


Abstract
Radiosynovectomy (RSV) is a local intraarticular injection of radionuclides in colloidal form for radiotherapy. First used by Fellinger et al. in 1952, the technique has now been applied for more than 50 y for treatment of resistant synovitis of individual joints after failure of long-term systemic pharmacotherapy and intraarticular steroid injections. RSV relieves pain and inflammation from rheumatoid arthritis (RA), for which it initially was used, and is accepted as an alternative to surgical synovectomy in cases of RA or other inflammatory arthropathies such as osteoarthritis and hemophiliac arthropathy. A good understanding of the clinical pathophysiology of the disease processes is mandatory, and close interdisciplinary collaboration with other clinicians who diagnose and treat patients is strongly suggested. Reported success rates range from 40% to 90% for the different joints and underlying diseases. A few well-designed prospective double-blind trials have evaluated the efficacy of RSV and justified the procedure as a viable option for treating chronic synovitis in RA or secondary to inflammatory arthropathies. In comparison with surgical synovectomy, RSV produces equivalent results, costs less, allows the patient to remain ambulatory, and is repeatable. RSV has to be considered the initial procedure of choice for the treatment of patients with hemarthrosis in hemophilia. In addition, local instillation of radiopharmaceuticals can effectively reduce effusions after implantation of a prosthesis.
With a prevalence of approximately 1%, rheumatoid arthritis (RA) is one of the most common autoimmune diseases (1). Destruction of diarthrodial or synovial joints causes pain, disability, and immobility in these individuals. The primary treatment for RA consists of various drugs administered systemically to reduce synovial inflammation. These include aspirin, nonsteroidal antiinflammatory agents, steroids, remission-inducing agents such as gold and penicillamine, low doses of antimetabolites, sulfasalazine, and tumor necrosis factor-α-blocker (2). Although, for the majority of the patients, RA can be controlled satisfactorily, long-term systemic therapy fails in some cases and its side effects accumulate to a serious level.
To prevent these side effects, intraarticular injections of corticosteroids have been used for effective local treatment. As an alternative, intraarticular injections of chemicals such as thiotepa and osmic acid have been developed and applied with limited success to stop chronic synovitis (3). Hemophiliac patients who have recurrent hemarthrosis are difficult to treat because “chemosynovectomy” with osmic acid may lead to massive hemorrhaging (4).
When drugs and local instillations have proven unsuccessful, surgical removal of the inflamed synovium has traditionally been the treatment of choice (5). Although surgical synovectomy has been successful, prolonged rehabilitation is necessary. Moreover, in hemophiliacs, the fear of uncontrollable hemorrhaging from the surgical procedure is widespread (6).
Radiosynovectomy (RSV) is a local form of radiotherapy that first was used by Fellinger et al. in 1952 (7) and has now been applied for more than 50 y for treatment of resistant synovitis of individual joints after failure of long-term systemic pharmacotherapy and intraarticular steroid injections (8–19). RSV relieves pain and inflammation from RA, for which it initially was used, and is accepted as an alternative to surgical synovectomy in cases of RA or other inflammatory arthropathies such as osteoarthritis and hemophiliac arthropathy (4,6,20,21).
RSV, or radiosynoviorthesis, is an intraarticular injection of a radionuclide in colloidal form. Three radionuclides are in current use: 90Y-silicate/citrate, 186Re-sulfide, and 169Er-citrate. These are approved in many countries for the treatment of painful arthropathy refractory to other treatment. They affect an inflamed synovium, which is the connective tissue lining a joint cavity (Fig. 1). Investigation of other potentially useful radionuclides, such as 188Rh-microspheres and 153Sm-particulate hydroxyapatite, is still relatively new. Some are experimental or commercially unavailable (22–26). A randomized double-blind human study showed, 1 y after treatment for chronic knee synovitis, no clear clinical benefit from use of combined 153Sm-particulate hydroxyapatite/triamcinolone hexacetonide injection over use of triamcinolone hexacetonide alone. Levels of unwanted extraarticular radiation have been shown to be negligible with these agents.
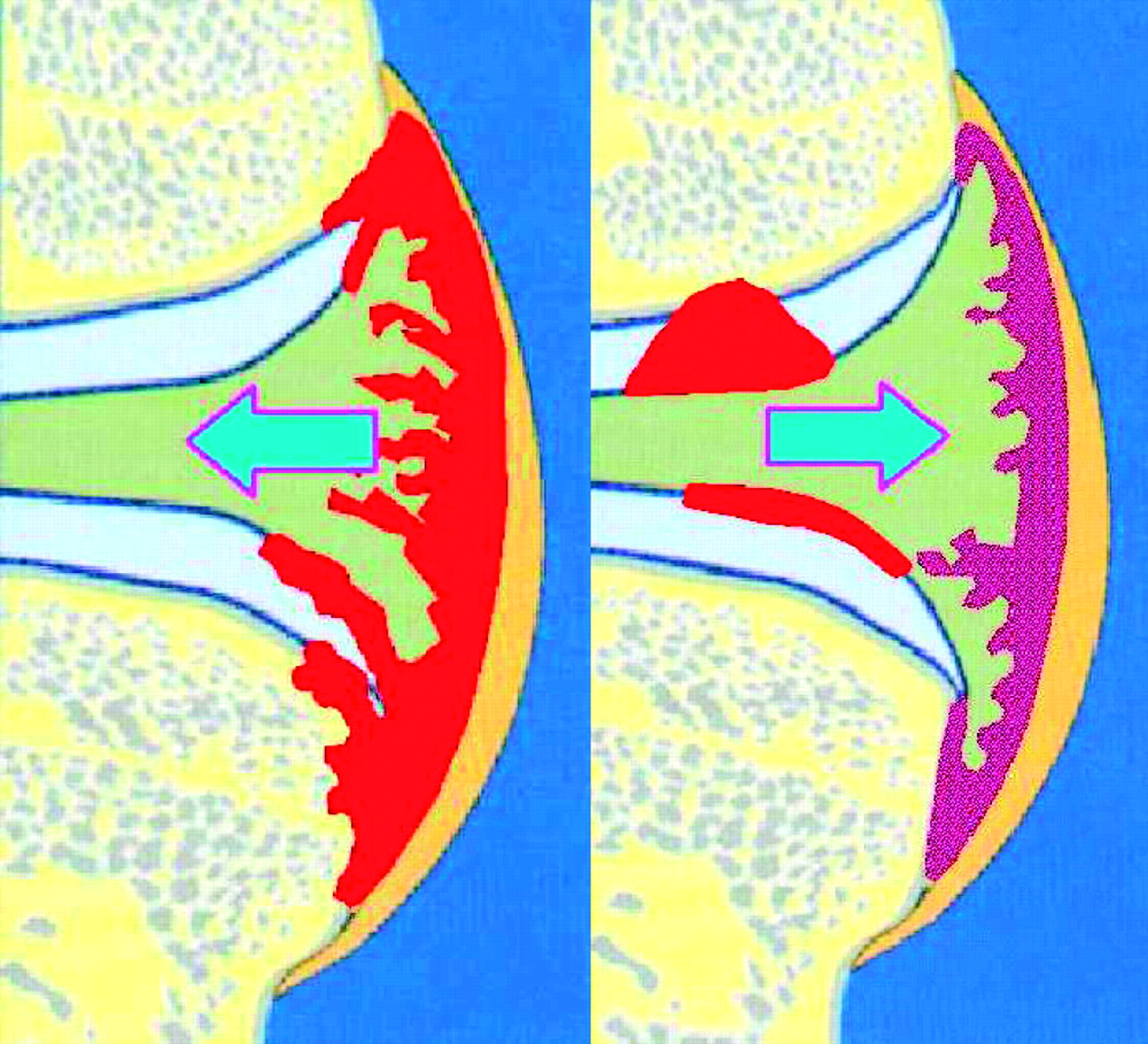
Synovitis in arthritis (left) and activated osteoarthrosis (right).
Good understanding of the clinical pathophysiology of the disease processes is mandatory, and the nuclear medicine physician should be familiar with other forms of therapy and patient management. Thus, close interdisciplinary collaboration with other clinicians who diagnose and treat patients is strongly suggested. These colleagues usually are rheumatologists or orthopedic surgeons who are assumed to take the role of the overall management of these patients.
PRINCIPLE
As shown by radioautography, radionuclide-loaded colloidal particles are rapidly phagocytized by macrophages in the inflamed synovial membrane (Fig. 2A). In synovial biopsies, colloidal particles are abundant in vacuolar cavities among the intercellular ground substance (27).

(A) β-Emitting colloidal particles (yellow stars) phagocytized by inflamed hypertrophic synovial lining with proliferating synoviocytes (pink). Top cartilage layer remains unaffected. (B) Subsequent cell damage and sclerosis of synovial membrane.
The ideal radiopharmaceutical for RSV should meet the following 3 requirements: It should be attached to a particle that is sufficiently small to be phagocytized but not so small that it might leak from the joint before being phagocytized (the appropriate size range is usually considered to be from 2 to 10 μm); binding between radionuclide and particle should be stable throughout the course of the RSV, which, in turn, is determined by the physical half-life of the radionuclide; and radiolabeled particles should be distributed homogeneously in the intraarticular space without initiating an inflammatory response.
These requirements are met by the radiocolloids listed in Table 1. 90Y-Colloid is suitable for the knee joint. 186Re-Colloid is used for medium-sized joints: hip, shoulder, elbow, wrist, ankle, and subtalar. 169Er is used for small joints: metacarpophalangeal, metatarsophalangeal, and digital interphalangeal. The activity to be administered and the injected volume vary according to the type of joint and the specific condition. Standard activities are listed in Table 2. In the United States, colloidal gold 198Au, 32P-chromic phosphate, and 165Dy-ferric hydroxide macroaggregate additionally are in use. However, because these radiopharmaceuticals have disadvantages such as high lymphatic transport, they are no longer mentioned in the guidelines of the European Association of Nuclear Medicine and the German Society of Nuclear Medicine (4,28,29).
Properties of Radiocolloids Used for Radiosynovectomy
Recommended Radionuclide and Activity per Injection for Radiosynovectomy of Different Joints
β-Particles cause ultimate damage to the absorbing medium—the cells of the synovial membrane—beginning with excitation and ionization of the atoms and molecules within this medium, creating a large number of secondary particles. Thus, free radicals known to initiate biochemical effects are created, with subsequent evolving apoptosis (30) and ablation of inflamed synovial membrane (Fig. 2B). Monte Carlo simulation has revealed absorbed doses per unit activity of 0.01–2 Gy/MBq in the synovial membrane, resulting (depending on radionuclide and disease state) in a dose of up to 100 Gy (18,31,32).
INDICATIONS AND CONTRAINDICATIONS
90Y-Silicate/citrate, 186Re-sulfide, or 169Er-citrate is indicated for treatment of joint pain in cases of the following established diagnoses (4,28,29): RA, undifferentiated arthritis characterized by synovitis, inflammatory joint diseases of other origin (Lyme’s borreliosis, psoriatic arthritis, ankylosing spondylitis), persistent synovial effusion (e.g., after endoprosthesis placement), osteoarthritis characterized by synovitis, villonodular synovitis, and hemarthrosis and synovitis associated with hemophilia.
After arthroscopy or joint surgery, including endoprosthesis placement, the interval before RSV should be 6 wk. The interval between joint puncture and RSV should be at least 2 wk. RSV may be repeated after a minimum of 6 mo.
Absolute contraindications for RSV include pregnancy, breast feeding, a ruptured Baker’s cyst (knee), local skin infection, and massive hemarthrosis. Relative contraindications include an age less than 20 y, evidence of significant cartilage loss, and joint instability with bone destruction. In patients younger than 20 y, the benefit of the treatment has to be greater than the potential hazard of the radionuclide.
DIAGNOSTIC PROCEDURES
Some patient-preparation procedures are essential, and some are optional. Usually, patients considered for RSV have a history of at least one intraarticular injection of a long-acting glucocorticoid without sufficient therapeutic effect. They usually will have pain severe enough to limit their normal activity and to require regular intake of systemic analgesics.
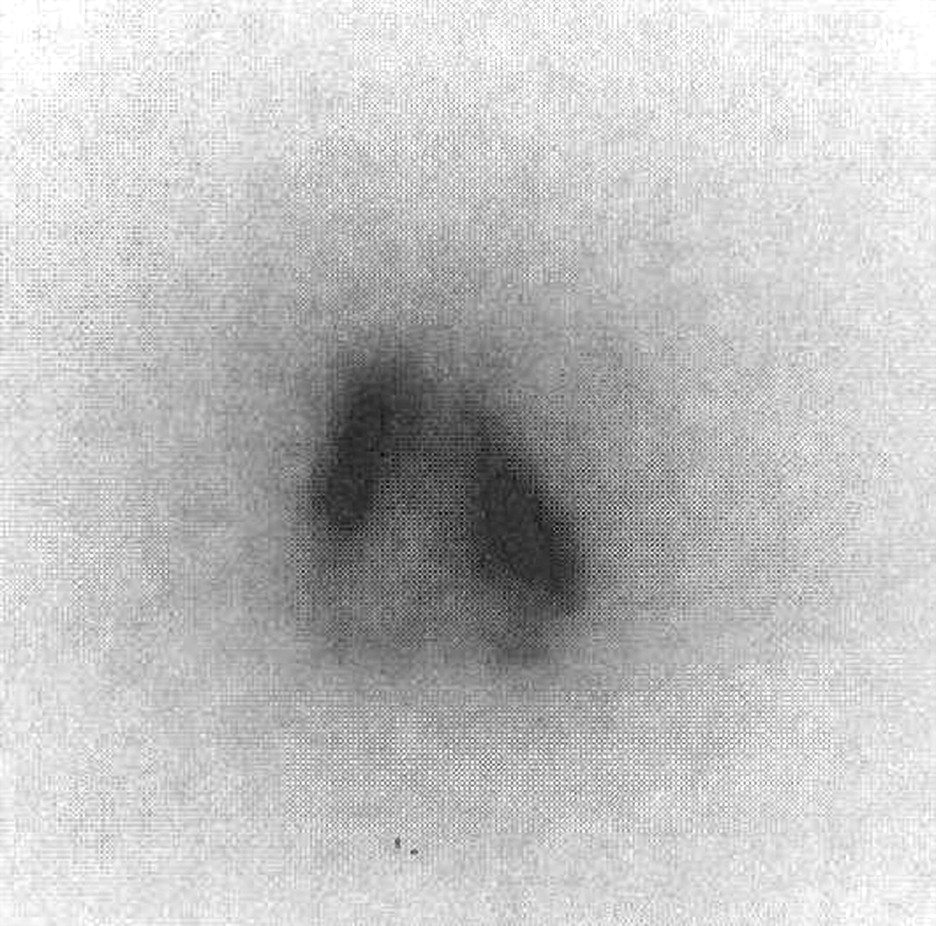
Candidates for RSV need to have undergone radiography or MRI of the joint no more than 6 mo previously. In addition, sonography of the joint may be helpful to evaluate synovial thickness and structure (33). For the knee, sonography is required to exclude a ruptured Baker’s cyst or hemarthrosis. Additionally helpful may be a 2- or 3-phase bone scan with 99mTc-phosphonate to assess the severity of active soft-tissue inflammation of the joints, particularly if multiple joints are affected (Fig. 3).

Two-phase bone scintigraphy using 600 MBq of 99mTc-methylene diphosphonate in a 34-y-old women with RA shows multiple inflamed joints. Right elbow was treated with 85 MBq of 186Re-sulfide; both proximal interphalangeal joints of the digitus secundus manus were treated later with 20 MBq of 169Er-citrate.
INFORMED CONSENT
Informed written consent from patients is mandatory. Information should be both verbal and written and should cover the procedure, its benefits, and its risks. A standard form developed for that specific treatment may be helpful. Patients should be informed about the radioactive nature of the treatment and its mechanism, indications, and contraindications. Patients should be told that response may be delayed by up to 1 mo, with further improvements up to 6 mo. Initially, a temporary increase in synovitis (and pain) may follow the treatment. Patients must be informed about possible side effects and complications, including the risks involved with puncture of a joint, such as infection, local hemorrhage, or extravasation; the risk of radionecrosis if injection is not strictly intraarticular (very rare); the future risk of malignancy (theoretic); the risk of postinjection pyrexia or allergy (very rare); and the risk of a thromboembolic event after immobilization of the lower limb for 48 h after treatment (antithromboembolic precautions have to be taken). The patient also has to be informed that the procedure is 60%–80% effective and may be repeated after at least 6 mo.
TECHNICAL PREREQUISITES
According to the guidelines of the European Association of Nuclear Medicine, the β-emitters should be administered in a dedicated room equipped for sterile injection procedures and approved for the use of β-emitters (28).
Measurement of β-emitting radionuclides is difficult. Dose calibrators may be used to indirectly measure the Bremsstrahlung of the radionuclides. For this purpose, the device should be specially configured to ensure a constant geometry for the holder of the syringe containing the β-emitter. Handling of the radionuclides requires special precaution because of the extremely high doses delivered to the fingers if syringes are touched directly at the zones containing the radionuclide. Appropriate shielding for β-emitting radionuclides is acrylic plastic (Fig. 4). Fingertip doses of up to 22.1 μSv/MBq have been observed when an appropriate shield was not used, compared with 0.4 μSv/MBq when a clamp and acrylic shield were used (34).

Injection of 169Er-citrate into proximal interphalangeal joint.
PROCEDURE
Injection into a joint must be performed under sterile conditions by medical and nursing staff, with support from physicists specially trained to use radioactive pharmaceuticals and to deal with potential contamination. Sterile gloves are mandatory. Before puncture, local skin anesthesia is advisable. Intraarticular puncture and injection have to be ensured. For the knee this is usually not difficult because intraarticular positioning of the needle (e.g., 7.6 cm [3 in.], 20 gauge) can be verified by aspirated synovial fluid.
The position of the needle in smaller joints may easily be controlled by radiography under fluoroscopic guidance, using a 22-gauge needle. Administration of just enough contrast medium to document that the needle is intraarticular is helpful (Fig. 5). A technique recommended for avoiding radioactive spills and radiation exposure is to hold the needle with a clamp strictly in position after these manipulations and then to remove the hose and only afterward attach the β-emitter syringe for the injection. Different techniques may be equivalently useful and appropriate. A most comprehensive description of techniques, enriched with figures, is given in a booklet by Mödder (16), although written in German.

Radiography of interphalangeal joint documents intraarticular location of needle and good distribution of small amount of contrast medium.
Simultaneous administration of 0.9% saline solution is advisable to achieve a sufficient distribution volume (Table 2). Long-acting glucocorticoids may be injected to reduce the risk of acute synovitis. In any case, before removal of the needle, flushing with saline solution is recommended to keep the puncture channel free of β-emitting particles. Usually this is difficult or impossible in small joints (fingers) because of the very small intraarticular volume. Sterile compression should be applied, and the joint should be immobilized for 48 h using appropriate methods (e.g., splints).
If several joints are treated in a single session, hospitalization may be advisable. Before the patient is released, posttherapy imaging should be done when γ-emitting 186Re has been applied. After application of 90Y, Bremsstrahlung imaging should be done to document appropriate intraarticular distribution of the radionuclide (Fig. 6).

Bremsstrahlung scintigraphy shows good intraarticular 90Y-silicate distribution 30 min after injection into knee joint. No activity is found extraarticularly or in puncture channel.
SIDE EFFECTS
As an early side effect, a temporary increase in joint pain due to radiation-induced synovitis may be observed. Lymphedema or fever may occur in rare cases (35).
Serious late side effects such as radionecrosis are very rare. Induction of malignancy is a theoretic potential side effect but has never been observed (36).
INSTRUCTIONS FOR PATIENTS
The patient has to be advised to keep the injected joint immobilized for at least 48 h. If early aggravation of pain occurs, it can be treated with simple antiinflammatory measures. A review is recommended 4–6 d (or earlier) after injection for possible side effects.
The patient should avoid unnecessarily exposing family members and the public to radiation. Various country-specific rules may apply in this regard. Women should avoid pregnancy for at least 4 mo after the treatment. Radiopharmaceutical excretion is not a concern in these patients because the application is local. In Germany, for example, no special requirement exists regarding urinary or bowel excretion. However, enhanced hygienic measures should be observed.
FOLLOW-UP
After 3–4 mo, the nuclear medicine specialist should or must (according to national regulations) reevaluate inflammatory activity of the synovial membrane and therapy response. Ultrasound, 2- or 3-phase bone scintigraphy, or MRI may be of value to document the status. Reevaluation can also be interdisciplinary, involving the rheumatologist or orthopedic surgeon as the physicians primarily taking care of these patients.
RESULTS
Many publications have reported results for RSV in patients treated for various indications. Interestingly, the results seem not to have depended greatly on factors such as indication for treatment, size of joint, radiocolloid applied, and method used to determine efficacy of treatment. The success rates ranged from 40% to 90% for the various joints and underlying diseases (11,17,37,38). Deutsch et al. (10) summarized the results of 72 studies performed between 1975 and 1992 on patients with RA. After 1 y of follow-up, the results of treatment were classified as good or excellent for 60%–80% of the patients. Recently, the efficacy of RSV in patients with osteoarthritis or other diseases not caused by RA has been studied in more detail. In these patients, similar results were observed, with response rates between 40% and 80% (20,37). We studied prospectively the time to remission after RSV and the influence of underlying disease, type of joint, duration of illness, and age and sex on the success rates of RSV. Visual analog scales were used to monitor improvement of pain after RSV, and the time until remission was determined according to the Kaplan-Meier survivorship function. The influence of the prognosis parameters on outcome was determined by multivariate discriminant analysis. After 6 mo, the probability of more than 20% pain relief amounted to 78% and was significantly dependent on the age of the patient (P = 0.02) and the duration of illness (P = 0.05). However, no influence was found for sex (P = 0.17), underlying disease (P = 0.23), and type of joint (P = 0.69) (37). Thus, RSV is effective not only in RA but also in activated osteoarthrosis (with effusion). Figure 7 shows that the intensity of pain measured by visual analog scales after RSV differs considerably between individuals (P. Schneider et al., unpublished data).

Pain intensity in 4 patients documented by visual analog scale (range, 0–100) over 3 mo, beginning 10 d before RSV: immediate long lasting success (A); protracted remission (B); unsuccessful treatment (C); and temporary success, mostly due to placebo effect (D). Green = morning; red = noon; blue = evening.
Few well-designed prospective double-blind trials have evaluated the efficacy of RSV (39–41). Overall, the efficacy that has been found (Table 3) justifies the viability of the procedure as an option for treating chronic synovitis in RA or secondary to inflammatory arthropathies. In comparison with surgical synovectomy, RSV produces equivalent results, costs less, allows the patient to remain ambulatory, and is repeatable (2,4).
Success Rates for Radiosynovectomy of Different Joints
For patients in whom chronic effusions develop after arthroplasty (e.g., of the knee), RSV is able to stop the effusions effectively (16).
For patients with hemophilia, the results of RSV are comparable to those for other underlying diseases. According to the review of Deutsch et al. from 1993 (10), 9 studies published between 1982 and 1991 reported good-to-excellent results for RSV in 60%–80% of patients with hemarthrosis because of hemophilia. These results are underlined by recent data of Siegel et al. (4), who reported a significantly decreased incidence of bleeding in 70%–80% of the patients, resulting in considerably lower treatment costs for RSV than for the conventional surgical approach requiring intensive use of clotting factors.
The radiation dose to the gonads is negligible, and the hypothetical morbidity from induction of tumors by whole-body radiation is low. An increased risk for cancer after RSV has not been reported (36).
CONCLUSION
RSV should be considered the initial procedure of choice for the treatment of patients with hemarthrosis in hemophilia. In patients with chronic synovitis secondary to RA or activated arthrosis, the results of RSV are favorable. In addition, local instillation of radiopharmaceuticals can effectively reduce effusions after implantation of a prosthesis.
Footnotes
Received May 3, 2004; revision accepted Aug. 13, 2004.
For correspondence or reprints contact: Peter Schneider, Prof.Dr.med., Clinic for Nuclear Medicine, Josef-Schneider-Strasse 2, D-97080 Würzburg, Germany.
E-mail: Schneider_P{at}nuklearmedizin.uni-wuerzburg.de
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Lutetium-177 hydroxyapatite radiosynovectomy in refractory chronic inflammatory arthritis of the knee joint
- Safety and Efficacy of Radiosynoviorthesis: A Prospective Canadian Multicenter Study
- Single-joint Outcome Measures: Preliminary Validation of Patient-reported Outcomes and Physical Examination
- Local delivery of a recombinant adenoassociated vector containing a tumour necrosis factor {alpha} antagonist gene in inflammatory arthritis: a phase 1 dose-escalation safety and tolerability study
- Effects of Gamma Radiation on Fc{varepsilon}RI and TLR-Mediated Mast Cell Activation
- The intra-articular distribution of 90yttrium does not influence the clinical outcome of radiation synovectomy of the knee
- Radiation synovectomy with yttrium-90 for persisting arthritis has direct harmful effects on human cartilage that cannot be prevented by co-administration of glucocorticoids: an in vitro study