


Abstract
The aim of this study was to determine the accuracy of 18F-FDG PET in detecting recurrent melanoma. Methods: PET findings were compared with those obtained by standard diagnostic clinical procedures (CP) to establish the role of PET in the management of patients with melanoma. From 156 patients with confirmed melanoma and recurrence suspected by clinical examination, 184 PET scans were retrospectively reviewed. Histology or clinical follow-up was used for final diagnosis. Results: The sensitivity and specificity of PET for detecting lesions on an individual-patient basis were 74% and 86%, respectively, compared with respective values of 58% and 45% for CP alone. The overall accuracy for PET was 81%, compared with 52% for other methods. PET was more accurate (91% vs. 67%) than CP in detecting locoregional disease and distant metastases (85% vs. 55%), and PET results led to a change in the planned clinical management of 36% of patients included in this study. PET was more accurate than CT in detecting skin lesions, malignant lymph nodes, and metastases to the abdomen, liver, and bone. In the assessment of pulmonary disease, PET showed higher specificity (92% vs. 70%) than CT for the detection of lung parenchyma lesions; however, the sensitivity was better for CT (93%) than for PET (57%). Conclusion: PET is better than CP in detecting locoregional disease and distant metastases in all sites except the lung, where it appears to be a useful adjunct to CT. The use of PET as a routine clinical tool can lead to a substantial change in the clinical management of suspected recurrent melanoma.
In primary cutaneous melanoma, sentinel node biopsy is an accurate method for initial staging and has become useful for the management of patients in early stages of the disease (1). Although 18F-FDG PET has been suggested as a useful alternative (2–6), the sensitivity of PET is too low to detect sentinel node metastases, which are often minimal at this stage. Therefore, preoperative lymphoscintigraphy remains the preferred method for initial regional evaluation and is routinely used to determine which nodal basins are at great risk for harboring occult metastatic disease (7–10).
The likelihood of finding regional or distant metastases in patients after successful treatment of the primary tumor is extremely low in asymptomatic patients with stage I or II disease. Many studies have reported the limited value of extensive staging work-ups, and the subsequent false-positive rate has led to unnecessary invasive procedures. Because patients with locoregional or distant metastases (stage III or IV) have a greater risk of systemic recurrence, selective imaging studies are warranted (1). Clinical examination, radiography, CT, bone scanning, MRI, ultrasound, and hepatic enzyme assays are commonly used in the follow-up of patients with melanoma or with suspected recurrence. However, the accuracy of these clinical procedures (CP) in detecting recurrent tumor is low, and on many occasions they detect locoregional or systemic spread when the disease is no longer resectable. For these reasons, an optimal method to screen for recurrent disease in earlier stages is needed to improve prognosis in these patients, especially in cases of a single metastasis that can be surgically removed to reduce the tumor load of the patient (1).
18F-FDG PET has been shown to be a useful imaging modality for several malignancies and is widely used in the staging and follow-up of several types of cancer. The obvious advantage of whole-body PET is the ability to examine the entire body with a single imaging procedure. PET has been successfully used for assessing locoregional recurrence (3,5) and occult distant metastases in patients with melanoma (11–14). However, this does not mean that PET should be used in any recurrent advanced-stage disease for which systemic palliative treatment is the only option, just to verify that even more metastases are present than suspected with other imaging tests. Reports in the literature about the value of PET in the management of patients with malignant melanoma have provided conflicting results. Some authors suggested that whole-body PET might replace staging techniques using multiple imaging modalities, such as chest radiography, ultrasound, CT, and MRI (15–18). Other series concluded that PET does not offer significant advantages over CP in detecting locoregional disease or visceral metastases (8,19,20).
The aim of this study was to determine the accuracy of whole-body PET in diagnosing recurrent malignant melanoma and to compare the results with those obtained from routine CP in order to establish the role of PET in the management of patients with melanoma.
MATERIALS AND METHODS
Patients
One hundred eighty-four PET scans from 156 patients (73 women, 83 men) with confirmed malignant melanoma (mean age, 53 ± 15 y) and suspected recurrence by clinical examination or elevated blood markers were retrospectively reviewed. Two or more PET scans were obtained for 23 patients. The clinical files were examined to ascertain the initial stage and the location of the primary tumor. Patients with other malignant tumors were excluded from this study. According to the revised version of the system established by the American Joint Committee on Cancer (21), 98 patients were stage I or II and 58 patients were stage III or IV. The primary tumor was located in the upper extremity (37 patients), lower extremity (33 patients), back (29 patients), head and neck (26 patients), thorax (8 patients), abdomen and pelvis (6 patients), ocular region (5 patients), or bowel (4 patients); in 8 patients the location of the primary tumor was unknown. The results of PET were compared with those of CP, including plain radiography, bone scanning, body CT, brain MRI, and ultrasound. Comparison was specifically between PET and body CT in 115 cases. Histology or clinical follow-up for at least 12 mo after PET was used for final diagnosis of disease recurrence. The study was approved by our Institutional Review Board.
PET Technique
The 18F-FDG PET protocol required the patients to fast for at least 4 h before the intravenous administration of 2.52 MBq of 18F-FDG per kilogram of body weight for C-PET (Philips-ADAC) studies or 5.18 MBq/kg for Allegro (Philips-ADAC) studies. Sixty minutes later, whole-body PET images were acquired in 3-dimensional mode on either the C-PET or Allegro scanner and included the neck, chest, abdomen, pelvis, and limbs. Attenuation correction was performed using a 137Cs transmission source and a nonuniform background subtraction method with scatter correction. The images were reconstructed using the 2.5-dimensional RAMLA iterative algorithm on the C-PET scanner and 3-dimensional RAMLA on the Allegro scanner.
Evaluation of PET Findings
The scans were assessed qualitatively by 2 reporters who did not then know the CP results. Areas of focal increased uptake were considered pathologic and were recorded for comparison with CP and patient follow-up results. Sensitivity, specificity, and accuracy were calculated for PET and CP evaluation on a patient basis. χ2 was calculated to compare the accuracy of PET, based on the initial stage of the primary tumor. Data are expressed as mean ± SD. A P value of <0.05 was considered statistically significant. Interobserver reliability and agreement between PET and CP were calculated using the κ-coefficient.
RESULTS
Of the 184 scans studied, 86 showed that the patient remained free of disease for at least 1 y after the scan, and 98 showed proven sites of active disease (146 lesions), which were confirmed by histologic examination or follow-up. For 47 of these 98 scans, the patients were proven to have locoregional involvement (including regional lymph nodes, in-transit metastases, and satellite lesions), and for 51 of the 98 scans (99 lesions), the patients presented with distant metastases in the lung (37 scans), liver (18 scans), bone (14 scans), lymph nodes beyond the regional nodal basins (13 scans), abdomen (10 scans), or brain (6 scans). There were no significant differences in the accuracy of PET based on the initial stage (79% in stages I and II; 85% in stages III and IV) of the primary tumor (P = 0.3). Patients in stages I and II were affected mostly by locoregional recurrence (65%), whereas patients in stages III and IV presented more frequently with distant metastases (72%).
The sensitivity and specificity of PET for detecting lesions on a patient basis were 74% and 86%, respectively, compared with respective values of 58% and 45% for CP alone. The overall accuracy for PET was 81%, compared with 52% with other methods. The agreement between PET and CP was only 49% (κ-coefficient of 0.41 ± 0.13). PET was more accurate than CP in detecting locoregional disease (91% for PET vs. 67% for CT) and distant metastases (85% for PET vs. 55% for CP). PET was not helpful in inconclusive brain MRI findings, detecting only 2 of 7 patients in whom brain metastases had developed. PET led to a change in clinical management for 36% of patients included in this study. PET findings were negative for 17 locoregional recurrences and 55 metastases suspected by CP, allowing us to discard those CP findings. In addition, PET findings led to curative resection of 14 locoregional recurrences and 10 distant metastases (6 in lymph nodes, 2 in the liver, 1 in the lung, and in the 1 small bowel). In 12 patients, PET led to systemic chemotherapy instead of inadequate surgery. Lower-limb imaging was helpful in 4 cases in which lower-limb lesions were the only lesions found: 3 cases of locoregional recurrence in the lower limbs (2 in the knee and 1 in the ankle) and 1 case of infiltrated metastatic lymph nodes in the popliteal basin.
PET and body CT were compared in 115 patients (Table 1). PET was more accurate than CT in detecting skin lesions and lymph node, abdomen, liver, and bone metastases (Fig. 1). At 83% for PET and 77% for CT, the accuracy of PET for lung parenchyma lesions was similar for both techniques (Fig. 2). However, in assessing pulmonary metastases, PET showed higher specificity (92%) than did chest CT (70%), whereas the sensitivity was higher for CT (93%) than for PET (57%). We found solitary lung lesions in 8 of 12 patients for whom PET was negative for lung involvement and who could have benefited from surgical removal of the lesion. On the other hand, for 5 of 8 solitary lung lesions, PET showed metastatic lesions in other locations, making curative therapy unfeasible. The standardized uptake value, being >3 for all false-positive readings, did not improve the specificity of PET readings. The interobserver reliability κ-coefficient was 0.87.
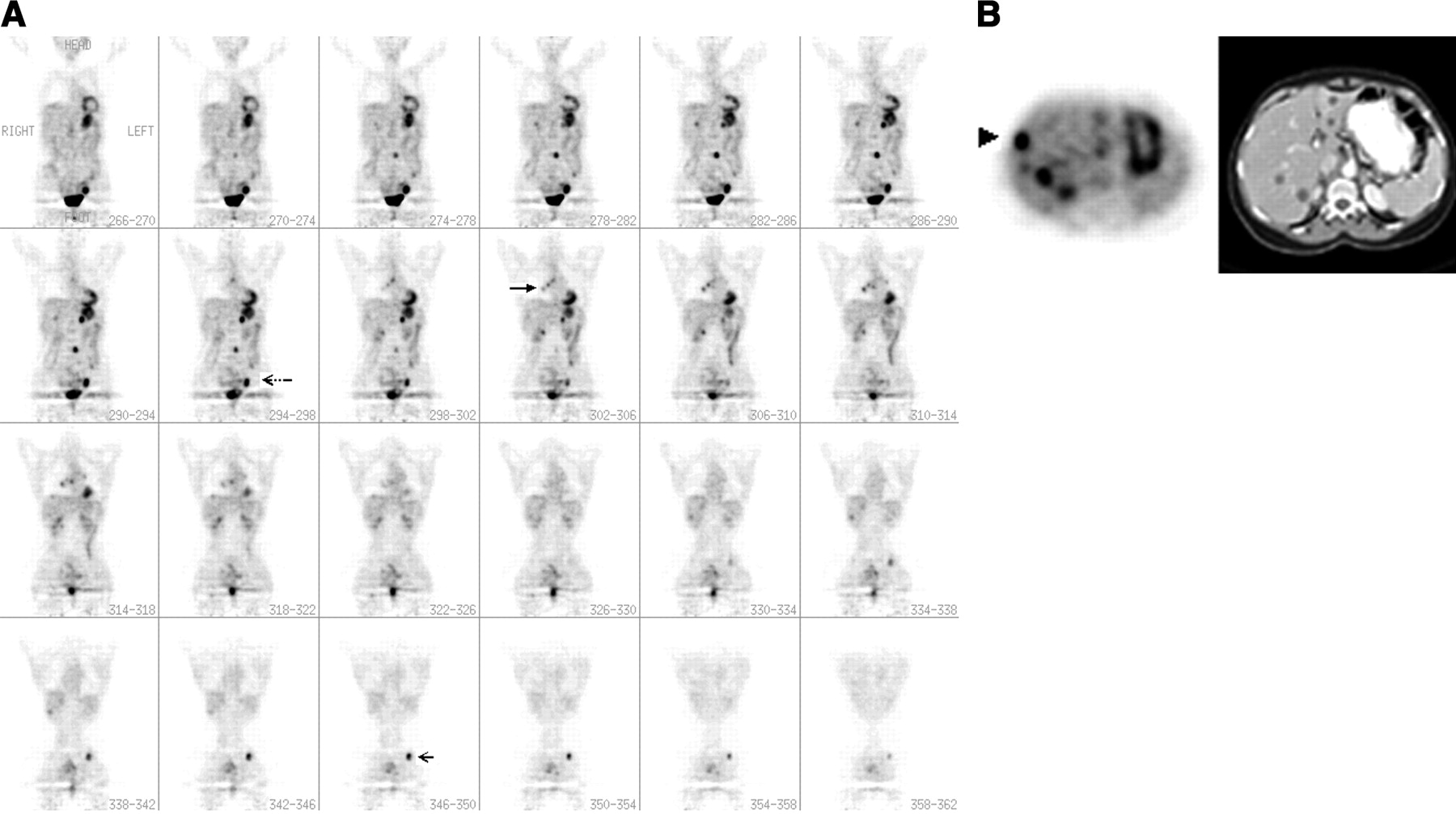
(A) Whole-body PET scan of a patient with a recently removed stage II melanoma of the right arm shows several lesions in the right hilum (large arrow), the liver, the left groin (dotted arrow), the lumbar spine, and the left ischium (small arrow). (B) CT of the chest, abdomen, and pelvis was able to identify only the liver metastases (right panel); PET showed the same lesions in the liver but detected an additional focus in the anterior right liver (arrowhead, left panel). The diagnosis of metastatic spread was further established by follow-up of the patient.
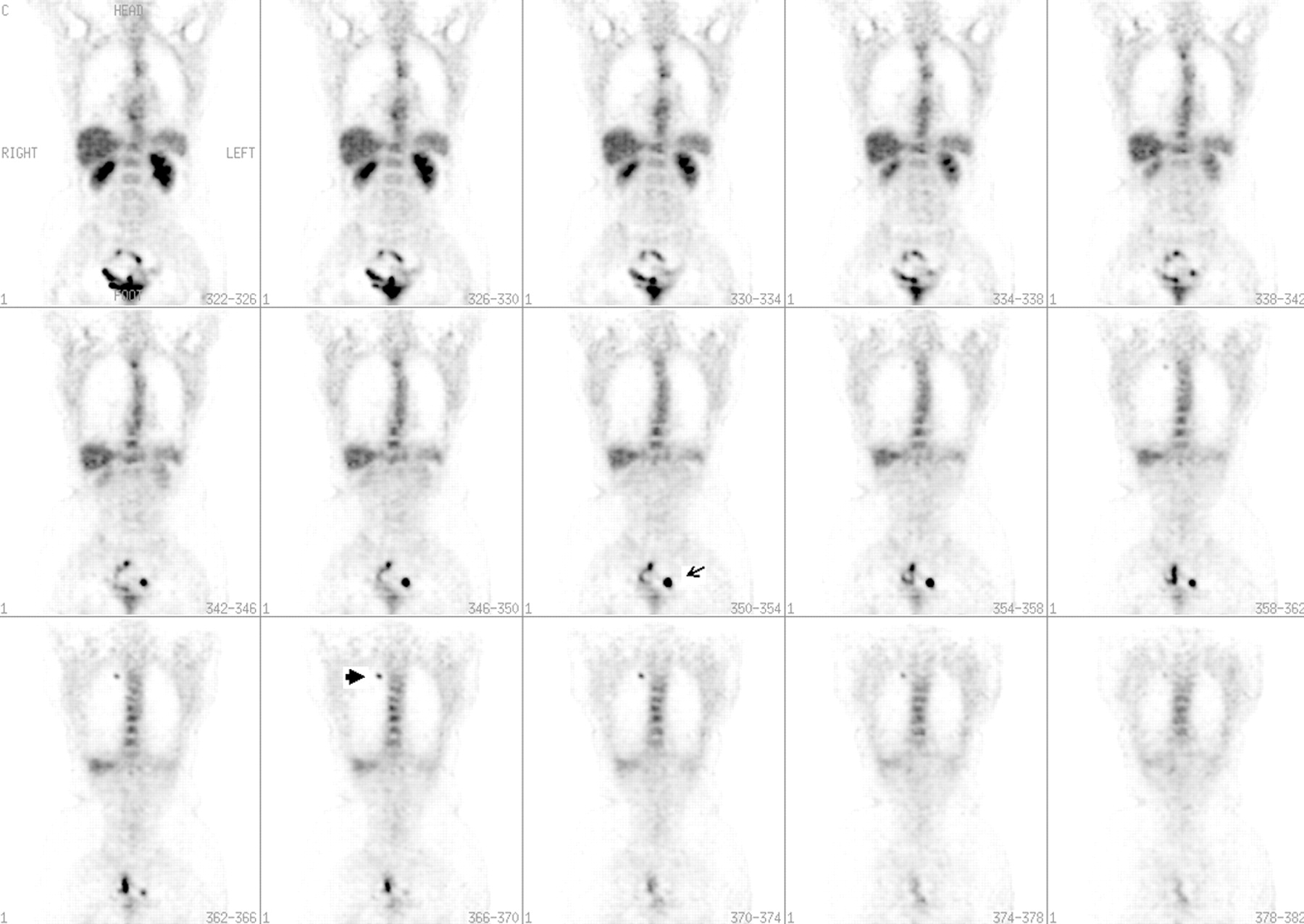
Whole-body PET scan shows focal uptake in the apex of the right lung, in the same location as a 2-cm lesion observed on a prior chest CT scan (large arrow). PET also detected several lesions that extended to the midline in the left pelvis and were not found by other CPs (small arrow). These lesions were histologically confirmed to be lymph node metastases.
A Comparison of PET and Body CT Results in the Detection of Active Melanoma in 115 Patients
DISCUSSION
Clinical data show that lymphoscintigraphy associated with intraoperative γ-probe detection of the sentinel node improves the accuracy of diagnosing lymph node involvement in patients with an initial diagnosis of melanoma (2). Some authors have suggested sentinel lymph node scanning and PET to be complementary (20,22). However, the role of lymphoscintigraphy in suspected recurrent melanoma is not yet established, and studies must be performed to determine its usefulness in clinical management. PET is a noninvasive technique that can be applied at any stage of disease. In this study, we found PET to be highly accurate (91%) for diagnosing locoregional involvement, compared with CP (67%). Though we did not directly compare PET with sentinel lymph node scanning, our results suggest that PET may have a role as a staging procedure, especially in patients with high-risk melanoma, for which distant spread of disease needs to be ruled out. The combination of the relatively large population of melanoma patients who are at risk for disease recurrence, and the fact that melanoma may metastasize to anywhere in the body, implies that evidence-based strategies are required to accurately survey these patients after primary treatment (23).
The sensitivity and specificity of PET for diagnosing recurrent and metastatic melanoma on a patient basis were 74% and 86%, respectively. The values obtained with PET were significantly higher those obtained with CP, which had a sensitivity of only 58% and a specificity of only 45%. The overall accuracy of PET was 81%, compared with only 52% for other methods. Brain was included in the PET examination only when anatomic imaging was nonconclusive, but PET did not add significant information. Brain metastases are difficult to distinguish from background activity because of the high rate of glucose metabolism in normal gray matter. On the other hand, we recommend lower-limb imaging because our results showed that it may help in diagnosing unsuspected locoregional recurrences or infiltrated metastatic lymph nodes.
Taking into account that metabolically active processes may show nonspecific 18F-FDG uptake, one concern was that PET findings could be confounded with uptake in benign processes or nonmelanoma tumors. The inflammatory changes detected by PET in this series were usually mild and diffuse, and except for 8 patients with false-positive findings, all instances were explained by clinical data, resulting in an overall specificity of 91%, compared with 44% for CP.
PET was more accurate than CT in detecting lymph node metastases and had a higher specificity (88%) than did CT (56%). PET was superior to CT in diagnosing spread to the liver, detecting 85% of the lesions and producing no false-positive findings. CT showed a lower sensitivity, 77%, and produced 17 cases of false-positive findings. In the abdomen, CT was less accurate (82%) than PET (96%) for diagnosis of disease, but it also produced 14 cases of false-positive findings, compared with only 2 for PET. PET and CT showed comparable accuracies for detecting metastatic lesions in the lung parenchyma, but the sensitivity of chest CT was higher (93%) than that of PET (57%). These results agree with those reported in the literature (16) and may be due to the difficulty for PET of detecting small, subcentimeter, nodules in the lungs. However, the PET scan showed 5 of 8 solitary lung lesions to have metastases to other locations, making curative surgery unfeasible. Because many of these nodules are incidental findings and may represent benign processes, CT specificity tends to be low, as was observed in this study, in which PET was shown to be more specific (92%) than CT (70%).
Our data clearly reveal that the use of PET as a whole-body screening test can rule out recurrent melanoma and may affect the outcome of these patients. PET is able to detect recurrent disease before symptoms appear or structural changes are evident on anatomic imaging. As with other series (15,17,24–25), PET changed the clinical management of a substantial number of the patients in our study (36%). In our series, the use of PET saved unneeded invasive procedures, as it excluded 17 locoregional recurrences and 55 metastases wrongly suspected by CP findings. Moreover, PET led to curative resection of 14 locoregional lesions and 10 distant metastases unsuspected by other procedures. Although no evidence suggests that earlier detection of occult melanoma metastases can improve survival (26), several reports have shown prolonged survival in selected patients whose distant melanoma metastases were limited and resectable at the time of diagnosis (27,28). On the basis of our analysis, we would recommend the use of PET when recurrence is suspected by clinical examination or when laboratory tumor markers are elevated.
CONCLUSION
Whole-body PET is a useful tool in the diagnosis of recurrent melanoma. PET is better than CP in detecting locoregional disease and distant metastases at all sites except the lung, where it appears to be a useful adjunct to CT. The use of PET as a routine clinical tool can lead to substantial change in the clinical management of suspected recurrent melanoma.
Footnotes
Received Nov. 20, 2003; revision accepted Mar. 2, 2004.
For correspondence or reprints contact: Abass Alavi, MD, Division of Nuclear Medicine, University of Pennsylvania, 110 Donner Building, 3400 Spruce St., Philadelphia, PA 19104.
E-mail: alavi{at}rad.upenn.edu
REFERENCES





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Nuclear Medicine and Molecular Imaging in Nodal Staging and Surveillance of Ocular Melanoma: Case Reports and Review of the Literature
- Prospective Comparison of [18F]Fluorodeoxyglucose Positron Emission Tomography and Computed Tomography in Patients With Melanoma With Palpable Lymph Node Metastases: Diagnostic Accuracy and Impact on Treatment
- Role of Modern Imaging Techniques for Diagnosis of Infection in the Era of 18F-Fluorodeoxyglucose Positron Emission Tomography
- Role of Nuclear Medicine in the Management of Cutaneous Malignant Melanoma
- Diagnostic Performance of Whole Body Dual Modality 18F-FDG PET/CT Imaging for N- and M-Staging of Malignant Melanoma: Experience With 250 Consecutive Patients