


Abstract
The purpose of this study was to compare the diagnostic utility of 123I-metaiodobenzylguanidine (123I-MIBG) scintigraphy and 18F-FDG PET in neuroblastoma. Methods: A total of 113 paired 123I-MIBG and 18F-FDG PET scans in 60 patients with neuroblastoma were retrospectively reviewed. Paired scans were acquired within 14 days of each other. Results: For stage 1 and 2 neuroblastoma (13 scans, 10 patients), 18F-FDG depicted more extensive primary or residual neuroblastoma in 9 of 13 scans. 123I-MIBG and 18F-FDG showed equal numbers of lesions in 1 of 13 scans, and 3 of 13 scan results were normal. For stage 3 neuroblastoma (15 scans, 10 patients), 123I-MIBG depicted more extensive primary neuroblastoma or local or regional metastases in 5 of 15 scans. 18F-FDG depicted more extensive primary neuroblastoma or local or regional metastases in 4 of 15 scans. 123I-MIBG and 18F-FDG were equal in 2 of 15 scans, and 4 of 15 scan results were normal. For stage 4 neuroblastoma (85 scans, 40 patients), 123I-MIBG depicted more neuroblastoma sites in 44 of 85 scans. 18F-FDG depicted more neuroblastoma sites in 11 of 85 scans. 123I-MIBG and 18F-FDG were equivalent or complementary in 13 of 85 scans, and 17 of 85 scan results were normal. Conclusion: 18F-FDG is superior in depicting stage 1 and 2 neuroblastoma, although 123I-MIBG may be needed to exclude higher-stage disease. 18F-FDG also provides important information for patients with tumors that weakly accumulate 123I-MIBG and at major decision points during therapy (i.e., before stem cell transplantation or before surgery). 18F-FDG can also better delineate disease extent in the chest, abdomen, and pelvis. 123I-MIBG is overall superior in the evaluation of stage 4 neuroblastoma, especially during initial chemotherapy, primarily because of the better detection of bone or marrow metastases.
Functional imaging plays an important role in the assessment of neuroblastoma, from the initial diagnosis and staging to the evaluation of treatment response and detection of recurrent disease. Scan findings not only aid in initial staging but also often guide therapeutic decisions at points during treatment. In recent years, 123I-metaiodobenzylguanidine (123I-MIBG) and 99mTc-methylene diphosphonate have been the radiopharmaceuticals used for neuroblastoma assessment. The use of 18F-FDG PET is increasing, although its role remains less clear. Questions remain regarding when and in which patients 18F-FDG PET is most useful.
Two prior studies have compared MIBG scintigraphy and 18F-FDG PET in neuroblastoma. In both studies, MIBG was labeled with either 131I or 123I. Shulkin et al. (1) reviewed 20 paired 18F-FDG PET and MIBG scans in 17 patients with neuroblastoma. These authors demonstrated that most neuroblastomas concentrate 18F-FDG. However, they found that 18F-FDG is inferior to MIBG in the evaluation of neuroblastoma because of its lower tumor–to–nontumor uptake ratio (especially after therapy) and because of 18F-FDG uptake in nontumor sites (such as bone marrow, thymus, and bowel), causing potential false-positive or false-negative results. They found 18F-FDG most beneficial in tumors that failed to accumulate or weakly accumulated MIBG (1).
Kushner et al. (2) reviewed ninty-two 18F-FDG PET scans obtained from 51 patients with neuroblastoma. 18F-FDG PET was performed in conjunction with staging evaluations including MIBG scans, bone scans, CT (or MRI) scans, urine catecholamine, and bone marrow examinations. They found that 18F-FDG PET and bone marrow sampling are sufficient to monitor for progressive disease in patients whose primary tumor has been resected and in whom cranial vault lesions are absent or resolved (2).
The purpose of our study was to compare the diagnostic utility of 123I-MIBG scintigraphy and 18F-FDG PET in patients with neuroblastoma.
MATERIALS AND METHODS
Patients
A retrospective review was performed after approval by the St. Jude Children's Research Hospital (SJCRH) and Cincinnati Children's Hospital Medical Center (CCHMC) institutional review boards. A total of 113 paired 123I-MIBG and 18F-FDG PET scans were acquired for 60 patients (23 girls and 37 boys; median age at diagnosis, 3.1 years) with pathologically proven neuroblastoma. Scans were obtained between January 2003 and October 2007. Paired scans at SJCRH were acquired for research purposes after informed consent was obtained; paired scans at CCHMC were obtained when requested by the oncology service for clinical reasons. Paired scans were obtained within 14 days of each other for inclusion in the study.
Although semiquantitative scoring systems for neuroblastoma have been described with the body divided into 7 or 9 sections to evaluate disease extent (3), a simplified version of disease quantification was used in our study. The effectiveness of 123I-MIBG and 18F-FDG PET in demonstrating neural crest tumor was assessed by review of the uptake patterns for each radiopharmaceutical in the following locations: primary and residual tumor, local and regional soft-tissue (local/regional) metastases, and bone and bone marrow (bone/marrow) metastases. The paired 123I-MIBG and 18F-FDG PET scans for each patient were reviewed with direct comparison between paired studies to determine the differences in the number and distribution of disease sites in these 3 locations.
Acquisition Protocol
A total of 86 paired scans were reviewed at SJCRH, and 27 paired scans were reviewed at CCHMC. 18F-FDG scans were acquired using administered activities of 5.18 or 5.55 MBq/kg (0.14 or 0.15 mCi/kg), depending on the institution, with a maximum dosage of 444 MBq (12 mCi). A total of eighty-five 18F-FDG scans at SJCRH were obtained on an LS Discovery PET/CT scanner (GE Healthcare); 1 scan included in the SJCRH cohort was a PET-only study performed at an outside institution. Twelve 18F-FDG scans at CCHMC were PET-only studies performed on Siemens Exact or Accel PET scanners, and fifteen 18F-FDG scans at CCHMC were performed on a DSTe PET/CT scanner (GE Healthcare). Most of the 18F-FDG scans reviewed were PET/CT studies; the 13 PET-only studies were directly compared with diagnostic CT scans when available.
All MIBG scans were acquired using 123I-MIBG with administered activities of either 5.18 MBq/kg (0.14 mCi/kg) or 370 MBq/1.7 m2 body surface area (10 mCi/1.7 m2 body surface area), depending on the institution, with a maximum dose of 370 MBq (10 mCi). A total of one hundred ten 123I-MIBG scans included 24-h whole-body and SPECT images. One 123I-MIBG scan obtained at CCHMC did not include SPECT images because of sedation issues. Two 123I-MIBG scans included in the SJCRH cohort were outside studies and did not include SPECT images.
RESULTS
Patient results are summarized by disease stage, as determined by the International Neuroblastoma Staging System, in Table 1. Results for the small subset of PET-only studies are summarized in Table 2.
Summary of Results
Summary of PET-Only Studies
Stage 1 and 2 Disease (13 Paired Scans in 10 Patients)
18F-FDG depicted more primary tumor or local or regional metastases in 9 of 13 scans (69%; 95% confidence interval [CI], 44–94) in 6 patients. Four scans in 4 patients were obtained at diagnosis, and 5 scans in 3 patients were obtained during follow-up evaluations for recurrent disease, including four 123I-MIBG scans with negative results in 3 patients with 18F-FDG–positive neuroblastoma. 18F-FDG and 123I-MIBG were equivalent in 1 of 13 scans (8%; 95% CI, 0–22) in 1 patient imaged at diagnosis. Findings were negative in three of thirteen 18F-FDG and 123I-MIBG scans (23%; 95% CI, 0–46) in 3 patients imaged after tumor resection. Paired negative scans were accompanied by normal urine catecholamines and negative bone marrow examinations, supporting that the studies were true-negatives indicating absence of disease.
Stage 3 Disease (15 Paired Scans in 10 Patients)
123I-MIBG depicted more extensive primary tumor or local or regional metastases in 5 of 15 scans (33%; 95% CI, 9–57) in 4 patients. All of these scans were obtained during the first year of therapy. This included three 18F-FDG scans with negative results in 3 patients with 123I-MIBG–positive neuroblastoma imaged during initial chemotherapy or before stem cell transplantation. 18F-FDG depicted more extensive primary tumor or local or regional metastases in 4 of 15 scans (27%; 95% CI, 4–49) in 4 patients. One of these scans was acquired at diagnosis, and the remainder was obtained during follow-up after more than 12 months of therapy. This included two 123I-MIBG scans with negative findings in 2 patients with 18F-FDG–positive neuroblastoma imaged during follow-up. 123I-MIBG and 18F-FDG were equivalent in 2 of 15 scans (13%; 95% CI, 0–31) in 2 patients imaged before therapy. 123I-MIBG and 18F-FDG scan findings were negative in 4 of 15 scans (27%; 95% CI, 4–50) in 3 patients. All 3 patients with paired negative scans had negative bone marrow examinations, and 2 patients had normal urine catecholamines; 1 patient had minimally elevated urine catecholamines (homovanillic acid 10.1 mg/g creatinine, normal < 10), suggesting subclinical disease below the magnitude that could be detected by functional imaging studies.
Stage 4 Disease (85 Paired Scans in 40 Patients)
123I-MIBG depicted more neuroblastoma sites in 44 of 85 scans (52%; 95% CI, 41–62) in 24 patients. 18F-FDG depicted more neuroblastoma sites in 11 of 85 scans (13%; 95% CI, 6–20) in 8 patients. 123I-MIBG and 18F-FDG were equivalent or complementary in 13 of 85 scans (15%; 95% CI, 8–23) in 11 patients, and 123I-MIBG and 18F-FDG scan findings were negative in 17 of 85 scans (20%; 95% CI, 12–29) in 14 patients.
In stage 4 disease at diagnosis, there were 16 paired scans (16 patients). 123I-MIBG depicted more bone or marrow metastases in 8 scans (8 patients). 18F-FDG depicted more extensive primary tumor, local or regional metastases, or bone or marrow metastases in 3 scans (3 patients). 123I-MIBG and 18F-FDG were equivalent in 3 scans (3 patients). Complementary findings were seen in 2 scans (2 patients), with 18F-FDG depicting more primary tumor or local or regional metastases and 123I-MIBG depicting more bone or marrow metastases.
In stage 4 disease during the initial 12 months of therapy, there were 35 paired scans (20 patients). 123I-MIBG depicted more neuroblastoma sites in 19 scans (12 patients), primarily because of the better depiction of bone or marrow metastases but also because of the detection of some residual primary masses or local or regional metastases. This included three 18F-FDG scans with negative findings in 3 patients with 123I-MIBG–positive neuroblastoma. 18F-FDG depicted more residual primary masses, local or regional metastases, or bone or marrow metastases in 5 scans (3 patients). This included three 123I-MIBG scans with negative results in 3 patients with 18F-FDG–positive neuroblastoma imaged before stem cell transplantation. 123I-MIBG and 18F-FDG were equivalent in 4 scans (4 patients). Complementary findings were seen in 1 scan, with 18F-FDG depicting more primary tumor or local or regional metastases and 123I-MIBG depicting more bone or marrow metastases. 123I-MIBG and 18F-FDG findings were negative in 6 scans (5 patients). All patients with paired negative scans had negative bone marrow examinations, and 3 patients had normal urine catecholamines; 2 patients had elevated urine catecholamines, indicating subclinical disease below the magnitude that could be detected by functional imaging studies.
In stage 4 disease follow-up more than 12 months after the beginning of therapy, there were 34 scans (20 patients). 123I-MIBG depicted more neuroblastoma sites in 17 scans (10 patients), primarily because of depiction of bone or marrow metastases but also because of the depiction of some local or regional metastases, including five 18F-FDG scans with negative findings in 3 patients with 123I-MIBG–positive neuroblastoma. 18F-FDG depicted more metastatic disease in 3 scans (3 patients). 123I-MIBG and 18F-FDG were equivalent in 3 scans (3 patients). 123I-MIBG and 18F-FDG were negative in 11 scans (10 patients). Only 5 patients with paired negative scans had bone marrow examinations at the time of functional imaging; all were negative. Only 8 patients with paired negative scans had urine catecholamines tested at the time of functional imaging; 1 patient had elevated urine catecholamines, indicating subclinical disease below the magnitude that could be detected by functional imaging studies.
In stage 4 patients at all times, 123I-MIBG depicted more sites of bone or marrow involvement in 36 scans (27 patients). Of these, only 8 scans (6 patients) were primarily because of the superior depiction of cranial sites with 123I-MIBG.
DISCUSSION
MIBG, with a sensitivity of about 90% and specificity of nearly 100%, is the radiopharmaceutical conventionally used for imaging neuroblastoma. MIBG was originally used for the localization of pheochromocytoma (4), with its use in neuroblastoma evolving shortly thereafter (5,6). MIBG takes advantage of the adrenergic origin of neuroblastoma, using the type 1 catecholamine uptake mechanism for transport into tumor cells.
MIBG was first labeled with 131I (7) and later with 123I (8). Availability of 123I-MIBG in the United States was previously limited, with compounding at a few academic centers for local use only. 123I-MIBG is now widely available in the United States, and the Food and Drug Administration has recently approved this agent for use in neuroblastoma and pheochromocytoma. 123I-MIBG gives higher-quality images, with 131I-MIBG generally held to be suboptimal in comparison (9). The evolution of SPECT has also aided the 123I-MIBG diagnosis of neuroblastoma, improving anatomic localization (10–12). Continued improvements are expected with the advent of SPECT/CT (13,14).
The role of 18F-FDG PET in neuroblastoma and other pediatric malignancies continues to evolve with increasing use. 18F-FDG is a positron-emitting glucose analog concentrated within cells using the glucose transporter. Because most tumor cells preferentially use glucose for energy, 18F-FDG uptake is seen within most tumors. Shulkin et al. demonstrated that most neuroblastomas will concentrate 18F-FDG, although 18F-FDG uptake in nontumor sites (such as bone marrow, thymus, and bowel) can cause potential false-positive or false-negative results (1).
Other positron-emitting tracers have been studied for neuroblastoma imaging with potential advantages over 123I-MIBG including improved resolution of PET, compared with SPECT; ability to accurately quantify uptake; and potential for imaging within minutes of injection. 11C-hydroxyephedrine and 11C-epinephrine have been studied in neuroblastoma (15–18). However, the short half-life of 11C requires on-site cyclotron synthesis and limits the practical use of these radiopharmaceuticals. Compounds labeled with 18F, such as fluoronorepinephrine, fluorometaraminol, fluorodopamine, and 4-18F-fluoro-3-iodobenzylguanidine, have the potential for imaging neuroendocrine tumors (19–25). PET using 124I-MIBG has also been described (26).
In our series, we reviewed a large number of patients and studies. There was consistent use of 123I-MIBG and SPECT. There was also extensive use of PET/CT (as opposed to PET only). 18F-FDG PET and 123I-MIBG planar/SPECT techniques were, therefore, largely optimized by current standards. We also sought to review a wide range of patients with neuroblastoma, including patients with different stages of neuroblastoma at many points of therapy. This is in comparison to the study of Kushner et al. (2), which primarily addressed appropriate follow-up for patients with progressive disease after primary tumor resection in the absence of cranial vault lesions.
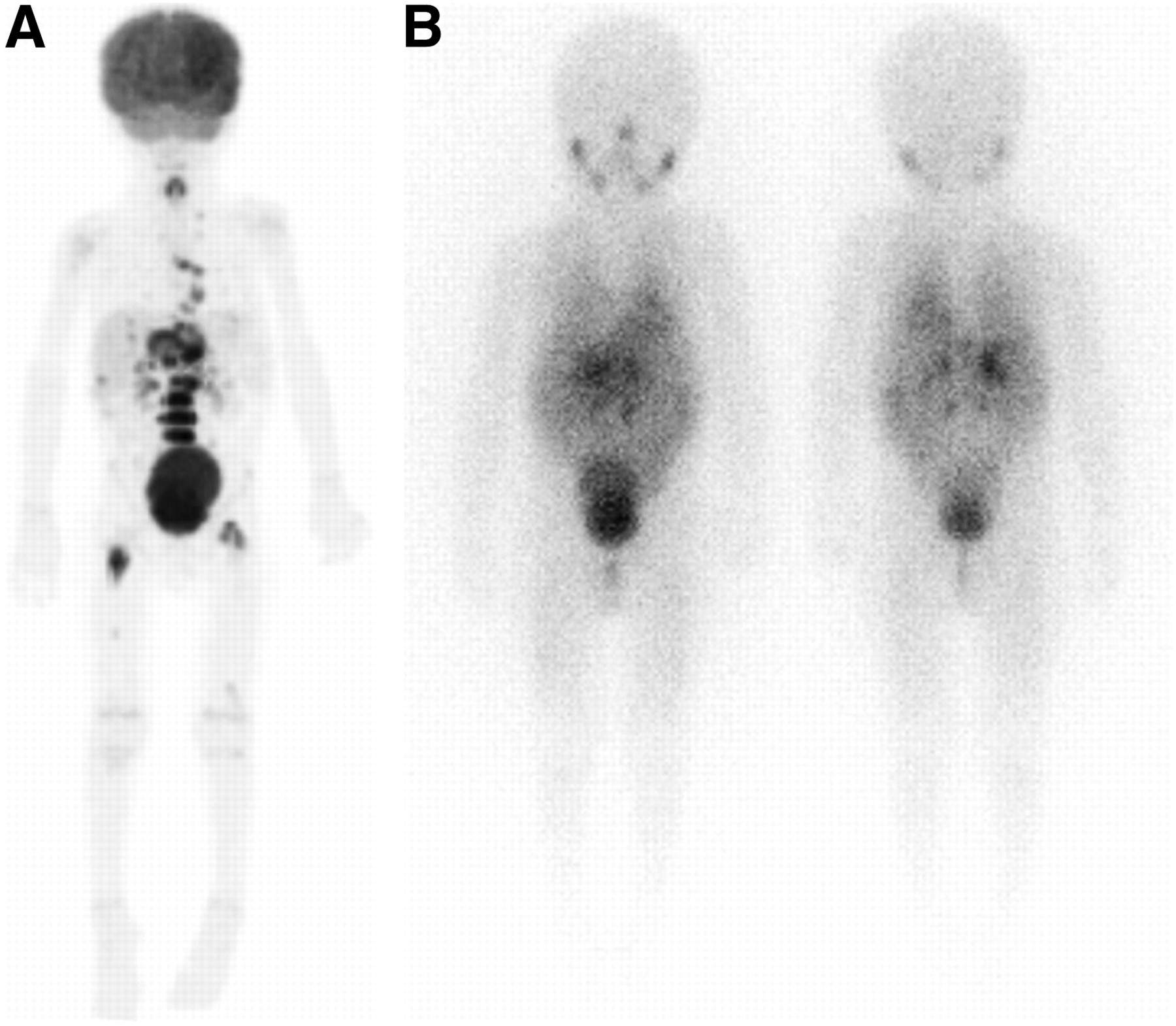
We found that 18F-FDG PET better depicted disease sites in stage 1 and 2 neuroblastoma. This was primarily because of more intense 18F-FDG uptake relative to background and better depiction of disease extent (Fig. 1). 18F-FDG also better depicted disease sites in stage 3 and 4 patients when tumors weakly accumulated 123I-MIBG (Fig. 2). In addition, 18F-FDG was useful for delineating disease extent in the chest, abdomen, and pelvis and should be used when disease involvement on CT or MRI appears more extensive than demonstrated with 123I-MIBG. Case reports of 123I-MIBG–negative recurrent neuroblastoma well demonstrated with 18F-FDG PET have recently been published, emphasizing the importance of 18F-FDG PET when 123I-MIBG reveals less disease than suggested by clinical symptoms or conventional imaging modalities (27,28).
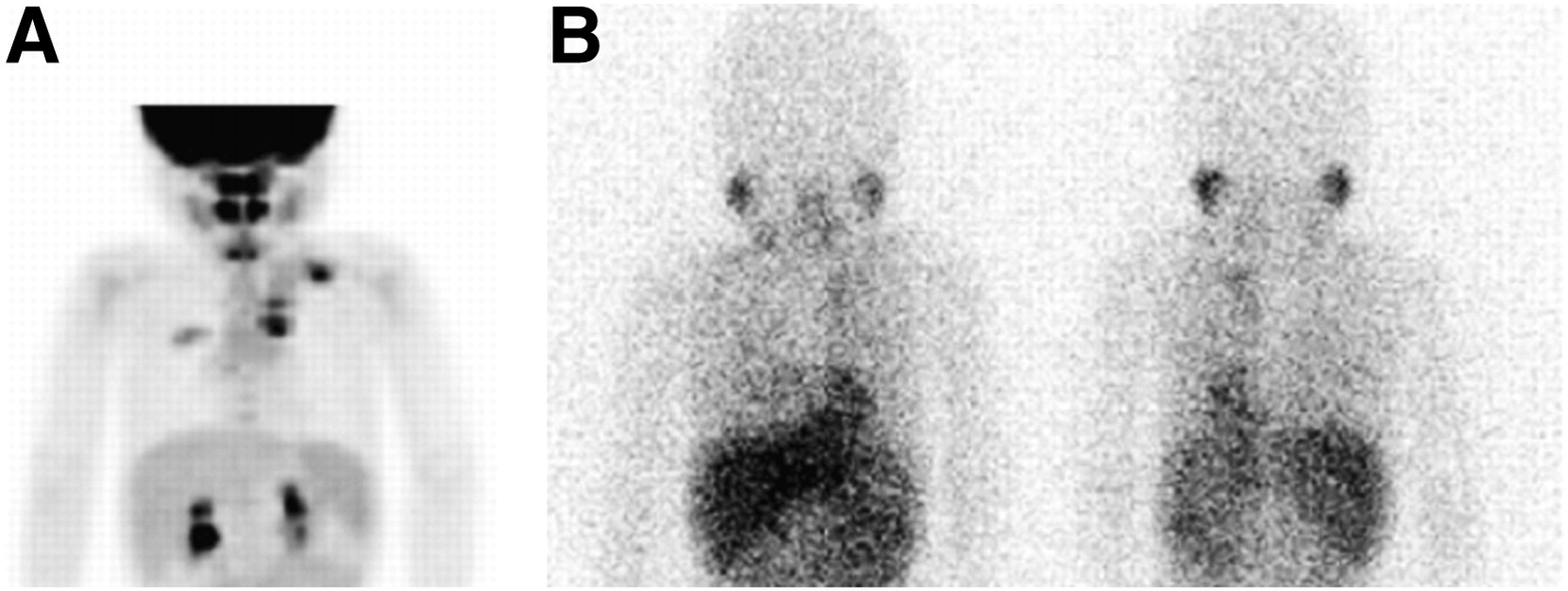
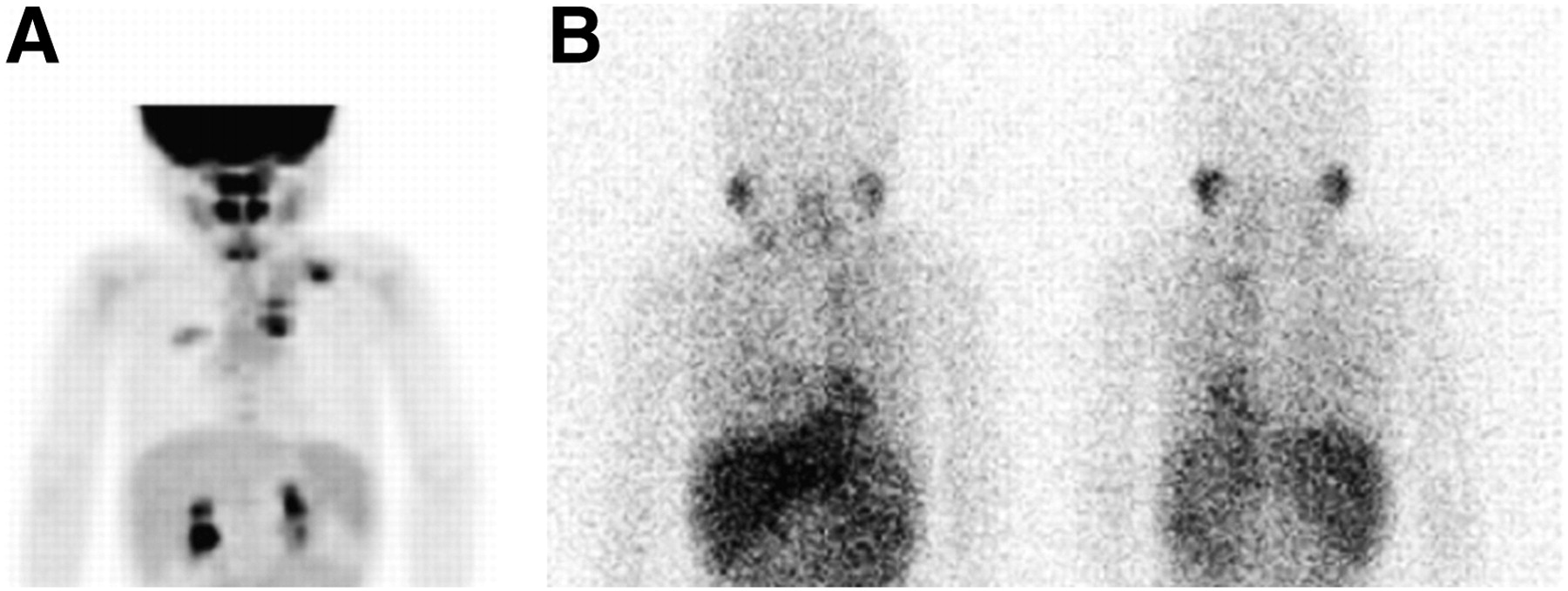
A 3-year-old boy with stage 2 neuroblastoma at diagnosis. (A) 18F-FDG anterior maximum-intensity-projection image demonstrates marked uptake in left thoracic paraspinal tumor and left supraclavicular metastatic lymph nodes. Uptake is also seen within dependent right upper lobe, corresponding to inflammatory airspace disease. (B) 123I-MIBG anterior and posterior planar images demonstrate minimal uptake in left thoracic paraspinal tumor.

A 3-month-old boy with stage 3 neuroblastoma at diagnosis. (A) 18F-FDG anterior maximum-intensity-projection image demonstrates marked uptake in the abdominal mass and mild diffuse physiologic uptake in the bone marrow. (B) 123I-MIBG anterior planar image demonstrates minimal uptake in abdominal mass, slightly above background.
18F-FDG also gave important information before stem cell transplantation, depicting residual disease not seen with 123I-MIBG in some patients (Fig. 3). Thus, 123I-MIBG and 18F-FDG scans may both be needed at major decision points during therapy to exclude residual disease that would alter management. However, routine use of paired 123I-MIBG and 18F-FDG scans in patients is impractical given scheduling and financial considerations. The cumulative radiation dose of paired studies should also be considered, particularly in low-stage-disease patients who may be treated by surgery without radiotherapy or chemotherapy, given concerns about long-term radiation effects in pediatric patients (29,30).
A 3-year-old boy with stage 4 neuroblastoma before bone marrow transplantation. (A) 18F-FDG anterior maximum-intensity-projection image demonstrates marked uptake in retroperitoneal and mediastinal disease. Uptake is also seen in bony disease, most marked in lumbar spine and proximal femurs. (B) 123I-MIBG anterior and posterior planar images demonstrate retroperitoneal uptake.
We found 123I-MIBG to be overall superior in the evaluation of stage 4 neuroblastoma, primarily because of the better detection of bone or marrow metastases. This was especially true during initial chemotherapy. Detection of bone or marrow metastases with 18F-FDG was frequently difficult, with uptake patterns that could be considered either normal or physiologic (Fig. 4). 18F-FDG scans obtained after granulocyte colony-stimulating factor therapy are especially problematic because of the associated marked increase in bone marrow uptake, which can mask or mimic metastatic disease (Fig. 5) (31). This potential problem can often be avoided by scheduling 18F-FDG imaging just before the next scheduled course of chemotherapy. Unfortunately, the PET literature does not yet indicate how much time should ideally separate the last dose of granulocyte colony-stimulating factor and attempted 18F-FDG imaging. Experimental work in animals shows that 18F-FDG uptake in bone marrow increases with increasing doses and repeated administration of cell-stimulating factors (32,33).
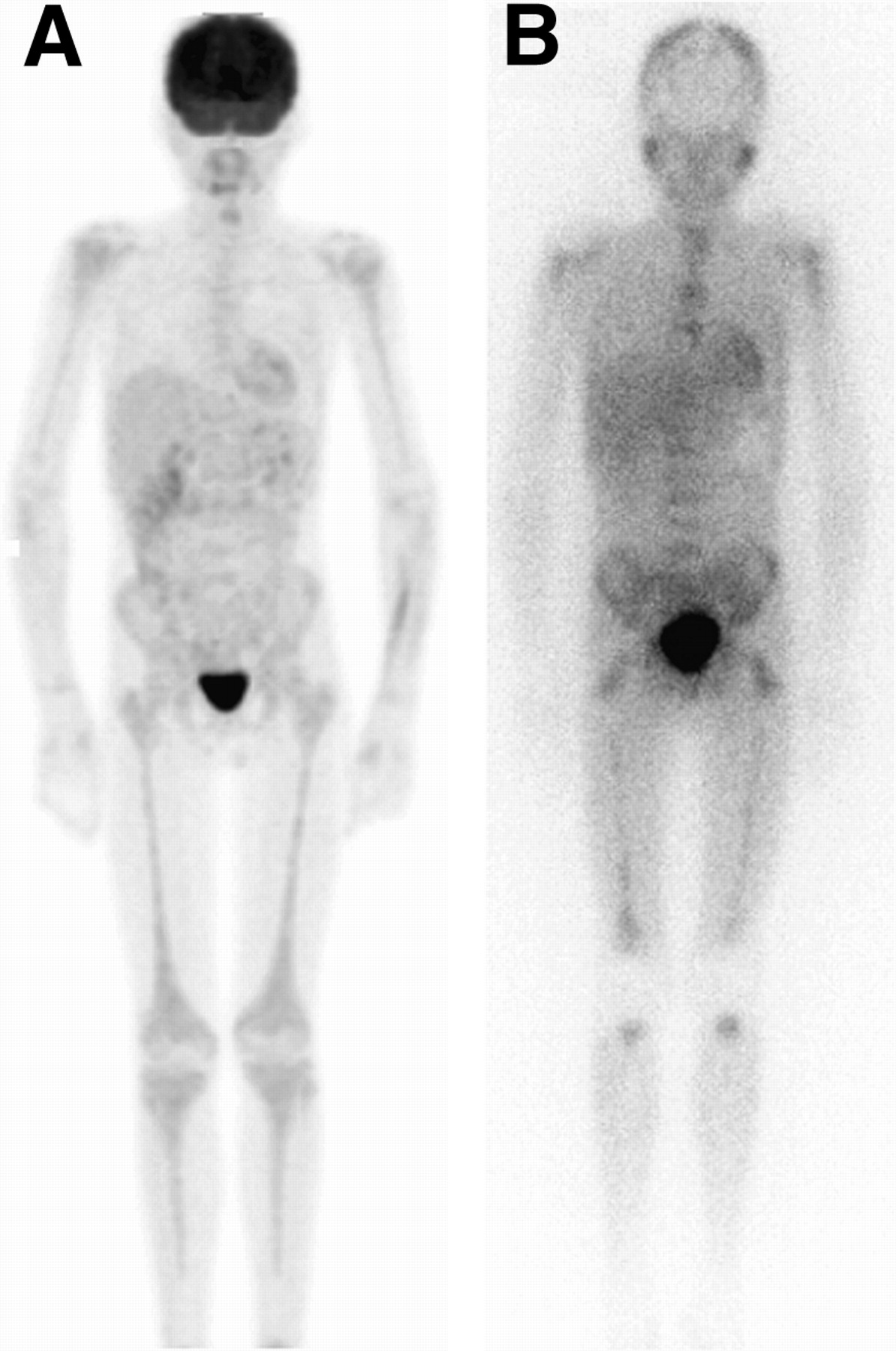
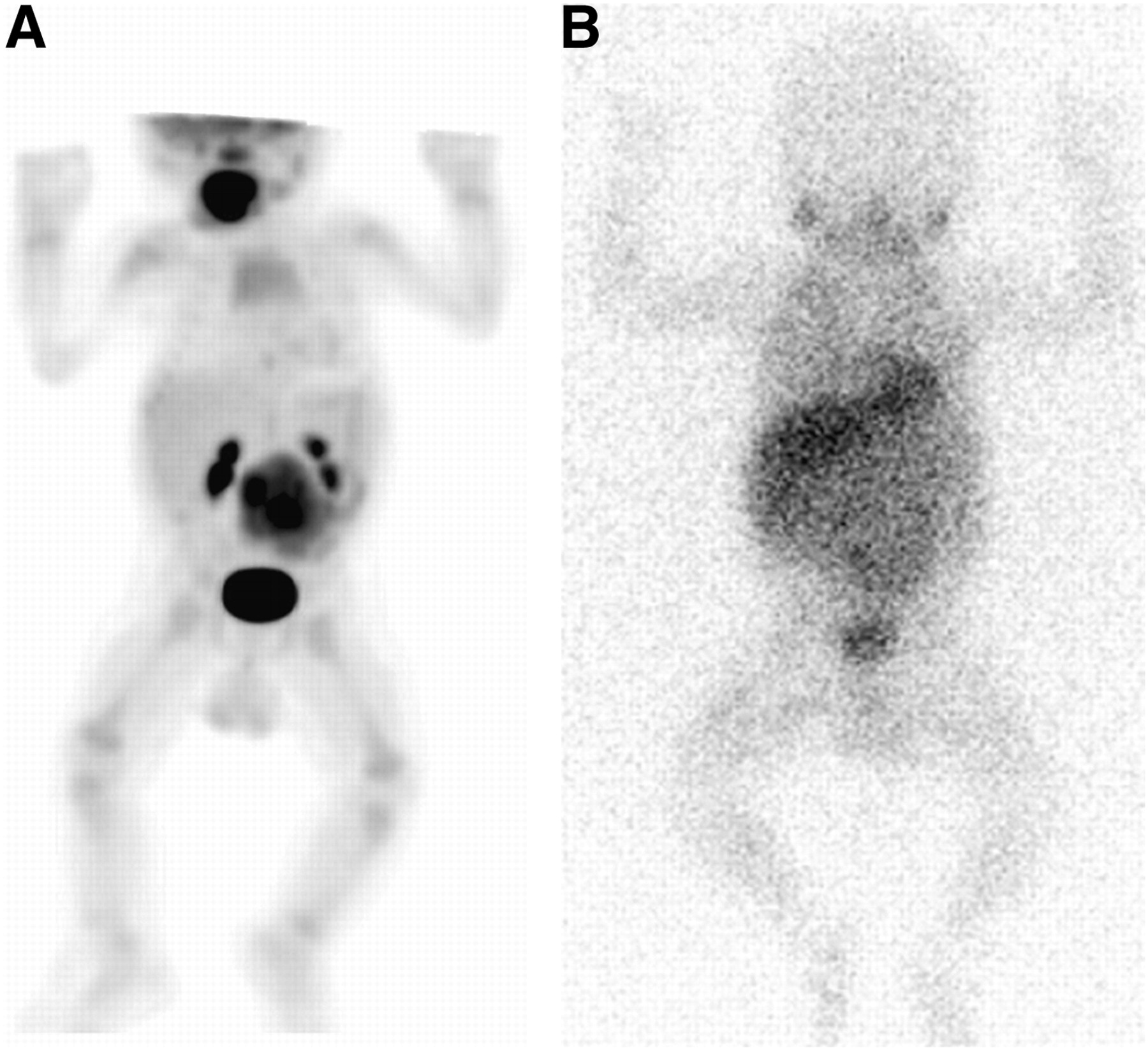
A 13-year-old boy with stage 4 neuroblastoma after initial chemotherapy. (A) 18F-FDG anterior maximum-intensity-projection image demonstrates mild diffuse bone marrow uptake extending throughout axial and appendicular skeleton in response to marrow expansion with some G-CSF stimulation. (B) 123I-MIBG anterior planar image demonstrates uptake in diffuse bone or marrow metastases. Note absence of 123I-MIBG uptake in mid- or distal humerus and mid- or distal tibia. G-CSF = granulocyte colony-stimulating factor.

A 6-year-old girl with stage 4 neuroblastoma. (A) 18F-FDG anterior maximum-intensity-projection image obtained at diagnosis demonstrates uptake in primary left retroperitoneal tumor (arrows) and multiple discrete bone or marrow metastases. 123I-MIBG imaging at diagnosis (not shown) demonstrated uptake in primary tumor and multiple bone or marrow metastases. (B) 18F-FDG anterior maximum-intensity-projection image obtained after chemotherapy and G-CSF therapy demonstrates intense diffuse bone marrow uptake, obscuring or mimicking metastatic disease. 123I-MIBG images at follow-up (not shown) demonstrated resolution of uptake in primary tumor and bone or marrow metastases. Bone marrow sampling at time of follow-up scan showed no evidence of metastatic tumor. G-CSF = granulocyte colony-stimulating factor.
CONCLUSION
18F-FDG is superior in depicting stage 1 and 2 neuroblastoma, although 123I-MIBG may be needed to exclude higher-stage disease. 18F-FDG also provides important information in patients with tumors that weakly accumulate 123I-MIBG and at major decision points during therapy (i.e., before stem cell transplantation or before surgery). 18F-FDG can also better delineate disease extent in the chest, abdomen, and pelvis and should always be considered when 123I-MIBG reveals less disease than suggested by clinical symptoms or conventional imaging modalities. 123I-MIBG is overall superior in the evaluation of stage 4 neuroblastoma, especially during initial chemotherapy. This is primarily because of the better detection of bone or marrow metastases.
Any generalized statements regarding the use of 123I-MIBG scintigraphy and 18F-FDG PET in neuroblastoma will have frequent exceptions that could significantly affect clinical management of individual patients. Larger multiinstitutional, prospective trials may be necessary to provide further information.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication November 24, 2008.
- Accepted for publication April 6, 2009.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- SNMMI Procedure Standard/EANM Practice Guideline on Pediatric 18F-FDG PET/CT for Oncology 1.0
- Is True Whole-Body 18F-FDG PET/CT Required in Pediatric Lymphoma? An IAEA Multicenter Prospective Study
- Radiolabeled (4-Fluoro-3-Iodobenzyl)Guanidine Improves Imaging and Targeted Radionuclide Therapy of Norepinephrine Transporter-Expressing Tumors
- Value of 18F-FDG PET and PET/CT for Evaluation of Pediatric Malignancies
- Potential Pediatric Applications of PET/MR
- Imaging the Norepinephrine Transporter in Neuroblastoma: A Comparison of [18F]-MFBG and 123I-MIBG
- Characterization of Neuroblastic Tumors Using 18F-FDOPA PET
- 64Cu-p-NH2-Bn-DOTA-hu14.18K322A, a PET Radiotracer Targeting Neuroblastoma and Melanoma
- Nuclear Medicine in the First Year of Life
- 18F-FDG PET/CT and 123I-Metaiodobenzylguanidine Imaging in High-Risk Neuroblastoma: Diagnostic Comparison and Survival Analysis
- Clinical presentations and imaging findings of neuroblastoma beyond abdominal mass and a review of imaging algorithm
- PET Imaging of Norepinephrine Transporter-Expressing Tumors Using 76Br-meta-Bromobenzylguanidine
- 123I-MIBG Scintigraphy and 18F-FDG PET in Neuroblastoma
- 123I-MIBG Versus 18F-FDG: Which Is Better, or Which Can Be Eliminated?
- Reply: 123I-MIBG Scintigraphy and 18F-FDG PET in Neuroblastoma