


Abstract
The evaluation of stem cell–mediated cardiomyoplasty by noninvasive in vivo imaging is critical for its clinical application. We hypothesized that dual-tracer small-animal SPECT would allow simultaneous imaging of 99mTc-sestamibi to assess myocardial perfusion and of 111In-labeled stem cells to delineate stem cell engraftment. Methods: Three to 4 million rat embryonic cardiomyoblasts (H9c2 cells) were labeled with 11.1–14.8 MBq (0.3–0.4 mCi) of 111In-oxyquinoline and then injected into the border zones of infarcted myocardium of rats. 111In images were acquired with a SPECT scanner 2, 24, 48, 72, and 96 h after the stem cells were injected into the infarcted myocardium. To visualize the perfusion deficit in the infarcted myocardium, we injected 74 MBq (2 mCi) of 99mTc-sestamibi (Cardiolite) intravenously 48 h after grafting. Dual-isotope pinhole SPECT was used to image 99mTc-sestamibi uptake simultaneously with 111In to delineate retention of 111In-labeled stem cells. The presence of labeled stem cells was confirmed by autoradiography and histology. Results: SPECT of 99mTc-sestamibi was used to delineate perfusion deficits and infarcted myocardium. Bull’s-eye plots indicated that the 111In signal from the labeled stem cells overlapped the perfusion deficits identified from the 99mTc-sestamibi images. The 111In signal associated with the radiolabeled stem cells could be detected with SPECT of the heart for 96 h after engraftment. Conclusion: This study demonstrated the feasibility of using dual-isotope pinhole SPECT for high-resolution detection of perfusion deficits with 99mTc-sestamibi and with 111In-labeled stem cells grafted into the region of the infarct.
Coronary heart disease is the leading cause of death in the United States. Postinfarction survival has improved in recent years because of the optimal therapies afforded by modern medicine. However, none of the therapies is able to reverse the destructive cascade that occurs after acute myocardial infarction: loss of cardiomyocytes, development of myocardial fibrosis, subsequent left ventricular (LV) remodeling, progressive LV dilatation, and heart failure. In fact, according to studies by the American Heart Association, in up to 50% of patients who experience a moderate or larger infarction, progressive LV dysfunction may develop. A novel treatment strategy, often referred to as cellular cardiomyoplasty, includes local (intramyocardial or intracoronary) and systemic (intravenous) delivery of fetal or neonatal cardiomyocytes, skeletal myoblasts, or embryonic or bone marrow–derived stem cells. This strategy aims at enhancing cardiac function by repopulating the infarcted region with viable cardiomyocytes and, therefore, bears great promise for the cure of this disease (1).
Before stem cell–mediated cardiomyoplasty can be applied in the clinic, basic research must be performed using animal models to address critical issues: Do the grafted cells survive in sufficient numbers to be biologically meaningful? Can grafted cells differentiate into cardiomyocytes in response to local stimuli? Do the grafted cells contribute to the improvement of contractile function in addition to the improvement of global function? Survival of grafted cells has been evaluated by labeling cells with BrdU or fluorescent dye followed by detection of the labels in tissue samples, or by quantification of male DNA in the donor cells using real-time polymerase chain reaction technique (2–4). However, the invasive nature of the technique allows only a single time-point study for each animal; thus, information on the natural history of cell survival or proliferation in an individual animal is lost. The approach of using a reporter or marker gene holds promise for noninvasive quantification of cell survival. The survival fraction of grafted cells can be evaluated over time by stably transfecting cells with a reporter gene (e.g., HSV1-tk), and quantification of reporter gene expression by PET or SPECT would allow evaluation of survival fraction of grafted cells over time. The original work of developing HSV1-tk as a reporter gene was pioneered by Gambhir et al. (5, 6) and Tjuvajev et al. (7). PET of rat cardiomyoblasts (H9c2 cells) that were grafted into rat myocardium after being transfected by HSV1-tk has been reported recently (8). When the cells are transfected with another reporter gene, firefly luciferase (Fluc), bioluminescent imaging can be used for detection of these cells (9, 10). Differentiation of stem cells can also be monitored noninvasively by imaging a tissue-specific reporter gene, such as Fluc, under the transcriptional control of the mouse ventricular myosin light chain 2 (MLC2v) gene, whose expression is primarily limited to cardiac ventricular myocardium in adult mice (11). Such a cardiac-specific reporter gene (MLC2v-Fluc) was used previously to study regulation of embryonic heart development in postmortem samples (12–14). In vivo detection of MLC2v-Fluc reporter gene expression by bioluminescent imaging has been achieved in mice recently (15).
Although optical (e.g., bioluminescence) and nuclear medicine (PET and SPECT) imaging modalities are sensitive for imaging gene expression, global cardiac function (e.g., ejection fraction and cardiac output) is routinely measured by MRI in the clinic because of the superior spatial resolution and tomographic acquisition method provided by MRI. Cardiac MRI of small animals (especially mice) at a high magnetic field strength (4–11 T) has greatly advanced in recent years (16–19), largely because of the wide application of transgenic models. MRI has yielded accurate and reliable quantification of murine global myocardium function (e.g., ejection fraction and cardiac output), LV mass, and right ventricular size (17, 20, 21). Cardiac wall motion and strain can be obtained by tagged MRI (18, 22), a unique, noninvasive technique for evaluation of regional contractile function (23, 24). In summary, noninvasive imaging techniques hold the key to addressing critical issues associated with stem cell therapy. Therefore, it is necessary to establish multimodality imaging as a means of investigating these complicated issues efficiently and accurately.
In this study, we attempted to use clinically applicable tracers for detection of stem cells in a rat model of myocardial ischemia (infarction) using ultra-high-resolution SPECT. We hypothesized that dual-tracer SPECT would allow simultaneous detection of perfusion deficits in the infarcted myocardium with 99mTc-sestamibi and of grafted stem cells labeled with 111In.
MATERIALS AND METHODS
Rat Model of Myocardial Infarction
Male Sprague–Dawley rats (6–8 wk old, 220–250 g) were purchased from Charles River Laboratories. The animals were anesthetized by an intraperitoneal injection of ketamine and xylazine (50 and 2.5 mg/kg, respectively) and then were intubated and ventilated through a small-animal ventilator (model 680; Harvard Apparatus). The tidal volume (1.5–2.5 mL) was determined for each animal according to its respiratory rate and body weight. One percent isoflurane mixed with oxygen was used to maintain the anesthesia during surgery. The body temperature was maintained by a heating lamp. The electrocardiogram was monitored throughout the surgery. After the thoracic cavity and pericardium had been opened, the left anterior descending coronary artery (LAD) was ligated by passing a piece of 6-0 silk suture underneath the vessel and the surrounding myocardium. A small piece of polyethylene tubing was used to ligate the artery without damaging it. Ligation was maintained for 45 min, and LAD perfusion was then restored. 111In-labeled cells were injected in 4–5 locations surrounding the infarcted (pale) region, and the thoracotomy incision was closed. All animal procedures were approved by the Institutional Animal Care and Use Committee of the University of Pennsylvania.
111In Labeling of Stem Cells
Rat embryonic cardiomyoblast H9c2 cells were obtained from American Type Culture Collection and were maintained in Dulbecco’s modified Eagle medium (DMEM) supplied with 10% fetal bovine serum. Cells were labeled with 111In-oxyquinoline (Amersham) following the procedures described by Cesano et al. (25). Briefly, 3–4 million cells were incubated with serum-free DMEM containing 11.1–14.8 MBq (0.3–0.4 mCi) of 111In-oxyquinoline for 30 min. Cells were then washed 3 times with phosphate-buffered saline and resuspended in 200 μL of serum-free DMEM. Labeling efficiency was estimated by dividing the radioactivity of the cell suspension during incubation (total added activity) by the radioactivity of the cell suspension after washing (final activity) and multiplying by 100. These procedures resulted in labeling efficiency of around 85%.
SPECT Imaging
Cardiac SPECT was performed on a Prism 3000XP triple-head γ-camera (Philips Medical Systems) equipped with custom-made tungsten knife-edge pinhole collimators (Nuclear Fields) (26–28). The focal length of the collimators was 24 cm, with a radius of rotation of 5 cm and a pinhole diameter of 3 mm. The acquisition parameters included a continuous mode with 120 projection angles over a 360° arc to obtain data in a 128 × 128 matrix with a pixel size and slice thickness of 3.56 mm. The images were then reconstructed using 10 iterations of a simultaneous algebraic reconstruction technique (29). Center of rotation error was corrected by scanning a thin line source and iteratively adjusting the center-of-rotation offsets until the reconstructed image was a point, rather than an annulus. The same source was used to measure the spatial resolution of the system for both 99mTc and 111In. Images consisted of a matrix of 128 × 128 × 128 with an isotropic voxel size of 0.74 mm. Attenuation and scatter correction were not performed on the SPECT data.
Perfusion images were obtained 30 min after injection of 74 MBq (2 mCi) of 99mTc-sestamibi (Cardiolite; Bristol-Myers Squibb Medical Imaging, Inc.). The 140-keV photons from 99mTc were acquired simultaneously with the 247-keV photons from 111In using 2 separate energy windows. This allowed the 99mTc-sestamibi perfusion images to be registered spatially with the 111In images of the grafted stem cells
Cross talk between the 2 isotopes into each energy window was measured by scanning the rats with each isotope separately. After injection of 111In-labeled stem cells, the rats were scanned with both sets of energy windows, and downscatter from the 111In into the 99mTc energy windows was counted. Similarly, the rats were injected with 99mTc-sestamibi and scanned with both energy windows, to measure any overlap from the low-energy 99mTc photons into the high-energy 111In window.
111In images were acquired 2, 24, 48, 72, and 96 h after grafting of labeled stem cells. Perfusion images were obtained 48 h (2 d) after stem cell grafting.
Image Analysis
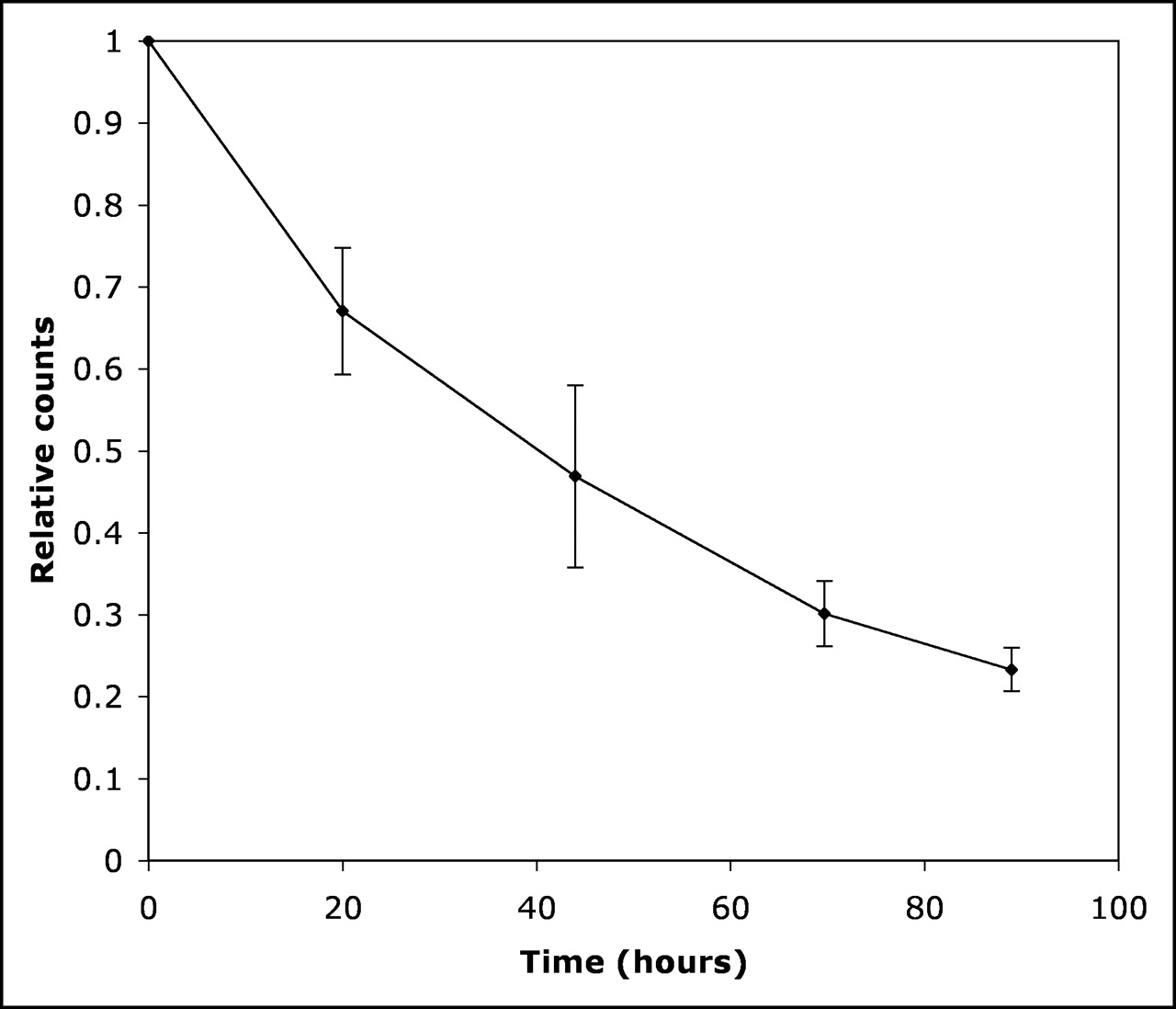
Regions of interest were placed over the most intense area of 111In uptake, and the counts were measured for each scan. After correction for radioactive decay of the isotope, the relative counts were plotted as a function of time to determine the washout rate.
The bull’s-eye plots for each study were obtained by first reorienting the data into short-axis slices. Each short-axis slice was processed to obtain circumferential profiles of the maximum intensity along each ray—also known as maximum count circumferential profile. For each slice, 80 rays were generated and the maximum along each ray was computed. These profiles were arranged as concentric rings starting from the apical region at the center and basal region at the periphery to give the bull’s-eye plot. In addition, both long- and short-axis slices were extracted to give representative images for each animal in the region of the infarct.
Autoradiography and Histology
H9c2 cells were prelabeled with superparamagnetic iron oxide (SPIO) particles. Briefly, SPIO containing ferumoxides injectable solution (Feridex; Berlex Laboratories) was mixed with culture medium (final iron concentration, 50 μg/mL), into which poly-l-lysine (molecular weight, 275 kDa; Sigma) was added (final concentration, 0.4 μg/mL). The cells were incubated with the labeling medium for about 20 h, followed by 3 washes and incubation overnight in fresh medium, before harvest for 111In labeling. Three million cells were injected into a rat with chronic infarction (1 wk after myocardium infarction surgery) and a rat with fresh infarction (immediately after surgery). Both rats were sacrificed 2 h after injection of labeled cells. The heart was perfused retrograde through the aorta with 5 mL of saline and then frozen in a bath of dry ice and acetone. After equilibrium had been reached at −20°C, 10-μm sections were cut on a cryostat microtome (Hacker Instruments) and thaw-mounted on microscope slides (3 sections per slide). Tissue sections were air-dried at room temperature and exposed to Cronex MRF-34 film for 20 h. The exposed film was developed by a Kodak automatic film processor.
Sections adjacent to the autoradiographic sections were reserved for histologic analysis. For Prussian blue staining, slides were incubated with Perls’ reagent, consisting of 2% potassium ferrocyanide (Sigma-Aldrich Co.) in 23.4% HCl, for 30 min in a dark room, followed by counterstaining with nuclear fast red (Sigma-Aldrich Co.). In addition, morphologic analysis of the slides was used to identify stem cells, which tend to be rounder and to have larger nuclei.
RESULTS
The spatial resolution of the pinhole SPECT system in the configuration used for the rat studies was measured using a thin line source for both isotopes. At the center of the field of view, the resolution for 99mTc was 3.9 mm, whereas for the higher-energy photons from 111In the resolution was degraded slightly to 4.6 mm, because of increased penetration at the pinhole edges. No energy window cross-talk was observed for either isotope—that is, no counts were recorded above background levels in the 99mTc energy window from pure 111In, and vice versa.
Long- and short-axis views of the normal rat myocardium revealed uniform uptake of 99mTc-sestamibi (Figs. 1A and 1C). However, the myocardial infarct was delineated clearly by a perfusion deficit (Figs. 1E and 1G). Bull’s-eye plots (Figs. 2) generated from the 99mTc-sestamibi images revealed uniform perfusion in normal myocardium (Fig. 2A, rat 3), whereas a region of perfusion deficit (dark blue) was detected in infarcted myocardium (Figs. 2C and 2E for rats 2 and 4, respectively). The perfusion deficit was localized primarily in the territory supplied by the LAD, that is, the anterior lateral wall (Fig. 2C), or in the apical region of the heart (Fig. 2E). This observation is consistent with the myocardial infarction model generated from LAD ligation and reperfusion. In addition, comparison of Figures 2C and 2E also reveals a smaller region of perfusion deficit in rat 2 than in rat 4. These 2 rats were reimaged with 99mTc-sestamibi SPECT 7 wk after infarction and then were euthanized. Triphenyl tetrazolium chloride (30) staining of the myocardium showed that the infarction volume was approximately 5% of the LV volume in rat 2 and 18% in rat 4. Although the infarction volume estimated at this late stage of infarction is likely to be smaller than the initial volume because of thinning of the infarcted myocardial wall, the difference in infarction size between the 2 animals was consistent with that observed from a qualitative visual inspection of the SPECT images.
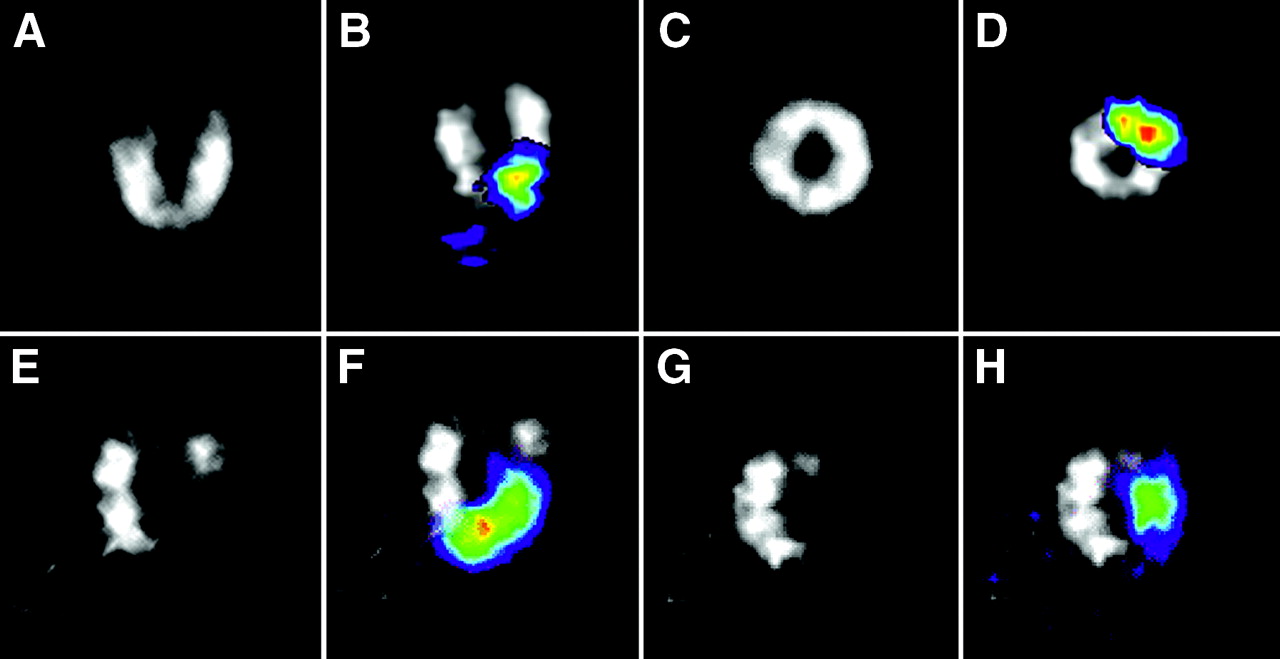
Cardiac long- and short-axis SPECT images of normal (A and C) and infarcted (E and G) heart using perfusion tracer 99mTc-sestamibi. 111In signal (color) was overlaid on gray-scale 99mTc-sestamibi images for normal (B and D) and infarcted (F and H) heart.
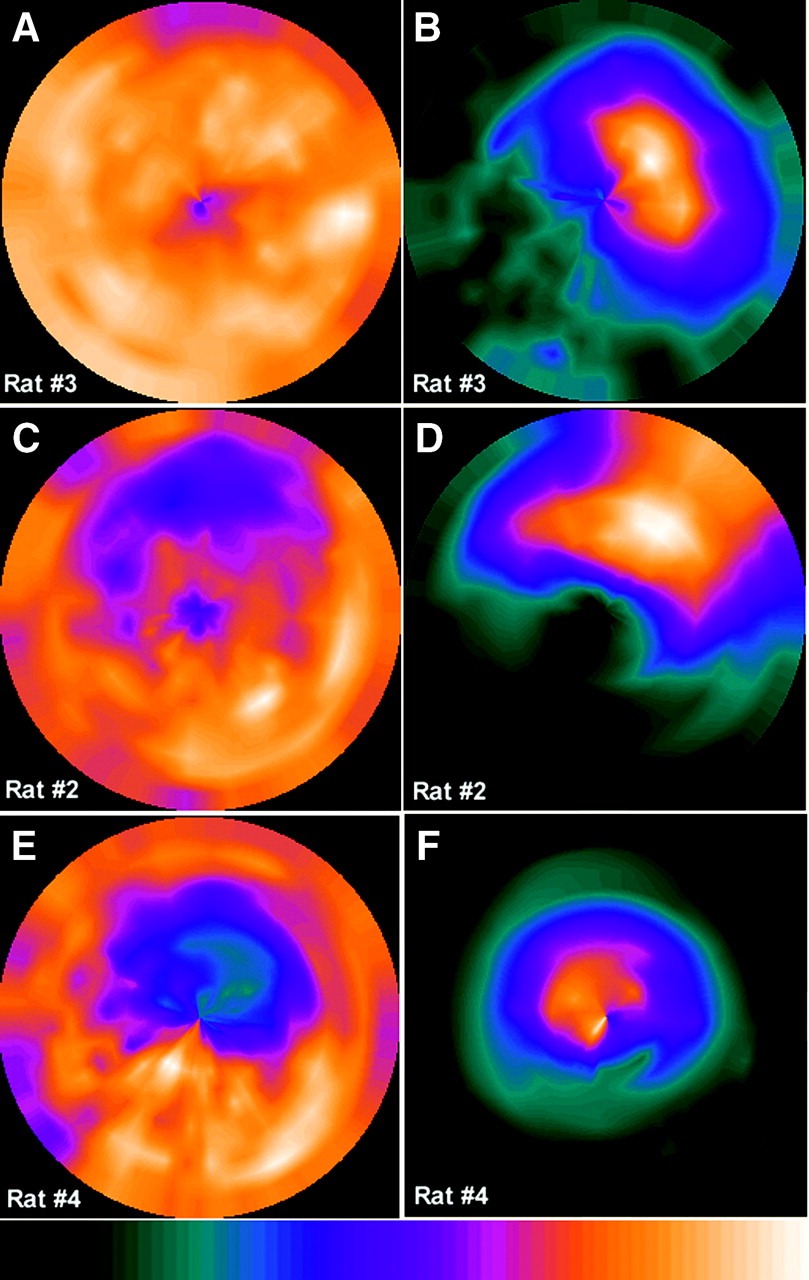
Bull’s-eye plots of 99mTc-sestamibi signal (A, C, and E) and 111In signal (B, D, and F) from normal rat (rat 3) and 2 rats with different infarction sizes (rats 2 and 4). Color bar represents transition from weak to strong signal intensity from left to right.
Simultaneous detection of the 140-keV photons generated from decay of 99mTc and of the 247-keV photons from 111In permits the perfect spatial coregistration of sestamibi and indium images. Because stem cells were injected both in normal rats and in rats with infarction, overlay of the 111In signal (color) on the 99mTc-sestamibi image (gray scale) indicated that the 111In signal coincided with the injection site in the normal rats (Figs. 1B and 1D) and also with the perfusion deficit region in the infarcted myocardium (Figs. 1F and 1H). Bull’s-eye plots from the 111In signal (Figs. 2B, 2D, and 2F) further confirmed this observation. The 111In signal from rat 2 (Fig. 2D) was greater than that from rat 4 (Fig. 2F) because more 111In activity (14.8 MBq [0.4 mCi]) was used to label the cells grafted in rat 2 than those grafted in rats 3 and 4 (11.1 MBq [0.3 mCi]).
The 111In signal from the grafted stem cells was readily detected in the heart within 2 h after injection and remained detectable 96 h after injection. For visualization of washout of background 111In signal from the lungs and thorax over time, a single transaxial slice at the level of the maximum 111In uptake is shown in Figures 3A–3E for a normal rat (rat 3) and in Figures 3F–3J for a rat with infarction (rat 4). A threshold was applied to these images to give the same maximum pixel value in each. Uptake of 111In in the thoracic region was observed in rat 3 within 2 h after grafting of stem cells but decreased to background levels 24 h after injection. Compared with rat 3, the background uptake of 111In was minimal in rat 4, possibly because of a better injection with little or no leakage of radioactivity from the myocardium. Slight bleeding occurred in some animals during the injection (e.g., when the needle hit a capillary) and resulted in leakage of the injected cells from the injection site to the chest cavity.

Time course of background 111In signal intensity in region of lungs and thorax in rats 3 (top) and 4 (bottom). Each image was normalized to give same maximum count to show relative washout of tracer from thoracic cavity. Signal detected in thoracic region in rat 3 in first image (acquired within 2 h after injection) was likely due to some leakage during injection of cells.
Figure 4 shows the time course of the 111In signal from the hearts of 6 animals (n = 6). The signal was normalized to the initial intensity of 111In, acquired within 2 h after cell grafting. The mean washout half-life was 2.55 ± 0.09 d. This curve was corrected for the radioactive decay of 111In (67.2-h half-life). Therefore, the curve reflects both clearance of the grafted stem cells from the myocardium and dissociation of the 111In label from the grafted cells.
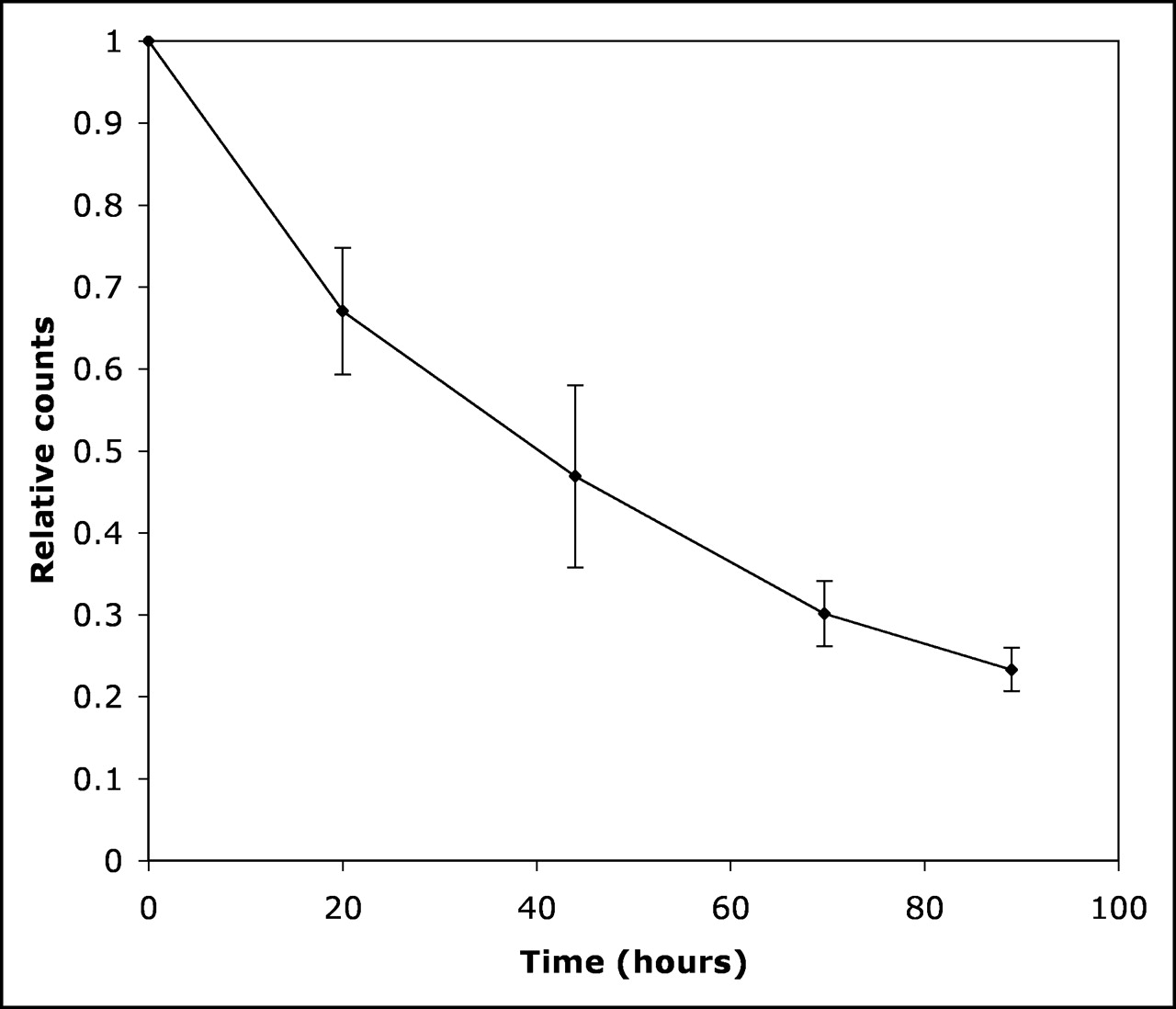
Time course of 111In signal intensity in hearts from 6 animals. Curve was corrected for radioactive decay of 111In. Error bars represent 1 SD.
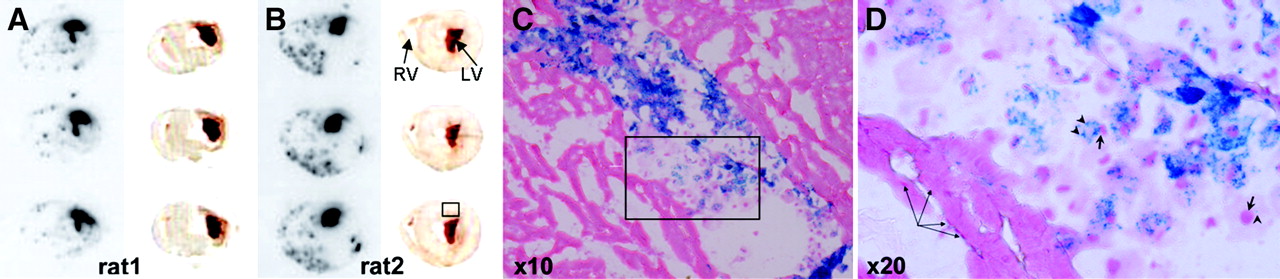
Autoradiographic images of 111In uptake from 3 adjacent slices, with the corresponding photographs, are shown for rats 1 and 2 in Figures 5A and 5B. A region of intense 111In uptake was identified on each slide. Histologic analysis (Fig. 5C) of adjacent slides confirmed SPIO-labeled cells in that region, where both intensely and lightly labeled cells were identified (Fig. 5D). The SPIO particles were stained blue and localized in the cytoplasm. The injected cells had a unique morphology—round, with large nuclei stained red—which was different from the surrounding myocardium.
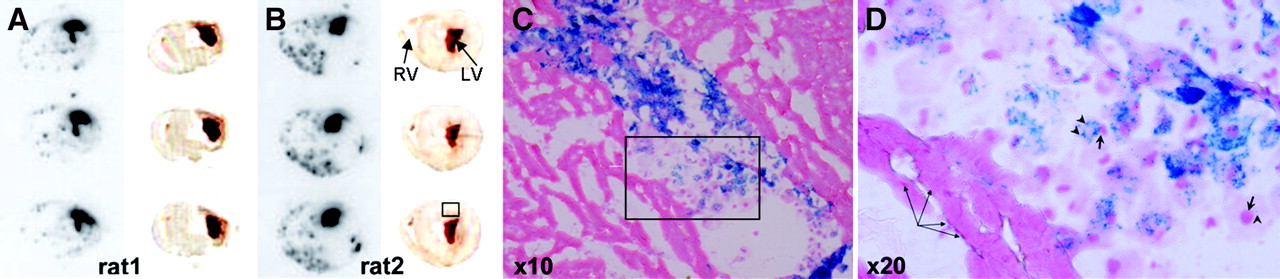
(A and B) Autoradiographs (left) of 3 adjacent slices and corresponding photographs (right). Region of intense 111In uptake (boxed area) was identified on each slice. (C and D) Histologic analysis of adjacent tissue slices reveals injected cells localized in region outlined in box. SPIO particles (arrowheads) are stained blue, whereas nuclei (short arrows) are counterstained red. Magnified view (D) of boxed area in C shows intensely SPIO-labeled cells (e.g., 1 in center) and slightly labeled cells (e.g., 1 in right corner, which contained only 1 blue dot; the cell is round, as delineated by pink-stained cytoplasm, and has a large nucleus). Unique morphology distinguishes injected cells from surrounding myocardium. Bundle of muscle fibers (long arrows) is also seen. LV = left ventricle; RV = right ventricle.
Some 111In label in the autoradiographs, where no injected cells were found by histologic analysis, may represent free 111In. This type of background was much lower in rat 1 than in rat 2, because the dose of 111In used to label the cells was 50% less. Although a significant amount of blood was retained in the LV lumen (tissue photographs in Figs. 5A and 5B), the radioactivity was primarily mapped to the myocardial wall instead of to the blood. This was true for both rat 1 and rat 2 but was particularly clear in rat 2, which had a fresh infarction where the wall thickness remained unchanged. Rat 1 had a chronic infarction (1 wk old), and the LV wall in the infarcted region was much thinner.
DISCUSSION
111In-Oxyquinoline and 99mT-hexamethylpropylene amine oxime have been used routinely in the general nuclear medicine clinic for labeling autologous white blood cells, which are then infused back to the patients for localization of inflammatory sites and infectious foci (31, 32). It is thought that the mechanism of labeling cells with 111In-oxyquinoline involves an exchange between the oxyquinoline carrier and subcellular components that chelate indium more strongly than oxyquinoline. According to the manufacturer, approximately 24% of the radioactive label dissociates from the labeled leukocytes by 24 h. We are seeking possible chemical modifications of indium oxyquinoline so that the 111In label of the cell is maintained longer than the physical decay (half-life, 67.2 h) of the radionuclide.
By incubation of 3–4 million cells with medium containing 11.1–14.8 MBq (0.3–0.4 mCi) of 111In, labeled cells were detected up to 4 d after engraftment. By 96 h, about 20% of the injected dose (after correction for radioactive decay) remained around the infarction site. Because of the dissociation of 111In from the labeled cells, the number of cells that remained in the heart (where the radioactivity was counted) would have been greater than 20% of the initially grafted cells. The rest of the cells were removed from the heart through circulation or other mechanisms. Because the 111In label may remain with the cell even after the cell has died, one cannot translate the observed radioactivity to the number of surviving cells. A marker gene approach (10, 33) would be more suitable for estimating the survival fraction of injected stem cells, although the cells have to be transduced stably before they are grafted, a manipulation that may have a long-term effect on a cell. Therefore, 111In is ideal for short-term tracking of cells and testing strategies that aim at enhancing the homing of stem cells. By being acquired simultaneously with 111In, using different energy photons from the 2 tracers, the 99mTc-sestamibi images could localize the anatomic extent of normal perfused myocardium for registration with the 111In images. The perfusion information provided by the 99mTc-sestamibi images potentially is useful for monitoring the functional recovery of infarcted myocardium in response to treatment.
The region where the injected cells (stained plus unstained) were found coincided with the hot region on the autoradiograph. Because the indium label could exit the cells, it is likely that free labels also contributed to some of the signal seen on both the in vivo SPECT images and the autoradiographs.
SPIO nanoparticles have been used to label stem cells (34, 35), whose location was identified by MRI (36) after myocardial injection. The application of micrometer-sized SPIO particles (37) also has the potential to identify a few cells, or even a single cell, in situ. The magnetic field inhomogeneity generated by these particles induces a signal loss (void), not a signal enhancement as one would expect for a nuclear medicine tracer such as 111In. Therefore, the specificity of this signal loss due to the presence of SPIO particles sometimes has to be verified. In addition, signals from surviving cells are not differentiated by this labeling technique from dead cells, or from macrophages that phagocytose the dead cells. A triple-labeling strategy might have the potential for monitoring short-term cell homing with 111In, for monitoring long-term cell survival with reporter genes, and for defining anatomy and assessing migration of the cells with SPIO particles.
CONCLUSION
We demonstrated that 111In-labeled cells were detected by ultra-high-resolution SPECT up to 96 h after they were grafted in the myocardium and that simultaneously acquired 99mTc-sestamibi images provided anatomic landmarks for localizing the 111In distribution and for visualizing the perfusion deficit in the infarcted region.
Acknowledgments
This research was supported by grants EB-002473, EB-000301, and EB-001809 from the National Institutes of Health and by grant 0425558U from the American Heart Association. We thank Dr. Jeff W. Bulte for providing the method of stem cell labeling using Feridex.
Footnotes
Received Jul. 22, 2004; revision accepted Jan. 16, 2005.
For correspondence or reprints contact: Paul D. Acton, PhD, 1 Silverstein, HUP, 3400 Spruce St., Department of Radiology, University of Pennsylvania, Philadelphia, PA 19104-4283.
E-mail: pacton{at}mail.med.upenn.edu
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Perspectives on Assessment of Stem Cell Therapy in Stroke by 18F-FDG PET
- 99mTc-Based Imaging of Transplanted Neural Stem Cells and Progenitor Cells
- Current Perspectives on Imaging Cardiac Stem Cell Therapy
- Noninvasive Quantification and Optimization of Acute Cell Retention by In Vivo Positron Emission Tomography After Intramyocardial Cardiac-Derived Stem Cell Delivery
- In Vivo SPECT Quantification of Transplanted Cell Survival After Engraftment Using 111In-Tropolone in Infarcted Canine Myocardium
- Small-Animal SPECT and SPECT/CT: Important Tools for Preclinical Investigation
- Imaging of Gene Expression in Live Pancreatic Islet Cell Lines Using Dual-Isotope SPECT
- In vivo imaging of T cell delivery to tumors after adoptive transfer therapy
- Intramyocardial Implantation of Bone Marrow-Derived Stem Cells Enhances Perfusion in Chronic Myocardial Infarction: Dependency on Initial Perfusion Depth and Follow-up Assessed by Gated Pinhole SPECT
- Imaging Stem Cells Implanted in Infarcted Myocardium