


Abstract
Systemic therapy using bone-seeking radiopharmaceuticals has clear advantages for the treatment of multisite metastatic pain. Evidence supporting the use of β-particle, electron, and α-particle–emitting radiopharmaceuticals is reviewed here. Appropriate patient selection relies on correlating clinical symptoms with focal abnormalities on conventional bone scintigraphy. Time to symptom relief and response duration vary with the physical half-life and dose rate of the radionuclide used, offering the opportunity to tailor radiopharmaceutical choice to individual patient circumstances. Toxicity is limited to temporary myelosuppression, governed by the administered activity and underlying bone marrow reserve. Optimal responses are achieved in patients with a modest skeletal tumor burden, suggesting that targeted therapy should be considered early in the management of bone metastases. The development of reliable dosimetric models will facilitate patient-specific prescribing to deliver enhanced symptom response within acceptable toxicity limits. It is likely that targeted therapy will be most effective in the context of multimodality tumor management. Further research is required to examine the potential of radionuclides in combination with external-beam irradiation, bisphosphonates, or chemotherapy. This approach might allow targeted therapy to progress beyond symptom palliation to early intervention for survival gain.
Bone pain is a common symptom in advancing malignancy and often determines quality of life in the later stages of disease (1). Improved survival resulting from advances in hormone treatment and chemotherapy, paradoxically, has increased the population of patients with skeletal metastases seeking symptom relief. The long-term management of refractory bone pain requires a multidisciplinary approach and close cross-specialty liaisons.
Moderate, localized skeletal symptoms are usually controlled by conventional analgesics, prescribed according to the World Health Organization (WHO) pain ladder, followed by single-fraction external-beam radiotherapy for persisting, limiting discomfort (2). This approach becomes less useful in the context of progressive skeletal metastases, which result in poorly localized or migratory multisite pain. Wide-field, hemibody radiotherapy is an effective treatment option, but potential benefit is often outweighed by significant bone marrow and gastrointestinal toxicity. Bisphosphonates target osteoclast-mediated bone resorption and reduce the skeletal complication rate arising from osteolytic metastases in breast cancer and myeloma (3,4). Their role in hormone-refractory prostate cancer (HRPC) is less well established, and controlled trials are required to determine the optimal agent, mode of administration, dose, and treatment duration (5).
Acting systemically, targeted therapy using bone-seeking radiopharmaceuticals are well suited to the management of disseminated disease when repeated local treatment becomes impractical. The potential toxicity of systemic administration is reduced by relatively selective tumor targeting.
Radionuclide therapy for bone pain palliation has been used successfully for more than 30 y. The early development of therapeutic radiopharmaceuticals was governed by scientific standards in place in the 1970s and 1980s and, in many cases, would not meet current criteria for evidence-based practice. The lack of randomized controlled trials, however, does not diminish the quality of experience reported in earlier peer-reviewed publications that provided incontrovertible support for the efficacy and tolerability of targeted therapy.
RADIONUCLIDE SELECTION CRITERIA
Treatment success depends on matching the physiologic characteristics of the target tissue to a specific pharmaceutical carrier and optimal radionuclide. Bone targeting relies on selective uptake and prolonged retention at sites of increased osteoblastic activity. Some therapeutic radionuclides, such as 89Sr and 223Ra, have a natural affinity for metabolically active bone. Others, including samarium and rhenium, form stable complexes with bone-seeking cations, such as phosphate and diphosphonate.
It is important that the physical half-life of the radionuclide used matches the biologic turnover of the radiopharmaceutical in vivo. The clinical significance of half-life as a determinant of dose rate and time to response is discussed more fully later in this article. Particle range influences treatment-related toxicity. Whereas the energy of short-range electron- or α-particles is largely absorbed within the target cell, longer-range β-particles may irradiate surrounding healthy tissues, contributing to unwanted side effects.
Experience has focused largely on β-particle–emitting radionuclides, although recent attention has been drawn to electron- and α-emitters. The physical characteristics of therapeutic radionuclides for bone pain palliation are summarized in Table 1. Evidence supporting the use of different radiopharmaceuticals is discussed here, and administered activities, typical responses, and retreatment intervals are listed in Table 2.
Physical Characteristics of Therapeutic Radionuclides for Bone Pain Palliation
Administered Activities, Typical Response Times and Duration, and Retreatment Intervals for Bone-Seeking Radionuclides
RADIOPHARMACEUTICALS FOR BONE PAIN PALLIATION
32P
32P decays by 1.7 MeVEmax β-emission and has a physical half-life of 14.3 d. The maximum particle range in tissue is approximately 8.5 mm. Eighty-five percent of total body phosphate is held within the skeleton, bound as inorganic phosphate to hydroxyapatite. Radiophosphorus, administered intravenously as 32P-sodium orthophosphate for skeletal targeting, was used extensively in the 1970s to treat metastatic HRPC (6). Equal success after oral administration has been reported more recently (7). Approximately 5%–10% of the administered activity is renally excreted within 24 h.
Animal data demonstrate increased radiophosphorus uptake in reactive bone surrounding osteoblastic metastases by a factor of 3:1 to 5:1 compared with normal bone. The red marrow absorbed dose approaches 6.5 mGy/MBq, reflecting contributions from the inorganic bone matrix and from the cellular component of the marrow space (6,8).
Published experience includes a range of fractionated treatment schedules, administering activities of 300–740 MBq over 7–40 d (9). Pretreatment with testosterone or parathormone was shown to stimulate osteoblastic activity around metastases, enhancing the therapeutic ratio by up to 20:1 in tumor versus normal bone (10). The potential benefit of this approach was outweighed by the risk of soft tissue tumor progression in hormone-sensitive tumors. Limited rodent dosimetry data predicted total bone doses in the order of 0.4–1.7 cGy/MBq, but these results cannot be reliably extrapolated to the metastatic human skeleton (8).
Pain relief was reported by 50%–87% of patients with metastatic prostate cancer treated with 200–800 MBq of 32P administered in daily 20- to 80-MBq fractions after androgen priming. Symptom benefit occured within 5–14 d, with mean response duration of 2–4 mo (11).
The main disadvantage of 32P therapy is dose-limiting myelosuppression with reversible pancytopenia maximal at 5–6 wk after administration (12). Toxicity appears cumulative and activity related. Although toxic deaths are very rare, 9 of 30 patients in one study required transfusion support after treatment (13,14). Complications arising from leukopenia and thrombocytopenia have not been considered in depth.
Although 32P is rarely used for bone pain palliation in North America and Western Europe, the significant cost advantage and ease of oral administration compared with licensed alternatives have regenerated interest in this agent as the radiopharmaceutical of choice for bone pain palliation elsewhere in the world. An open-label study comparing single, oral administration of 444 MBq of 32P with intravenous administration of 148 MBq of 89Sr demonstrated equal efficacy and toxicity in 31 patients with painful skeletal metastases. Clinically significant myelosuppression was not observed (7).
89Sr
89SrCl2 decays by 1.4 MeV (Emax) β-emission with a physical half-life of 50.5 d. The maximum particle range in tissue is approximately 7 mm. As a group II metal, strontium has a natural affinity for metabolically active bone. Biodistribution studies undertaken using the γ-emitter 85Sr demonstrated a therapeutic ratio of 10:1 for tumor to normal bone (15). Excretion is predominantly renal, dictated by skeletal tumor burden and glomerular filtration rate (16). Strontium plasma renal clearance is significantly reduced in patients with bone metastases compared with the International Commission on Radiological Protection standard man. The biologic half-life in normal bone is around 14 d compared with more than 50 d in osteoblastic metastases.
Tumor absorbed doses of 21 ± 4–231 ± 56 cGy/MBq have been calculated (17). No activity–response relationship has been demonstrated, although pooled data from several small studies suggested a threshold activity of 1 MBq/kg below which 89SrCl2 therapy appeared ineffective and a response plateau above 1.5 MBq/kg (18). The licensed administered activity is 148 MBq.
A systematic review of published data reported pain relief in approximately 74% of patients (19). Most series were published before the introduction of quality-of-life assessments and are therefore based on subjective response criteria, supported by objective reductions in analgesic strength and dose. A double-blind randomized study confirmed that 89SrCl2 is more effective than stable 86Sr and 88Sr as a placebo (20). 89SrCl2 was subsequently shown to be as effective as both local field and hemibody external-beam radiotherapy in relieving existing bone pain but delayed the development of new pain at preexisting, clinically silent sites (21). This observation was confirmed in the Trans-Canada study (22) but later contradicted by Smeland et al. (23). This discrepancy may reflect the higher 89SrCl2 activity (400 MBq) administered in the Trans-Canada trial compared with the 148-MBq licensed activity used in the Smeland study.
The toxicity of treatment is limited to temporary myelosuppression, which typically occurs <6 wk after therapy. Recovery is typically slow over the next 6 wk, dictated by tumor skeletal extent and bone marrow reserve.
The potential of combined chemoradiation therapy has been assessed in randomized phase 2 trials. 89SrCl2 with low-dose cisplatin achieved 91% pain response compared with 63% pain response with 89SrCl2 alone (P < 0.01) and appeared to slow the rate of skeletal metastatic progression (24). Tu et al. (25) reported improved survival using 6 weekly administrations of 89SrCl2 with doxorubicin after induction chemotherapy compared with 6 weekly administrations of doxorubicin alone. A nonrandomized study using 12 weekly administrations of estramustine phosphate, vinblastine, and 89SrCl2 recorded effective, durable symptom palliation, >50% reduction in prostate-specific antigen (PSA) in 48% of treated patients, and reduced demand for subsequent palliative radiotherapy (26). In all 3 studies, combined chemoradiation therapy was consistently well tolerated without significant additional hematologic toxicity.
186Re
186Re is a medium-energy β-emitter (Emax = 1.07 MeV) with a physical half-life of 89 h. Rhenium forms a stable bisphosphonate complex with hydroxyethylidene disphosphonate (HEDP). Peak skeletal uptake occurs 3 h after intravenous administration. The mean biologic half-life in bone metastases ranges between 45 ± 6 h (mean ± SD) and 59 ± 10 in breast and prostate lesions, respectively (27). Uptake is directly proportional to the metastatic tumor burden, as assessed by the bone scan index (BSI). Clearance is predominantly renal, with 69% ± 15% occurring within 24 h of administration (28).
Activity-escalation studies have established the maximum tolerated activity per single administration as 2,405 and 2,690 MBq in breast and prostate cancer, respectively (29). Lesion-to-marrow absorbed dose estimates in the range of 20–30:1 have been reported using conventional MIRD calculations (30). Subsequent revision by the same group, based on Monte Carlo modeling, suggested significantly higher absorbed dose to osteoblastic lesions than previously predicted (31).
Eighty to ninety percent of patients reported symptom benefit after a single 186Re-HEDP administration. Response was typically rapid, occurring within 24–48 h of activity administration. Placebo-controlled, randomized studies confirmed the efficacy of 186Re-HEDP (32,33).
Toxicity is limited to temporary myelosuppression, with platelet and neutrophil nadirs at 4 wk after therapy. Recovery occurs within 8 wk and is usually complete. In the prostate cancer population, hematologic toxicity can be reliably predicted from the BSI normalized to body surface area (29). Toxicity is less predictable in breast cancer patients, probably because of the effects of previous combination chemotherapy (34). Limited data support an activity–response relationship using 186Re-HEDP in patients with HRPC. Symptom benefit was reported in more than 70% of patients using activities in the range of 1.85–2.4 GBq (35). Temporary changes in biochemical markers have been observed in patients treated with higher activities. In a single study, O’Sullivan et al. (36) documented a transient decrease in PSA in HRPC patients receiving more than 3.5 GBq 186Re-HEDP with peripheral stem cell rescue. de Klerk et al. (37) previously reported a temporary fall in bone alkaline phosphatase in patients receiving relatively high administered activities in phase 1 trials.
Temporary pain flare has been reported in up to 50% of patients treated with 186Re-HEDP, with case reports of cranial nerve palsy (38). This is attributed to endosseous edema and is controlled by temporary analgesic increase and corticosteroids.
188Re
The therapeutic potential of 188Re has generated recent interest. 188Re has a short physical half-life of 16.9 h and a maximum β-particle energy of 2.1 MeV. The maximum β-range in tissue is approximately 10 mm. 188Re is produced from a 188W (188W/188Re) generator, which offers significant advantages in terms of availability and convenience compared with other therapeutic radionuclides. As with 186Re, targeting is achieved by chelation with HEDP.
Blood clearance is rapid after intravenous injection, with 41% renal clearance within 8 h of administration. The mean effective whole-body half-life is 11.6 ± 2.1 h compared with 15.9 ± 3.5 h in bone metastases. Absorbed doses for bone metastases are in the range of 3.83 ± 2 mGy/MBq, in comparison with 0.61 ± 0.2 mGy/MBq for bone marrow and 0.07 ± 0.02 mGy/MBq for whole body (39). Open-label activity-escalation studies over the range of 1.3–4.4 GBq reported symptom benefit in 64% of patients with HRPC, with 75% response in the 4.4-GBq cohort (40). Toxicity was hematologic, reaching WHO grades 3 and 4 thrombocytopenia at higher administered activities. The maximum tolerated activity was established at 4.4 GBq in patients with normal marrow reserve, reduced to 3.3 GBq in patients with pretreatment platelet levels <20 × 109/L. Similar response rates, associated with improved Karnofsky status, have been confirmed in subsequent studies (41).
The short physical half-life and high dose rate are predicted to lead to rapid symptom response. Fractionated therapy has been shown to prolong response duration and progression-free survival in a small series (42). Further randomized clinical trials are in progress.
153Sm
153Sm has a physical half-life of 46.3 h and decays by the emission of a 0.81 MeV (Emax) β-particle. Samarium forms a stable complex with ethylenediaminetetramethylenephosphonate (EDTMP). Clearance is biexponential after intravenous administration, comprising rapid bone uptake (half-life = 5.5 min) and plasma renal clearance (half-life = 65 min) (43). Fifty percent of injected activity is excreted renally within 8 h of administration. Total skeletal uptake ranges between 55% and 75%, depending on the skeletal tumor burden (44). 153Sm-EDTMP targets hydroxyapatite at sites of increased osteoblastic activity, the tumor-to-normal bone ratio being 4:1–7:1 (45). Autoradiographic studies confirm that activity is associated with the bone surface (46). The short-range β-emission mean pathlength is 3.1 mm in soft tissues and 1.7 m in bone.
Sixty-five to eighty percent of patients reported pain relief after 153Sm-EDTMP administration in early phase 1/2 open-label studies (47,48). Symptom response is typically rapid, occurring within 1 wk of administration, frequently within 48 h. Response duration is typically 8 wk (range, 4–35 wk) (48). An activity-escalation study (37–111 MBq/kg) reported symptom benefit in 70%–80% of 36 patients with HRPC. Pain relief was observed at each activity level but not in all patients in each cohort (49). Toxicity was limited to activity-dependent, temporary myelosuppression with a nadir at 6 wk. Subsequent phase 2 dose escalation studies confirmed the maximum tolerated marrow dose as 2 Gy (50). The maximum tolerated activity was 166 MBq/kg (51).
Larger, randomized, double-blind, placebo-controlled studies reported consistently high clinical efficacy on the basis of visual analog score and physician’s global assessment and established the optimal administered activity as 37 MBq/kg (52,53).
A trend toward improved response rates, superior response quality, and prolonged survival was reported in patients receiving higher administered activities (49,53). Higher activities correlated with improved PSA and alkaline phosphatase (49).
Treatment has been repeated safely for recurrent symptoms and appears well tolerated (54). Pain flare is rare, occurring in approximately 10% of published series (55). High-activity therapy with peripheral blood stem cell rescue has been used to treat bone metastases and osteosarcoma (56). Lesion-absorbed doses of 39–241 Gy were estimated after administration of 37–1,110 MBq/kg of 153Sm-EDTMP.
117mSn
The premise that the efficacy of other bone-seeking radionuclides is limited by myelotoxicity has stimulated interest in the therapeutic potential of short-range electron emitters. 117mSn(4+) decays by the emission of low-energy conversion electrons (Emax = 0.13 and 0.16 MeV) and a low-abundance 159 keV γ-photon. The physical half-life is 13.6 d. Optimal blood and soft tissue clearance is achieved by chelation with diethylenetriaminepentaacetic acid (DTPA) (57). Dosimetric studies in a mouse femur model determined the mean femoral marrow absorbed dose as 0.043 cGy/MBq compared with a mean absorbed dose to bone of 1.07 cGy/MBq (58). Human studies confirm biexponential whole-body clearance after intravenous 117mSn-DTPA injection. The average soft tissue biologic half-time is 1.45 d, accounting for 22.4% of the administered activity. The bone component accounts for 77.6% of injected activity and shows no biologic clearance, and 22.4% of administered activity is cleared renally. Peak bone uptake occurs in normal bone within 24 h, but metastatic skeletal uptake occurs slowly over 3–7 d (59). The first phase 1 activity escalation study conducted over the activity range of 66–573 MBq reported symptom benefit in 9 of 10 evaluable patients with no significant myelotoxicity (60). A later phase 1/2 activity escalation study in 47 patients with painful bone metastases reported a 75% overall pain response (range, 60%–83%), with complete pain relief in 30% (61). The typical response time was 19 ± 15 d using activities of ≤5.29 MBq/kg and 5 ± 3 d in patients receiving activities of ≥6.61 MBq/kg. Myelotoxicity was minimal, with 1 patient experiencing grade 3 white cell count toxicity. The outcomes of additional trials are awaited.
223Ra
Recent attention has focused on the α-emitter 223Ra, administered as 223Ra-chloride (223RaCl2). Like calcium, radium has a natural affinity for metabolically active bone. The physical half-life is 11.4 d. Blood clearance is rapid after intravenous administration. Peak skeletal uptake occurs within 1 h of injection, with no subsequent redistribution (62). Unlike most other bone-seeking radionuclides, excretion is predominantly via the gastrointestinal tract, with less than 10% renal clearance (62). 223Ra decays by the emission of 4 α-particles via daughter isotopes to stable 207Pb. The total decay energy is 28 MeV. 223RaCl2 is selectively concentrated on bone surfaces relative to soft tissues in murine models, leading to relative marrow sparing. Limited absorbed dose estimates indicate a tumor-to-marrow ratio of 30:1. Preclinical and pilot phase 1 activity-ranging studies have failed to demonstrate limiting toxicity. Temporary myelosuppression is reported but has not exceeded WHO grade 1, even at high activities (200 kBq/kg) in heavily pretreated patients. The low-grade toxicity reported is attributed to the short (100-μm) α-particle range in tissue. Common side effects include diarrhea and nausea or vomiting, which appear activity related in a small phase 1 study. Phase 1 data suggest superior response after fractionated administration compared with a single high-activity therapy. Phase 2 randomized, placebo-controlled studies are in progress.
PATIENT SELECTION CRITERIA
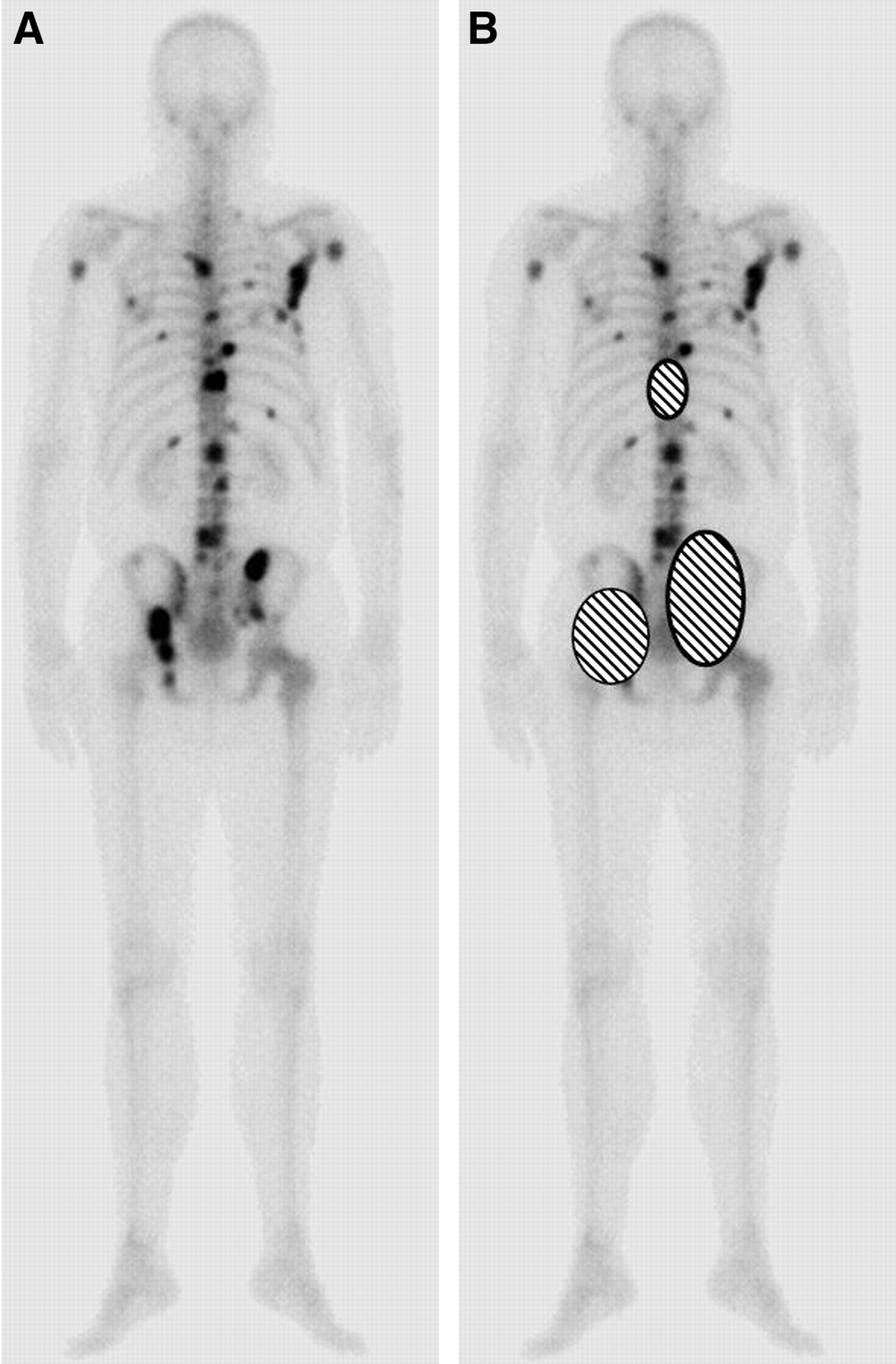
The most common explanation for treatment failure is inappropriate patient selection. It is essential that patients undergo tracer 99mTc-methylene diphosphonate (99mTc-MDP) bone scintigraphy shortly before planned treatment administration. Foci of increased uptake on the bone scan can then be correlated with a “body map” of the patient’s symptoms to ensure that sites of discomfort can be directly attributed to osteoblastic bone metastases. An example of symptom mapping is given in Figures 1A and 1B. Common sources of symptom confusion in this patient population include vertebral collapse, nerve root entrapment, fracture, and visceral pain, none of which will respond to radionuclide therapy.

(A) Posterior whole-body 99mTc-MDP bone image of patient with hormone-refractory prostate cancer. (B) Pain sites (cross-hatched) correlate exactly with foci of increased osteoblastic activity.
Optimal results are obtained where pain sites match areas of increased 99mTc-MDP uptake that are likely to concentrate and retain bone-seeking radiopharmaceuticals. Response is less predictable in patients with a predominantly osteolytic pattern of skeletal metastasis, presumably because poor uptake and retention result in a lower metastatic absorbed radiation dose.
Patients should be hematologically and biochemically stable before treatment. Hemopoietic reserve can be assessed by correlating the peripheral full blood count with tumor extent on conventional bone scintigraphy. Diffuse infiltration, the superscan appearance, or increased uptake in the proximal long bones indicate extensive marrow replacement by tumor and are unfavorable prognostic features. 99mTc-MDP imaging predicts myelotoxicity more reliably than bone marrow scintigraphy (63). In the palliative care setting, formal bone marrow examination is rarely appropriate.
Poor renal function will delay clearance of most bone-seeking radiopharmaceuticals, leading to a higher whole-body dose and, potentially, increased toxicity. Modest renal impairment is common in the elderly HRPC population, but outflow obstruction at the vesicoureteric junction or bladder neck should be treated appropriately before radionuclide administration (Fig. 2).

Unsuspected bilateral vesicoureteric junction obstruction in advanced prostate cancer. Lumbar discomfort was relieved by ureteric stenting. Targeted radionuclide therapy would not have controlled dominant symptom, and poor excretion might have increased renal and whole-body doses.
Contraindications to treatment include acute or chronic renal failure, risk of imminent pathologic fracture, and acute spinal cord compression, which should be regarded as a surgical or radiotherapy emergency. Urinary incontinence presents a contamination risk and should be managed by bladder catheterization before radiopharmaceutical administration. Criteria for patient selection are summarized in Table 3.
Criteria for Patient Selection for Bone-Seeking Radionuclide Therapy
The value of early treatment is well recognized. Although patients with extensive skeletal disease may report dramatic pain relief, the quality of response is generally better in patients with a moderate skeletal tumor burden (18,63). Taken with evidence that treatment delays the development of new pain in preexisting, clinically silent sites, there is a strong argument for early intervention, particularly in HRPC (21,22). Clinical trials investigating the potential of targeted therapy in patients with asymptomatic bone metastases are in progress.
Growing understanding of the characteristics of specific radiopharmaceuticals allows treatment selection to be tailored to individual patient circumstances. Important considerations include time to response, predicted response duration, and bone marrow reserve. Patients with relatively early metastases (Fig. 3), a favorable prognosis (life expectancy >6 mo), reasonable pain control using conventional analgesics, and normal marrow function are particularly likely to derive sustained benefit from 89SrCl2. By comparison, patients with more advanced metastases (Fig. 4), severe pain, and limited marrow reserve would be more appropriately treated using 153Sm-EDTMP or 186Re-HEDP.

99mTc-MDP bone image of patient with early metastases.

99mTc-MDP bone image of patient with diffuse metastases.
RETREATMENT
Treatment can be repeated safely for recurrent pain (64). Selection criteria for re-treatment should repeat the rationale outlined for the first administration and include bone scintigraphy and hematologic and renal assessment. It may be preferable to treat single-site pain recurrence using external-beam radiotherapy, keeping unsealed source treatment in reserve for multifocal symptom relapse. The quality of response may decrease with successive treatments, although most studies report continuing benefit (65).
TOXICITY
The critical organ for treatment using bone-seeking radiopharmaceuticals is the bone marrow. Most patients develop temporary myelosuppression 4–8 wk after therapy, with full or partial recovery over the next 3 mo. The rate and completeness of recovery depend on the radionuclide administered, prescribed activity, and, critically, on underlying bone marrow reserve. The latter is particularly relevant in patients who have received previous chemotherapy or external-beam radiotherapy where large or overlapping treatment fields have included a significant proportion of remaining bone marrow. Myelotoxicity is cumulative in patients receiving repeated radionuclide therapies for recurrent symptoms, but the toxicity of repeated therapy is not easily distinguished from the effects of underlying tumor progression.
Toxicity is increased in patients with subclinical disseminated intravascular coagulation (DIC), which affects 10%–20% of patients with advanced prostate carcinoma. It is recommended that patients with extensive disease be routinely screened for DIC pretreatment (66).
Acute myeloid leukemia was reported in 2 patients 17 and 26 mo after 89SrCl2 therapy (67). A causal relationship was inferred on the basis of historical 90Sr data, but both patients had been heavily pretreated with external-beam irradiation, cytotoxic chemotherapy, and investigational drugs, making the postulated link between 89Sr and leukemogenesis unclear. The current trend toward earlier intervention for patients with longer life expectancies than previous treatment populations justifies increased vigilance, although any leukemogenic risk is likely to be outweighed by the benefit of long-term pain control. There is no evidence that targeted therapy increases the toxicity of subsequent chemotherapy.
MECHANISM OF ACTION AND FUTURE DIRECTION OF TARGETED THERAPY
The mechanism of bone pain palliation by ionizing radiation is poorly understood. Experience from external-beam irradiation indicates that the absorbed dose required to achieve pain relief is significantly lower than would be necessary to achieve a tumoricidal effect. Pain palliation, therefore, cannot depend solely on clonogenic cell kill.
The etiology of metastatic pain is likely to involve both mechanical and humoral factors. Mechanical factors include direct bone invasion, microfractures, increased intramedullary pressure, and periosteal stretching. High–dose-rate, external-beam irradiation induces tumor shrinkage, thereby reducing pressure effects and periosteal stimulation. These effects are not instantaneous, however, and mechanical change cannot explain the rapid symptom relief reported after hemibody radiotherapy. Similarly, the lower dose rate delivered by targeted radionuclides is unlikely to improve pain resulting from mechanical stress within 48 h as documented after 153Sm-EDTMP and 186Re-HEDP therapy.
The observation that pain palliation is independent of tumor radiosensitivity suggests that the site of action of palliative radiotherapy might be the interface between tumor and normal bone, or normal bone itself (68). Exposure to ionizing radiation is known to activate the early-response gene cascade, regulating downstream genes that, in turn, modify cellular cytokine and growth factor release (69). Radiation-induced humoral changes within normal osteocytes and in the surrounding microenvironment may be an important mechanism in symptom relief.
Time-to-response differences after the administration of long–and short–half-life targeted radionuclides are a function of dose rate and suggest a “threshold” absorbed dose for pain relief. This threshold would be achieved early using a short–half-life isotope, such as 153Sm or 186Re, but would be delayed after 89Sr administration. The observation from both external-beam and targeted therapy data that around 25% of patients fail radiation therapy supports the theory that pain palliation may be determined by the radiosensitivity of normal bone at the leading edge of a metastasis. As the radiosensitivity of normal tissues is genetically determined, it would be logical to consider repeat treatment or dose escalation when initial therapy is unsuccessful.
The identification of biochemical markers of bone resorption and formation has provided new markers of treatment efficacy and additional insight into possible mechanisms of action of radionuclide therapy. Serum procollagen type IC terminal peptide (PICP) is a marker of bone turnover. A reduction in PICP concentration was shown to correlate with clinical response to 89SrCl2 therapy in patients with HRPC (70). In addition, the rate of production of markers of bone resorption, such as urinary pyridinium collagen cross- links, pyridinoline, and deoxypyridinoline, decreases after palliative 89SrCl2 therapy (71). More important, 89SrCl2 therapy reduces the secretion of cell adhesion molecules (E-selectins) in patients with HRPC. Cell adhesion molecule expression determines metastatic progression in a range of malignancies (72). The observation that radionuclide therapy inhibits E-selectin release suggests that the therapeutic potential of radionuclide treatment could extend beyond symptom palliation. A sustained reduction in E-selectin production might be expected to slow the rate of skeletal metastatic progression. This could be achieved by activity escalation to increase tumor dose or by fractionation.
The efficacy and toxicity of activity escalation with peripheral stem cell support has been reported: a phase 1 trial using 186Re-HEDP in 25 patients with HRPC who were administered single activities of 2.5–5 GBq followed by peripheral blood stem cell rescue at 14 d (36). The injected activity correlated with PSA response but not with hematologic toxicity, which was dependent on the whole-body absorbed dose. A multifactorial algorithm based on pretreatment biochemical and physiologic parameters was then developed and accurately predicted whole-body dose. A change of emphasis from activity escalation trials to whole-body dose-escalation studies was recommended (73). This approach would allow patient-specific activity prescription within acceptable toxicity limits. The importance of patient-specific prescribing was highlighted previously in a small series of patients receiving 153Sm-EDTMP therapy (74). The administered activity predicted to deliver a 2-Gy marrow dose varied between 35% and 63% of the 37 MBq/kg approved activity.
On current evidence, single-administration, high-activity treatment to deliver a sustained response is unlikely to be achievable within acceptable toxicity limits. Fractionated therapy may be more realistic. The short-range electron 117mSn-DTPA or α-emitting radionuclides (223Ra) are less likely to cause cumulative myelosuppression than long-range β-emitters and offer the best hope for repeated administration. It is critical that future trials be dosimetry based. Recent in vitro studies have shown that the C4–2B prostate cancer cell line exhibits osteoblast-like properties within the bone microenvironment and directly contributes to mineralized matrix formation (75). This observation suggests that single cells may be targeted using bone-seeking radiopharmaceuticals and has major implications for the future of targeted therapy. The hypothesis that high-dose therapy can target micrometastases formed the basis of activity-escalation studies using 186Re-HEDP (36). On radiobiologic grounds, the range of β-emitting radionuclides is likely to be too long for efficient energy deposition within single cells. By contrast, targeting using a bone-seeking, high-linear energy transfer α-particle emitter might be expected to achieve cell kill. The opportunity to influence skeletal tumor progression marks a significant transition from treatment delivered with palliative intent to potentially tumoricidal therapy. Further trials will be necessary to assess the value of fractionated α-particle therapy in early disease.
Several study protocols have used radionuclide therapy as an adjuvant to external-beam radiation therapy. Exposure to high-dose-rate external-beam irradiation might be expected to alter the uptake of bone-seeking radiopharmceuticals in the irradiated site, depending on the precise sequence of treatment delivery. To date, the timing of isotope administration in relation to external-beam radiation therapy has not been standardized, and the potential of response enhancement remains theoretic.
CONCLUSION
The case for radionuclide therapy within a multimodality management strategy for metastatic bone pain is strong. Response rates are consistently high, irrespective of the radiopharmaceutical prescribed and treatment is well tolerated, even in heavily pretreated patients. Further research is required to evaluate emerging treatments, examine fractionated therapy for prolonged response duration, and assess the benefits of chemoradiation. The therapeutic potential of targeted therapy will not be accepted by the wider oncology community unless studies are conducted according to internationally recognized outcome and toxicity criteria.
It is vital that future clinical trial designs incorporate prospective whole-body and tumor dosimetry. Reliance on activity-escalation studies without measuring tumor absorbed dose allows treatment to be delivered reasonably safely but prevents assessment of a dose–response relationship. The goal of patient-specific activity prescription offers the only realistic prospect of enhancing response rates within predictable toxicity limits and of progressing beyond symptom palliation to earlier intervention for survival gain.
Footnotes
Received June 15, 2004; revision accepted Nov. 17, 2004.
For correspondence or reprints contact: Val J. Lewington, BM, MSc, FRCP, Consultant Nuclear Medicine Physician, Royal Marsden Hospital, Downs Road, Sutton SM2 5PT, U.K.
E-mail: val.lewington{at}rmh.nthames.nhs.uk
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Nuts and Bolts of 223Ra-Dichloride Therapy
- Molecular radiotheragnostics in prostate cancer
- The Metastatic Spine Disease Multidisciplinary Working Group Algorithms
- Phase 2 Study of a High Dose of 186Re-HEDP for Bone Pain Palliation in Patients with Widespread Skeletal Metastases
- Therapeutic Effects of a 186Re-Complex-Conjugated Bisphosphonate for the Palliation of Metastatic Bone Pain in an Animal Model