


Abstract
The feasibility of 18F-3′-fluoro-3′-deoxy-l-thymidine PET (FLT PET) for detecting laryngeal cancer was investigated and compared with 18F-FDG PET. Methods: Eleven patients diagnosed with or strongly suspected of having recurrent laryngeal cancer and 10 patients with histologically proven primary laryngeal cancer underwent attenuation-corrected 18F-FLT PET imaging 60 min after injection of a median of 213 MBq (range, 175–400 MBq) 18F-FLT and attenuation-corrected 18F-FDG PET imaging 90 min after injection of a median of 340 MBq (range, 165–650 MBq) 18F-FDG. All patients were staged by endoscopy and CT according to the Union Internationale Contre la Cancer TNM staging system. All patients underwent biopsy of the laryngeal area after imaging. Lesions seen on 18F-FDG PET and 18F-FLT PET were compared with histopathologic results. Mean SUVs, maximum SUVs, and tumor-to-nontumor (TNT) ratios were calculated for 18F-FLT and 18F-FDG. Wilcoxon nonparametric testing was used for comparison of 18F-FDG with 18F-FLT uptake. The Spearman correlation coefficient was used to correlate mean SUVs, maximum SUVs, and TNT ratios of 18F-FDG PET and 18F-FLT PET. Two-tailed P values < 0.05 were considered significant. Results: 18F-FDG PET and 18F-FLT PET detected laryngeal cancer correctly in 15 of 17 patients. One lesion judged as positive on 18F-FDG PET turned out to be normal tissue. Of 2 lesions judged as positive on 18F-FLT PET, 1 turned out to be inflammation and the other to be normal tissue. Maximum SUVs were 3.3 (range, 1.9–8.5) for 18F-FDG and 1.6 (range, 1.0–5.7) for 18F-FLT (P < 0.001). Mean SUVs were 2.7 (range, 1.5–6.5) for 18F-FDG and 1.2 (range, 0.8–3.8) for 18F-FLT (P < 0.001). TNT was 1.9 (range, 1.3–4.7) for 18F-FDG and 1.5 (range, 1.1–3.5) for 18F-FLT (P < 0.05). Conclusion: The numbers of laryngeal cancers detected with 18F-FLT PET and 18F-FDG PET were equal. In laryngeal cancer, the uptake of 18F-FDG is higher than that of 18F-FLT.
The current standard for staging of laryngeal cancer is direct laryngoscopy complemented by histologic biopsy and CT or MRI (1,2). The detection of tumors and metastatic lymph nodes by CT and MRI is solely dependent on changes in tissue structure and size of lymph nodes (2). Therefore, nonenlarged metastatic nodes and primary or recurrent tumors that do not distort tissue structures can be missed. In addition, tissue changes caused by radiation therapy can also complicate the interpretation of CT and MR images. Despite the fact that biopsy is the gold standard, locating the possible site of recurrence for biopsy is still difficult, because most recurrent head and neck cancers are located in the submucosa (1). Moreover, the surgeon will be reluctant to obtain multiple blind biopsies, because these could initiate or aggravate radionecrosis (2).
18F-FDG PET is accepted as a powerful, noninvasive metabolic imaging method for the diagnosis and staging of cancer (3–5). 18F-FDG PET has been introduced as a noninvasive diagnostic tool in head and neck cancer, where it is especially accurate in detection and in providing prognostic information (6–8). However, experience with 18F-FDG PET solely in patients with laryngeal cancer is limited. 18F-FDG PET has proven in a few studies to be valuable in distinguishing between benign and malignant tissue changes after radiation therapy in patients with suspected recurrent laryngeal cancer (9–11). Even fewer data are available on 18F-FDG PET in patients with untreated primary laryngeal cancer (9,12).
Because 18F-FDG is also metabolized in nontumor tissue, results may be false-positive in inflammation, reactive tissue, or supraclavicular fat (13–15). In addition, muscle uptake of 18F-FDG may interfere with PET interpretation. Moreover, the interval between radiation therapy and 18F-FDG PET imaging is important for accurate diagnosis (1,9,16).
Recently, Shields et al. (17) introduced 18F-3′-fluoro-3′-deoxy-l-thymidine (18F-FLT) as a PET tracer that might not have these drawbacks (18). This pyrimidine analog is phosphorylated by the enzyme thymidine kinase 1 (TK1), which leads to intracellular trapping (17). During DNA synthesis, TK1 activity increases almost tenfold and is thus an accurate reflection of cellular proliferation (19). 18F-FLT uptake is probably related to TK1 activity and, therefore, also related to proliferation. The aim of this study was to investigate the feasibility of 18F-FLT PET in comparison with 18F-FDG PET for detection of primary and recurrent laryngeal cancer. A second aim was to investigate possible differences in uptake of 18F-FLT and 18F-FDG in malignant and normal tissue.
MATERIALS AND METHODS
Patients
This prospective study included 21 consecutive patients: 11 with suspected recurrent laryngeal cancer and 10 with primary laryngeal cancer. Informed consent was obtained. Patients were enrolled from September 2001 through March 2003.
The patients with suspected recurrent laryngeal cancer had been treated initially with radiation therapy for laryngeal squamous cell carcinoma. Recurrent disease was suspected in these patients, because increased hoarseness, edema, pain in the larynx, or referred pain developed. All patients with suspected recurrent laryngeal cancer underwent diagnostic laryngoscopy for biopsy. The patients with primary laryngeal squamous cell carcinoma were candidates for radiation therapy. The disease of all patients had been clinically staged according to the Union Internationale Contre la Cancer TNM classification (20).
All patients underwent physical examination of the head and neck, chest radiography, endoscopic examination under general anesthesia, biopsies of suspected areas, and spiral CT of the neck. For inclusion, liver and kidney functions and hematologic parameters (hemoglobin, hematocrit, erythrocytes, thrombocytes, leukocytes, and white cell count) had to be within normal limits. Pregnant patients and patients with psychiatric disorders were excluded. All screened patients were included in the study. The medical ethics committee of the Groningen University Hospital approved the study protocol.
Tracer Synthesis
Synthesis of 18F-FLT was performed according to the method of Machulla et al. (21). 18F-FLT was produced by 18F fluorination of the 4,4′-dimethoxytrityl-protected anhydrothymidine, followed by a deprotection step. After purification by reversed-phase high-performance liquid chromatography, the product was made isotonic and passed through a 0.22-μm filter. 18F-FLT was produced with a radiochemical purity of >95% and specific activity of >10 TBq/mmol. The radiochemical yield was 7.5% ± 5.1% (at end of bombardment).
Synthesis of 18F-FDG was performed according to the method of Hamacher et al. (22) by an automated synthesis module. The radiochemical yield was 65.9% ± 7.1% (at end of bombardment).
PET Scanning
All studies were performed using an ECAT EXACT HR+ (Siemens/CTI Inc.). Before PET imaging, patients were instructed to fast for at least 6 h. They were also instructed to drink 1 L of water before imaging to stimulate 18F-FLT and 18F-FDG excretion from the renal calyces and subsequent voiding.
For injection of the radiopharmaceuticals, a venous cannula was inserted in each patient’s forearm. The interval between the 18F-FDG PET and 18F-FLT PET imaging was a maximum of 16 d. All patients were scanned in 4 positions from the nose down in emission–transmission–transmission–emission mode, with 3 and 5 min per bed position for transmission and emission scanning, respectively. Twenty-one patients (20 men, 1 woman) with a median age of 65 y (range, 50–91 y) were included in this study (Table 1). Patients received a median of 340 MBq (range, 165–650 MBq) 18F-FDG and a median of 213 MBq (range, 175–400 MBq) 18F-FLT. Patients were scanned 60 min after 18F-FLT injection and 90 min after 18F-FDG injection. Previous experience with 18F-FLT indicated that tumor-to-nontumor (TNT) ratios were constant from 60 min after injection of the tracer. PET images were iteratively reconstructed (ordered-subset expectation maximization) (23).
Patient Characteristics
Pathologic Evaluation
Biopsies of the laryngeal area and surgical specimens of total laryngectomies were examined on hematoxylin-and-eosin–stained sections. The pathologist was unaware of the results of the PET images. In patients in whom a total laryngectomy was performed, the maximum tumor diameter was obtained (Table 1). In the remaining patients only biopsies were performed, and these were used for histologic investigation.
Data Analysis
18F-FLT PET and 18F-FDG PET images were analyzed for uptake in malignant lesions and normal anatomic structures. A physician experienced with PET evaluated the images aware only of the location of the primary or suspected lesion and unaware of other clinical information.
18F-FLT PET and 18F-FDG PET images were first interpreted visually. The presence of a hypermetabolic lesion was judged as positive, and the absence of a hypermetabolic lesion was judged as negative. After visual interpretation, both the 18F-FLT PET and 18F-FDG PET images were analyzed randomly for hypo- and hypermetabolic lesions and sagittal sections. The slice with the highest uptake was selected for region-of-interest (ROI) analysis. After selecting the plane with the maximum SUV, an ROI was drawn manually. ROIs were placed at the 70% contour of the maximal SUV in the tumor when possible. In other cases, ROIs were drawn manually. The same ROI method was applied on the same slice in normal laryngeal tissue above or below the tumor site to calculate the background SUV. The mean SUV of the tumor was divided by the mean SUV of the background region to produce the TNT ratio. The TNT ratios and SUVs of 18F-FLT PET and 18F-FDG PET were compared. Images were displayed on a SUN workstation (Sun Microsystems). ROI calculation was performed using Clinical Applications Programming Package version 5 (CTI, Inc.).
Statistical Analysis
The results of the visually interpreted PET images were compared with the histologic data, which were used as standard. The Wilcoxon signed rank test was used to compare the mean SUVs, maximum SUVs, and TNT ratios of 18F-FDG PET and 18F-FLT PET. The Spearman correlation coefficient was used to correlate the mean SUVs, maximum SUVs, and TNTs of 18F-FDG PET and 18F-FLT PET. Two-tailed P values < 0.05 were considered significant.
RESULTS
Patients
Fifteen patients underwent biopsy of the laryngeal area after PET scans in the Groningen University Hospital. However, patients 7, 8, 11, 12, 15, and 20 underwent a biopsy in a referring hospital. These biopsies were performed at 7 mo and 17, 11, 27, 42, and 21 d, respectively, before the PET scans.
Visualization of Laryngeal Cancer
In patients 2, 11, 14, and 19, no uptake of 18F-FLT or 18F-FDG could be observed, and, therefore, no SUV could be calculated. Histopathologic investigation showed no malignancy in patients 2 and 11. However, in patients 14 and 19 histopathologic investigation showed 2 recurrent laryngeal cancers.
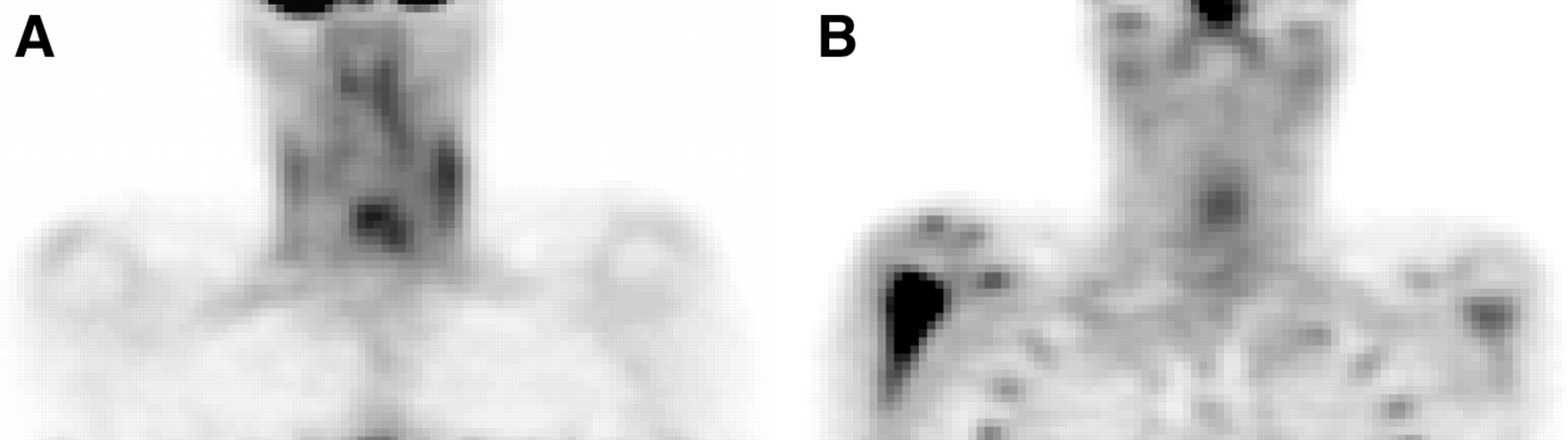
18F-FDG PET and 18F-FLT PET detected 15 of 17 laryngeal cancers. One lesion (in patient 10) judged as positive on 18F-FDG PET was found to be normal tissue. 18F-FLT PET and 18F-FDG PET missed 2 T1 tumors in patients 14 and 19. Two lesions (in patients 3 and 10) judged as positive on 18F-FLT PET were found to be inflammation in one patient and normal tissue in the other. Figure 1 shows an 18F-FDG image and an 18F-FLT PET image of a patient with primary laryngeal cancer.

Coronal 18F-FDG PET (A) and 18F-FLT PET (B) images of patient 3, diagnosed with primary laryngeal cancer. With both imaging modalities, uptake of the tracer in the laryngeal region can be observed. Maximum 18F-FDG SUV was 3.2, and maximum 18F-FLT SUV was 1.2. Physiologic 18F-FDG uptake can be seen in the muscles of the neck, and physiologic 18F-FLT uptake can be seen in the bone marrow of the ribs and sternum.
Comparison Between 18F-FDG and 18F-FLT Uptake
The uptake of 18F-FDG was significantly higher than that of 18F-FLT, whether expressed in mean SUV, maximum SUV, or TNT ratio (Table 2). The correlations between mean SUVs, maximum SUVs, and TNT ratios of 18F-FDG and 18F-FLT varied between 0.613 and 0.705 and were significant (P < 0.05).
Wilcoxon Nonparametric Test
DISCUSSION
This study was conducted on 21 patients and showed that both 18F-FDG PET and 18F-FLT PET could detect 15 of 17 laryngeal cancers. In 4 patients, lesions suggestive of laryngeal cancer turned out to be normal or inflammatory laryngeal tissue. 18F-FDG PET detected 1 of these lesions as positive, and 18F-FLT PET detected 2 of these lesions as positive. The uptake of 18F-FDG (mean SUV of 2.7 [range, 1.5–6.5]) in laryngeal cancer was significantly higher than that of 18F-FLT (mean SUV of 1.2 [range, 0.8–3.8]).
Although few data are available, the limited 18F-FDG PET data on sensitivity in this study are in the same range as 18F-FDG PET data in the literature, where sensitivity for the detection of laryngeal cancer ranged from 80% to 97% (9,11,12,16,24,25) and specificity ranged from 61% to 82% (10,11,16). The specificity obtained in this study for 18F-FDG PET (100%, 3 of 3) is less reliable and not comparable with the literature because of the low number of false-positive and true-negative lesions.
False-positive results with 18F-FDG PET do occur, because 18F-FDG is also trapped in normal tissue. Secretion of 18F-FDG in normal mucosa and saliva and pooling of saliva in the larynx may cause increased uptake in the laryngeal area (13). Increased uptake is also found in salivary glands, tonsil tissue, muscle tissue of the larynx and the neck, benign laryngeal papilloma, and the base of the tongue (15). Moreover, wound healing after biopsy, local inflammation such as osteomyelitis or cellulitis, or a polyp may cause increased local 18F-FDG uptake (9,10,13,26). Furthermore, the interval between radiation therapy and the 18F-FDG PET is important for accurate diagnosis (9,10,16,27).
As an alternative to 18F-FDG, tracers have been developed that are potentially more specific and that take part in other metabolic processes. Several amino acids that image protein synthesis have been developed as tracers. Most of these studies have been performed with l-[methyl-11C-]-methionine (MET). The disadvantage of MET is substantial accumulation of non–protein-related metabolites in tumor tissue (28). l-[1-11C]-tyrosine (TYR) also has been used to detect tumors and determine protein metabolism. In laryngeal and hypopharyngeal cancer, TYR was able to detect all primary tumors, with a correlation between protein synthesis rate and SUV (29–31). However, the disadvantage of this tracer is the low tumor uptake and accumulation in salivary glands, which could impair detection of metastatic lymph nodes in head and neck cancer (28,29). In 1998, Shields et al. (17) developed 18F-FLT, a pyrimidine analog that indirectly measures DNA synthesis through the DNA salvage pathway. Recent articles about 18F-FLT PET focused on the detection of colorectal and lung cancer and their metastases (32,33). A correlation was found between SUV and proliferation in single pulmonary nodules (32,34,35).
Despite the promising properties of 18F-FLT, 18F-FLT PET barely detected a recurrent laryngeal tumor (in patient 3) that displayed avid uptake of 18F-FDG. The tumor was large (1.8 mm), poorly differentiated, and surrounded with ulcers. This could explain the low 18F-FLT uptake and avid 18F-FDG uptake in the surrounding inflammation. 18F-FLT PET and 18F-FDG PET missed 2 T1 tumors that were detected on CT. The size of these tumors could be below the detection level of PET, and a partial-volume effect could be involved. In the literature, 18F-FDG PET has been reported to miss T1–T4 laryngeal tumors as well. However, no histologic explanation is given for these false-negative findings (11,24,25). Unfortunately, it is impossible to accurately quantify or assess the size of a primary laryngeal cancer. This is because diagnosis and extent of the tumor are obtained by a laryngoscopically guided biopsy and CT, because almost all T1–T3 tumors are treated with radiation therapy. The size of the biopsy obtained from the tumor is often too small to obtain reliable Ki-67 data for correlation with 18F-FLT uptake. In contrast, it is possible to obtain reliable Ki-67 data in patients with T4 tumors, who undergo total laryngectomy and are not palliatively treated with radiation therapy. In these patients, the tumor can be fully examined histologically. However, a T4 tumor often causes acute respiratory distress leading to acute laryngectomy, making a PET scan unethical and impossible.
Malignant tissue displayed a significantly higher uptake of 18F-FDG than 18F-FLT. The mean 18F-FDG SUV reported in the literature for patients with primary or recurrent laryngeal cancer ranges from 4.6 to 10.7 (9,12,13). These values are higher than the maximum 18F-FDG SUV of 3.3 (range, 1.9–8.5) and mean 18F-FDG SUV 2.7 (range, 1.5–6.5) in this study. No literature is available on 18F-FLT PET for detecting laryngeal cancer. However, the SUVs of 18F-FDG PET and 18F-FLT PET in patients with colorectal or lung cancer have been compared in the literature (32,33). The mean 18F-FLT PET SUV in colorectal cancer was 4.2, compared with a mean 18F-FDG PET SUV of 8.7. The 18F-FLT SUV in lung cancer ranged from 1.2 to 3.1, and the 18F-FDG PET SUV ranged from 1.7 to 8.9. Although these articles discuss different types of malignancies, they also reported significantly lower uptake of 18F-FLT than 18F-FDG, just as was found for the detection of laryngeal cancer in this study (32,33). The lower level of uptake probably raises the detection limit.
The correlation between 18F-FDG and 18F-FLT uptake was not strong. The SUV is the net result of several uptake processes. The availability of the tracer in the blood pool, nonspecific uptake, perfusion of the tumor, membrane transport, metabolic processes in which the tracer is involved, and (ir)reversible trapping of the tracer flow over the membrane are factors that can influence the SUV. It is our impression that both 18F-FLT and 18F-FDG are taken up by malignant cells but that the demand for glucose is larger than that for thymidine. The phosphorylation rate in vitro is about 30% of the phosphorylation rate of serum thymidine by TK1, which could be an explanation for a low 18F-FLT uptake in the tumor (36,37).
The number of patients in this study was too small to draw conclusions about the accuracy of 18F-FDG PET and 18F-FLT PET for detection of laryngeal cancer in general and for detection of primary or recurrent laryngeal cancer specifically. Larger groups of patients are needed with at least 2 observers to calculate the interobserver agreement to more accurately reflect clinical reality.
Future roles for 18F-FDG PET and 18F-FLT PET in laryngeal cancer are only partly clear. The role for 18F-FDG PET in detecting laryngeal cancer seems to be in differentiating between tumor and nontumor tissue in patients with suspected recurrent laryngeal cancer (1,9–11,13). It is reasonable to delay biopsy on a negative 18F-FDG PET assessment and prevent unnecessary biopsies that could initiate or aggravate radionecrosis (1,10,11). Imaging with PET lacks anatomic detail, but this could be overcome by the use of PET/CT. Too few data are available for the detection of primary laryngeal cancer untreated by radiation therapy (9,24,25). Further research is needed to investigate whether 18F-FDG PET is an adequate tracer for the detection of primary laryngeal cancer. Because of the low uptake of 18F-FLT, 18F-FLT PET seems less adequate for the detection of laryngeal cancer (11).
The numbers of laryngeal cancers detected with 18F-FLT PET and 18F-FDG PET were equal. The uptake of 18F-FDG in laryngeal cancer was higher than that of 18F-FLT.
Acknowledgments
This research was funded by the Dutch Cancer Foundation (grant 2000-2299).
Footnotes
Received Jul. 9, 2003; revision accepted Sep. 22, 2003.
For correspondence or reprints contact: David C.P. Cobben, MD, PET Center, Groningen University Hospital, P.O. Box 30.001, Groningen, The Netherlands 9700 RB.
E-mail: D.C.P.Cobben{at}pet.azg.nl
REFERENCES
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- 18F-FLT PET During Radiotherapy or Chemoradiotherapy in Head and Neck Squamous Cell Carcinoma Is an Early Predictor of Outcome
- PET Imaging During Radiotherapy of Head and Neck Cancer
- Biologic Imaging of Head and Neck Cancer: The Present and the Future
- Histopathologic Validation of 3'-Deoxy-3'-18F-Fluorothymidine PET in Squamous Cell Carcinoma of the Oral Cavity
- Innovations in Radiotherapy Planning of Head and Neck Cancers: Role of PET
- 18F-FDG and 18F-FLT Uptake Early After Cyclophosphamide and mTOR Inhibition in an Experimental Lymphoma Model
- Kinetic Analysis of 3'-Deoxy-3'-18F-Fluorothymidine (18F-FLT) in Head and Neck Cancer Patients Before and Early After Initiation of Chemoradiation Therapy
- Gene Expression Patterns and Tumor Uptake of 18F-FDG, 18F-FLT, and 18F-FEC in PET/MRI of an Orthotopic Mouse Xenotransplantation Model of Pancreatic Cancer
- Imaging of Cell Proliferation: Status and Prospects
- 18F-FLT PET Does Not Discriminate Between Reactive and Metastatic Lymph Nodes in Primary Head and Neck Cancer Patients
- Future Issues in Highly Conformal Radiotherapy for Head and Neck Cancer
- 18F-FLT PET in Hematologic Disorders: A Novel Technique to Analyze the Bone Marrow Compartment
- Imaging Proliferation in Brain Tumors with 18F-FLT PET: Comparison with 18F-FDG
- Comparison of 18F-FLT PET and 18F-FDG PET in Esophageal Cancer
- Kinetic Analysis of 3'-Deoxy-3'-Fluorothymidine PET Studies: Validation Studies in Patients with Lung Cancer