


Article Figures & Data
Figures
- FIGURE 1.
A 43-y-old woman with normal whole-body distribution on 11C-HED PET scan (several levels of coronal slices) with high 11C-HED accumulation in renal pelvis, ureter, urinary bladder, myocardium, liver, thyroid, and pancreas and moderate tracer uptake in salivary glands and spleen. Adrenal glands demonstrate only very low 11C-HED uptake and can only be differentiated from surrounding tissue by using PET/CT fusion image.
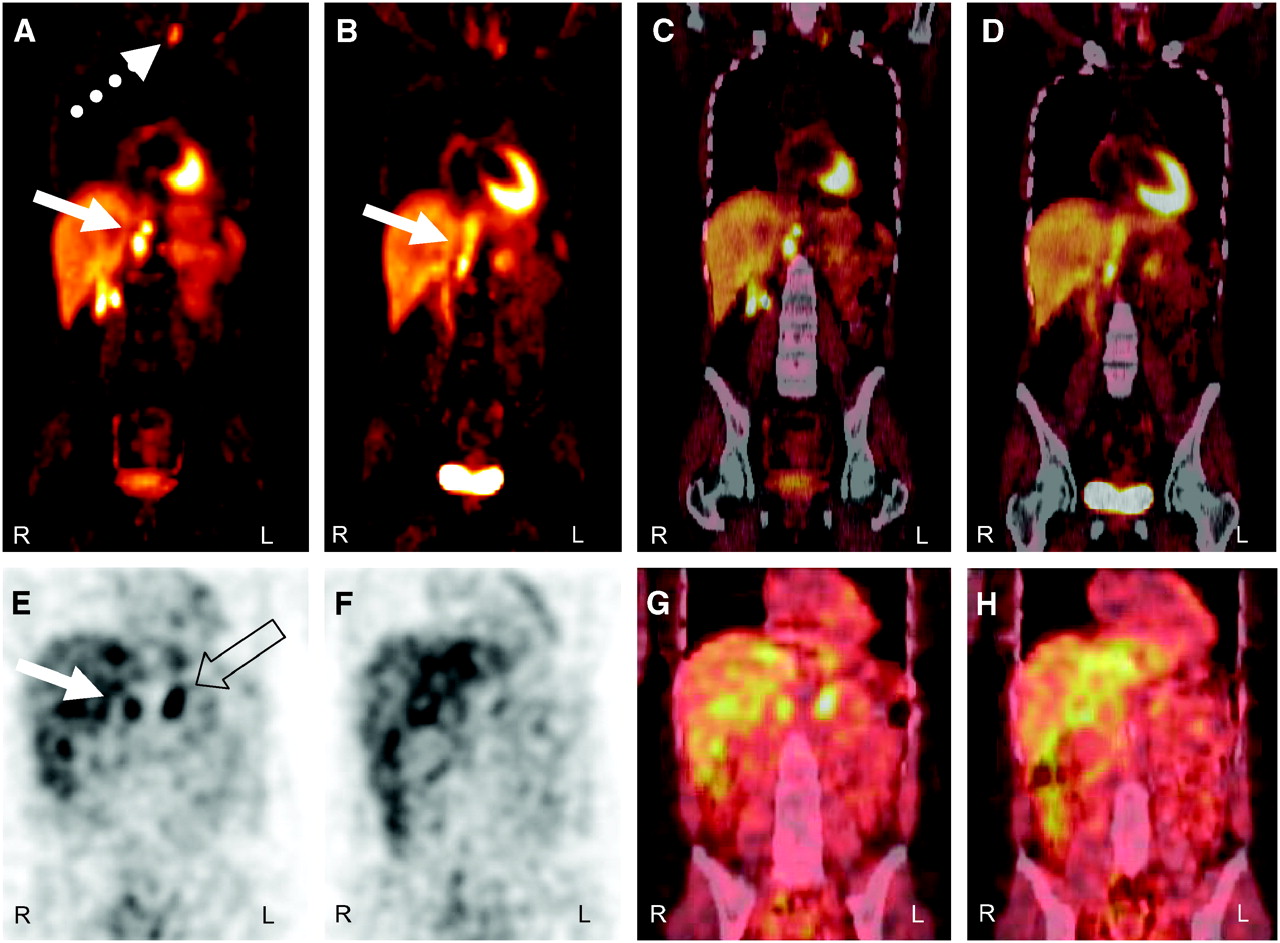
- FIGURE 2.
A 33-y-old woman (patient HA) who had pheochromocytoma of right adrenal gland and resection years ago. 11C-HED PET/CT: (A and B) PET images; (C and D) PET/CT fusion images, 2 levels of coronal slices. There is local relapse (solid arrow) and metastases retrocrural (solid arrow), cervical (dotted arrow), and mediastinal (not shown) with highly increased tracer uptake. 11C-HED uptake of left adrenal gland is very low. 123I-MIBG SPECT/CT: (E and F) SPECT images; (G and H) SPECT/CT fusion images, 2 levels of coronal slices. There is moderately increased tracer uptake in local relapse (solid arrow) and physiologic uptake in left adrenal gland (open arrow). Retrocrural metastases are not visible with increased 123I-MIBG accumulation. Cervical and mediastinal metastases are not within field of view of SPECT.
- FIGURE 3.
A 57-y-old man (patient GP) with metastatic paraganglioma. Primary tumor (open arrows) in left paravertebral region with involvement of 10th thoracic vertebral body and osseous metastasis in right iliac bone (solid arrows) demonstrate moderately increased 11C-HED uptake in PET/CT: (A) PET, coronal slice; (B) PET/CT fusion image, coronal slice. 123I-MIBG SPECT/CT: (C) SPECT, coronal slice; (D) SPECT/CT fusion image, coronal slice. Very high tracer uptake is evident in primary tumor and only faintly increased tracer uptake is seen in osseous metastasis.
- FIGURE 4.
A 5-y-old girl (patient EN) who had neuroblastoma stage IV 3 y ago. Large local relapse in left upper abdomen does not demonstrate increased 11C-HED uptake above surrounding tissue in PET/CT: (A) PET, coronal slice; (B) PET/CT fusion, coronal slice; (C) PET, transversal slice; (D) CT, transversal slice; (E) gadolinium-enhanced T1-weighted MRI with fat saturation, transversal slice. Osseous metastasis (solid arrows in A and B) in left hemipelvis is visible with faintly increased tracer uptake. 123I-MIBG SPECT/CT: (F) SPECT, coronal slice; (G) SPECT/CT fusion, coronal slice. Local relapse (open arrows) and osseous metastasis (solid arrows) show highly increased 123I-MIBG accumulation. Neuroblastoma was confirmed histologically at first diagnosis 3 y ago. In relapse situation, osseous involvement was confirmed by bone marrow puncture. Additionally, patient showed increased urinary catecholamines at first diagnosis and in relapse situation.




Tables
Patient* Age (y) Sex Histology Primary tumor Metastases Indication BM 37 M Pheochromocytoma After resection Soft tissue Relapse, restaging ES 40 M Pheochromocytoma Adrenal glands, bilateral Soft tissue Staging, MEN IIa HA1 33 F Pheochromocytoma After resection, local relapse Soft tissue Relapse, restaging HA2 33 F Pheochromocytoma After resection, local relapse Soft tissue Follow-up after operation SI 66 F Pheochromocytoma Adrenal gland No Staging BA 51 F Pheochromocytoma After resection Soft tissue Progression, restaging EN 5 F Neuroblastoma After resection Soft tissue, bone Relapse, restaging SL 4 M Neuroblastoma Adrenal gland/abdomen Bone Staging BV1 6 F Neuroblastoma After resection Soft tissue, bone Relapse, restaging BV2 6 F Neuroblastoma After resection Soft tissue, bone Follow-up after therapy BR 2 F Neuroblastoma Adrenal gland/abdomen Soft tissue Follow-up after therapy WJ 9† M Neuroblastoma Adrenal gland/abdomen No Staging KL 2 M Neuroblastoma Adrenal gland/abdomen Bone Staging KS1 23 F Ganglioneuroblastoma After resection Soft tissue Relapse, restaging KS2 24 F Ganglioneuroblastoma After resection Soft tissue Follow-up after therapy KS3 24 F Ganglioneuroblastoma After resection Soft tissue Follow-up after therapy OJ 59 M Paraganglioma After resection Soft tissue, bone Progression, restaging GP1 57 M Paraganglioma Paravertebral Soft tissue, bone Progression, restaging GP2 57 M Paraganglioma Paravertebral Soft tissue, bone Follow-up after therapy Organ or tissue SUVmax SUVmean Salivary gland 8.8 ± 2.8 4.7 ± 0.8 Thyroid (n = 4) 12.8 ± 5.1 5.5 ± 1.6 Lung 2.5 ± 0.8 1.6 ± 0.4 Myocardium (L ventricle) 9.9 ± 2.8 5.6 ± 1.4 Liver 9.0 ± 2.7 5.3 ± 1.2 Spleen 5.0 ± 1.0 4.1 ± 0.8 Pancreas 11.5 ± 3.3 6.2 ± 1.1 Adrenal gland 4.9 ± 2.7 3.2 ± 1.7 Kidney, parenchyma 6.0 ± 1.4 4.4 ± 1.7 Kidney, pelvis 36.7 ± 8.8 13.7 ± 2.6 Ureter 15.4 ± 10.9 5.5 ± 3.9 Urinary bladder 148.7 ± 82.5 64.9 ± 20.3 Bowel 2.6 ± 0.8 1.5 ± 0.1 Vertebral body 2.8 ± 0.8 1.6 ± 0.4 Long bone 0.8 ± 0.1 0.5 ± 0.1 Muscle 1.5 ± 0.3 0.6 ± 0.2 Data are expressed as mean ± SD.
11C-HED PET 123I-MIBG SPECT Tumor or localization TP FP FN TP FP FN Neuroblastoma 25 0 1* 26 0 0 Pheochromocytoma 21 0 0 17 0 4 Paraganglioma 27 0 0 26 0 1 Ganglioneuroblastoma 7 0 0 6 0 1 Osseous 19 0 0 19 0 0 Soft tissue 61 0 1* 56 0 6 Total 80 0 1* 75 0 6 ↵* No increased 11C-HED uptake in large local relapse. In low-dose CT, large tumor mass is visible.
TP = true-positive; FP = false-positive; FN = false-negative.
Lesion localization (no.) Median or quantile SUVmax SUVmean Total (81)* Median 8.9 4.3 25th quantile 4.3 2.3 75th quantile 15.0 7.9 Osseous (19) Median 3.4 1.9 25th quantile 2.8 1.6 75th quantile 5.4 3.7 Soft tissue (62)* Median 10.9 6.1 25th quantile 5.5 3.3 75th quantile 16.4 8.7 ↵* SUVs were also calculated for large neuroblastoma relapse that was missed in visual analysis of 11C-HED PET.
Tumor Localization HED > MIBG MIBG > HED HED = MIBG Total Neuroblastoma Osseous 2 2 8 12 Soft tissue 2 10 2 14 Pheochromocytoma Osseous 0 0 0 0 Soft tissue 9 2 10 21 Paraganglioma Osseous 6 0 1 7 Soft tissue 2 2 16 20 Ganglioneuroblastoma Osseous 0 0 0 0 Soft tissue 5 0 2 7 Total Osseous 8 2 9 19 Soft tissue 18 14 30 62 Total 26 16 39 81





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Norepinephrine Transporter as a Target for Imaging and Therapy
- Modern Nuclear Imaging for Paragangliomas: Beyond SPECT
- Usefulness of 123I-MIBG Scintigraphy in the Evaluation of Patients with Known or Suspected Primary or Metastatic Pheochromocytoma or Paraganglioma: Results from a Prospective Multicenter Trial
- 123I-MIBG Scintigraphy and 18F-FDG PET in Neuroblastoma
- SPECT/CT
- Role of positron emission tomography and bone scintigraphy in the evaluation of bone involvement in metastatic pheochromocytoma and paraganglioma: specific implications for succinate dehydrogenase enzyme subunit B gene mutations
- Significant Benefit of Multimodal Imaging: PET/CT Compared with PET Alone in Staging and Follow-up of Patients with Ewing Tumors
- Imaging hNET Reporter Gene Expression with 124I-MIBG
- The role of 6-[18F]fluorodopamine positron emission tomography in the localization of adrenal pheochromocytoma associated with von Hippel-Lindau syndrome