represent an ideal tracer for the evaluation of primary SCC of the head and neck region. Also, the detection rate of 18F-FET PET for lymph nodes in the present study appeared to be lower than that of 18F-FDG PET, although the number of positive lymph nodes in this series of patients was too small to allow for definitive conclusions. Nevertheless, the higher specificity makes 18F-FET PET an interesting additional tool in the follow-up of patients with SCC. A possible application of 18F-FET PET may be the monitoring of radio- or chemotherapy of SCC, because the reaction of the tumor tissue may be specifically detected without the interfering uptake by inflammatory or reactive tissue. Especially in pretreated patients in whom CT or MRI cannot differentiate a recurrent tumor from reactive changes, a reliable noninvasive imaging method may be helpful. Although a biopsy should be performed in cases of clinical suspicion, repeatedly negative biopsies may not exclude the presence of viable tumor, and the trauma caused by biopsies on irradiated tissue may initiate infection, further edema, and failure to heal (5). Further clinical studies are needed to elucidate the possible role of 18F-FET PET in this context.
CONCLUSION
18F-FET may not replace 18F-FDG in the PET diagnostics of head and neck cancer but may be a helpful additional tool in selected patients by allowing better differentiation of tumor tissue from inflammatory tissue. The sensitivity of 18F-FET PET in SCC, however, was inferior to that of 18F-FDG PET because of lower SUVs.
Acknowledgments
The authors thank Bettina Palm, Erika Wabbals, and Silke Grafmüller for technical assistance in the radiosynthesis of 18F-FET, and Elisabeth Theelen and Suzanne Schaden for assistance with patient studies and data analysis.
References
- Received for publication July 20, 2005.
- Accepted for publication October 31, 2005.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- First Clinical Results of (D)-18F-Fluoromethyltyrosine (BAY 86-9596) PET/CT in Patients with Non-Small Cell Lung Cancer and Head and Neck Squamous Cell Carcinoma
- Pituitary Incidentaloma Found on O-(2-18F-Fluoroethyl)-L-Tyrosine PET
- Innovations in Radiotherapy Planning of Head and Neck Cancers: Role of PET
- Radiopharmaceuticals in Preclinical and Clinical Development for Monitoring of Therapy with PET
- Tumor Cell Metabolism Imaging
- Differential Uptake of O-(2-18F-Fluoroethyl)-L-Tyrosine, L-3H-Methionine, and 3H-Deoxyglucose in Brain Abscesses
- FDG-PET/CT in restaging of patients with recurrent breast cancer: possible impact on staging and therapy
- Nuclear Imaging Probes: from Bench to Bedside
- Differential Roles of 18F-FDG PET in Patients with Locoregional Advanced Nasopharyngeal Carcinoma After Primary Curative Therapy: Response Evaluation and Impact on Management
- 18F-FET PET Differentiation of Ring-Enhancing Brain Lesions