


Abstract
In the past decade, the integration of anatomic imaging and functional imaging has emerged as a new and promising diagnostic tool. Developments in software provided methods to integrate various modalities, such as PET, CT, MRI, and MR spectroscopy. The introduction of combined PET/CT scanners has boosted image fusion in this specific field and raised high expectations. Image fusion can be performed at 3 different levels: visual fusion, software fusion, and hardware fusion, each having strengths, weaknesses, and issues inherent to technique. Visual fusion is the traditional side-by-side reviewing of 2 separate modalities. Software image fusion provides evaluation of 2 modalities in 1 integrated image set. True hardware fusion of PET and CT does not exist at present. Currently, hardware fusion refers to a PET/CT scanner that consists of separate scanners, which positioned in line at a fixed distance, with projection of the PET image over the CT image. The suggested superiority of hardware fusion with these so-called hybrid PET/CT scanners over software fusion has sparked debate. Because scientific data that unequivocally show that state-of-the-art software fusion is less accurate than hardware fusion (as provided in hybrid PET/CT scanners) are unavailable, the primacy of a combined PET/CT scanner over stand-alone PET and CT is more a matter of belief than of science. Further research comparing the overall performance of PET/CT scanners with that of separate scanners with software for image fusion is much needed. The continuous development of better software for image fusion and respiratory and cardiac gating is also needed, not only for PET and CT imaging but also for fusion of PET with MRI and CT with MRI.
In the past decade, functional imaging with 18F-FDG PET has been the fastest growing diagnostic modality in oncology. The high sensitivity for depicting increased metabolism in a wide variety of malignancies adds significant accuracy to many diagnostic regimens compared with anatomic imaging only (CT, MRI, ultrasound). For several reasons, anatomic and functional imaging has been integrated into one diagnostic modality that is known as image fusion.
Image fusion can be performed at 3 different levels: visual fusion, software fusion, and hardware fusion. In traditional visual image fusion, the physician compares 2 separate imaging modalities viewed next to each other. The fusion takes place in his or her mind. In soft- and hardware image fusion, the results of both procedures are overlaid in an integrated set of images. It is the suggested superiority of hardware fusion in hybrid PET/CT scanners over software fusion that has sparked current discussions.
Software for image fusion has been developed by various vendors and is universally applicable to all sorts of image sets. True hardware fusion of PET and CT does not exist at present. It would require the use of a single detector system that registers 2 image sets at the same time (e.g., 511-keV γ-rays from 18F-FDG and x-rays from CT). An alternative solution is a combined device with separate CT and PET scanners positioned in line. Several companies adopted this principle, and so-called hybrid PET/CT scanners are now widely available commercially.
Although hybrid PET/CT scanners are advertised extensively as the latest achievement in modern technology and as “state-of-the-art” and “must-haves,” independent research on real benefits has just begun. At this moment, few objective results have been produced that show the necessity of a combined PET/CT scanner or its advantages over software fusion. The current debate is mainly led by commercial companies and individual physicians’ expert opinions. Therefore, comments and concerns are justified.
Objective and independent grounds and arguments are discussed here, both for and against the use of image fusion in the modern daily clinical practice of diagnostic imaging and including both soft- and hardware fusion.
DIAGNOSTIC MODALITIES
Anatomic Imaging
Imaging modalities such as CT and ultrasound adequately reflect normal anatomy and anatomic changes. MRI has similar or even better potential for depicting anatomy and also provides additional tools for functional imaging. In recent years, the spatial resolution of these techniques has improved greatly, now significantly <1 mm. This permits accurate recognition and delineation of organs and structures, especially with the use of contrast-enhancing agents. These procedures are widely available and hold a solid position in the diagnostic algorithm of many disease entities. Despite these advances, anatomic imaging may be unable to differentiate between normal and pathologic tissues with similar densities. It provides relatively little information about the viability or metabolic activity of organs and lesions, thus lacking sufficient sensitivity and specificity to answer a number of important clinical questions. Well-known examples are the differentiation of viable tumor from scar tissue after external beam radiation or chemotherapy, the detection of isodense metastases in the liver (in particular in a deformed liver after surgical procedures or in liver cirrhosis), and the detection of metastases in normal-size lymph nodes.
Functional Imaging
Functional imaging with 18F-FDG PET scanning permits the differentiation of viable malignant tissue or active infection from normal tissue and from nonviable remnants by direct visualization of metabolic activity in vivo. Other tracers currently under development may prove useful in visualizing other important parameters, such as DNA synthesis, mitotic activity, protein synthesis, local ischemia, and expression of tumor-specific receptors. Despite high contrast resolution, the major drawbacks of PET scanning are the relatively low spatial resolution of images (at present in the range of 4–6 mm and physically limited to about 2 mm) and poor recognition and delineation of anatomic structures. This may result in uncertainty or even failure in correctly localizing detected abnormalities. Recognized examples are lesions in the upper abdomen, situated near the border of organs, or between adjacent organs.
Advanced MR techniques such as dynamic MRI and MR spectroscopy (MRS) are now available. These techniques also show functional aspects, such as vascularity, blood perfusion, oxygenation, and biochemical information. Moreover, MR contrast agents have been developed to label specific tissues. For example, ultrasmall superparamagnetic iron oxide particles specifically visualize macrophages and enable the differentiation of normal lymph node tissue from metastases (1).
BENEFITS OF IMAGE FUSION
The limitations in separate CT and PET imaging may be compensated for when the 2 modalities are used in a complementary way. High-resolution anatomic information produced by CT adds significant information to tissue characterization delivered by PET. In addition, fusion of high-resolution MRI anatomic and functional information with PET will provide an extra dimension. When applying the integration of different imaging modalities, image fusion becomes an issue. Adequate anatomic alignment of both image sets permits convenient visualization of all information in one study.
Diagnostic Effect
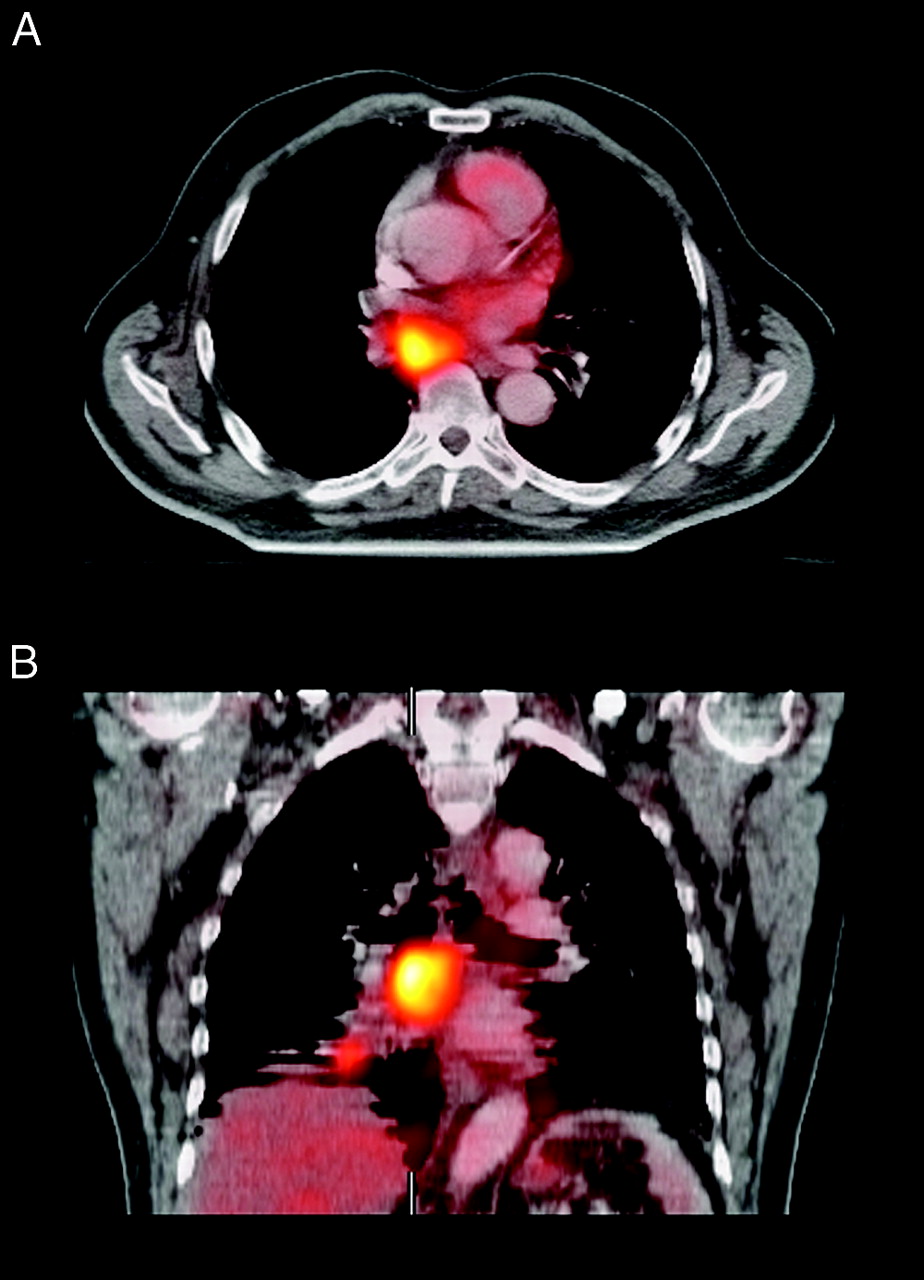
Improved lesion characterization and localization will result in increased diagnostic accuracy, which is recognized as a beneficial diagnostic effect. However, better accuracy in staging and restaging of disease is only relevant when it leads to changes in patient management (e.g., by decreasing the indication for invasive procedures). Also, improved lesion localization may lead to better results in other successive diagnostic procedures (e.g., easier CT-guided biopsy). Figure 1 is an example of improved lesion localization with software image fusion.

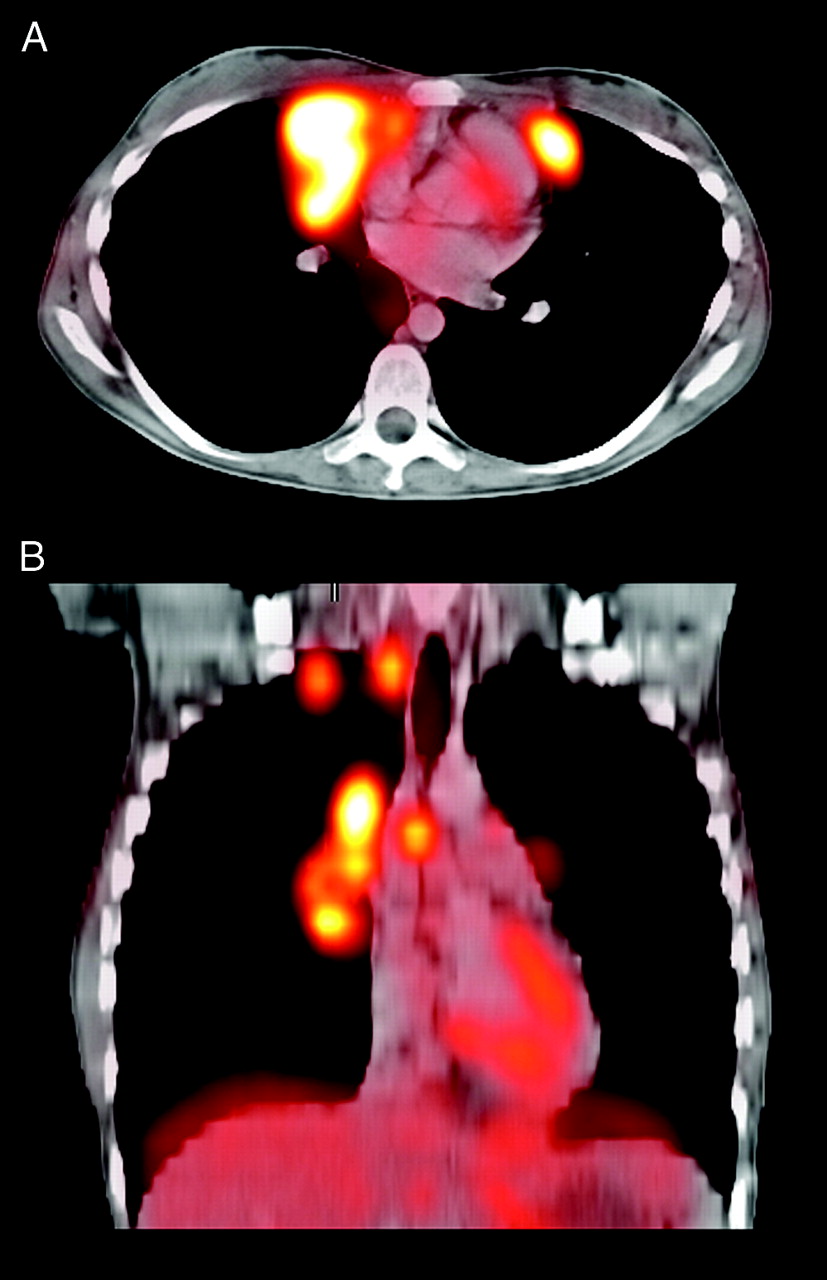
Example of software fusion of 18F-FDG PET and CT images for lesion localization. (A) 18F-FDG PET clearly showed pathologic lesion somewhere in upper thoracic aperture. More precise localization was not possible because of lack of anatomic information. (B) Lesion was not found retrospectively on diagnostic CT images. (C) Image fusion localized lesion in rib near costovertebral joint.
Integration of multiple functional imaging techniques, such as PET studies with various tracers or functional MRI with contrast enhancement and MRS, results in comprehensive in vivo tissue characterization.
Effect on Therapy
PET images can be implemented in radiotherapy treatment planning and may be of particular value for high-precision techniques, such as intensity-modulated radiotherapy (IMRT). With IMRT, different dose prescriptions can be delivered to multiple target sites with extremely high dose gradients between tumor and normal tissues. This places demands on the ability of conventional imaging techniques to localize and delineate tumors. PET scanning can detect additional lesions or may provide complementary information to facilitate the interpretation of equivocal CT findings (e.g., marginally enlarged lymph nodes). Consequent adjustments of the radiotherapy target volume will have a direct effect on the chances of cure, and on the risk and level of side effects and on complications.
In addition, functional PET imaging may identify tumors or regions within tumors with increased radioresistance. Examples are tumor hypoxia and areas of very active tumor cell proliferation that can be detected by specific tracers (2). A next step in the development of IMRT will be the integration of anatomic and functional information into a biologic target volume (3). Using the ability of IMRT to deliver nonuniform dose patterns, biologic dose conformality can be pursued, creating higher doses to areas of increased radioresistance, and lower doses in areas of high radiosensitivity. Figures 2 and 3 demonstrate the use of software image fusion in IMRT planning. Figure 4 is an example of a resulting IMRT field.

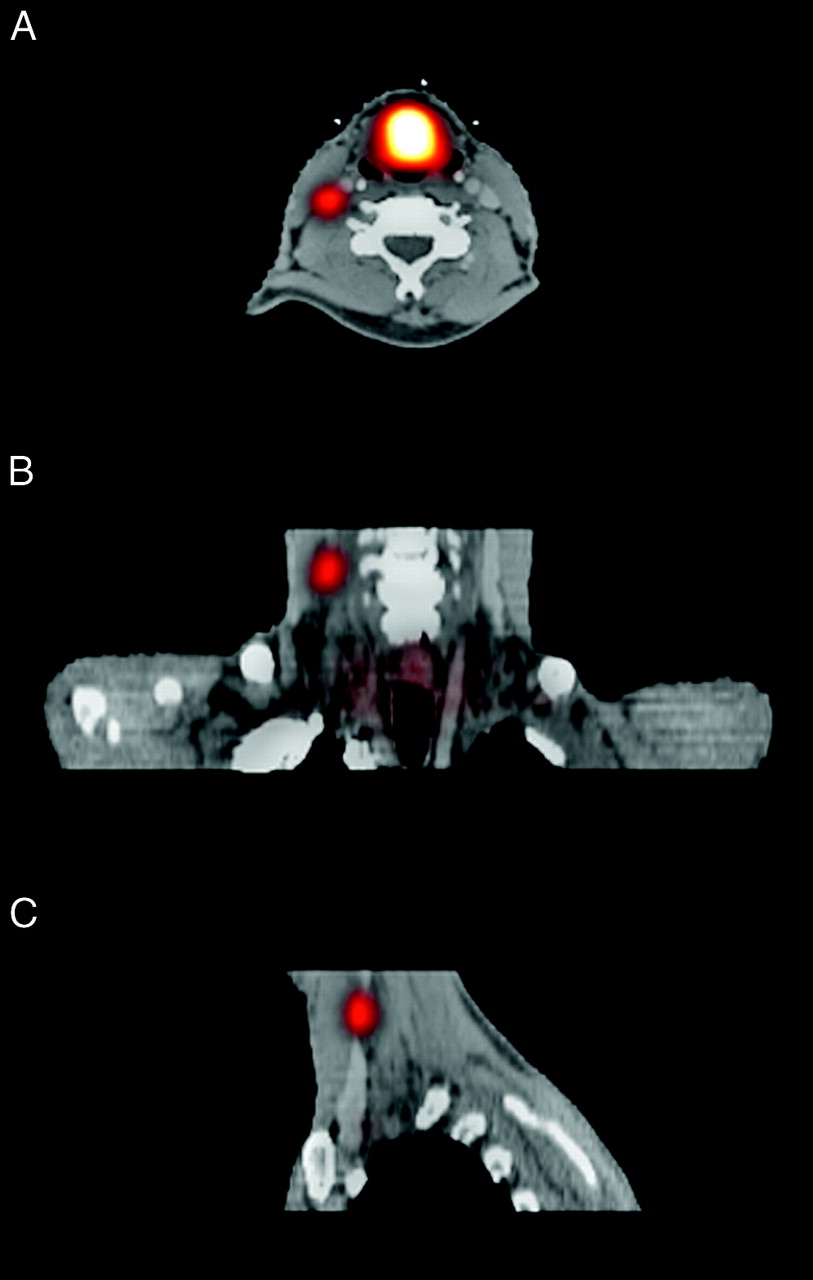
Example of software fusion of 18F-FDG PET and CT images of primary laryngeal carcinoma for IMRT field planning. Patient was scanned for both 18F-FDG PET and CT on flat bed, in personalized rigid radiotherapy mask covering head and shoulders to prevent positioning differences. Lymph node in neck that was only marginally enlarged on CT proved pathologic on 18F-FDG PET and was included in the radiotherapy field. (A) Transverse slice through pathologic lymph node. (B) Coronal slice. (C) Sagittal slice.

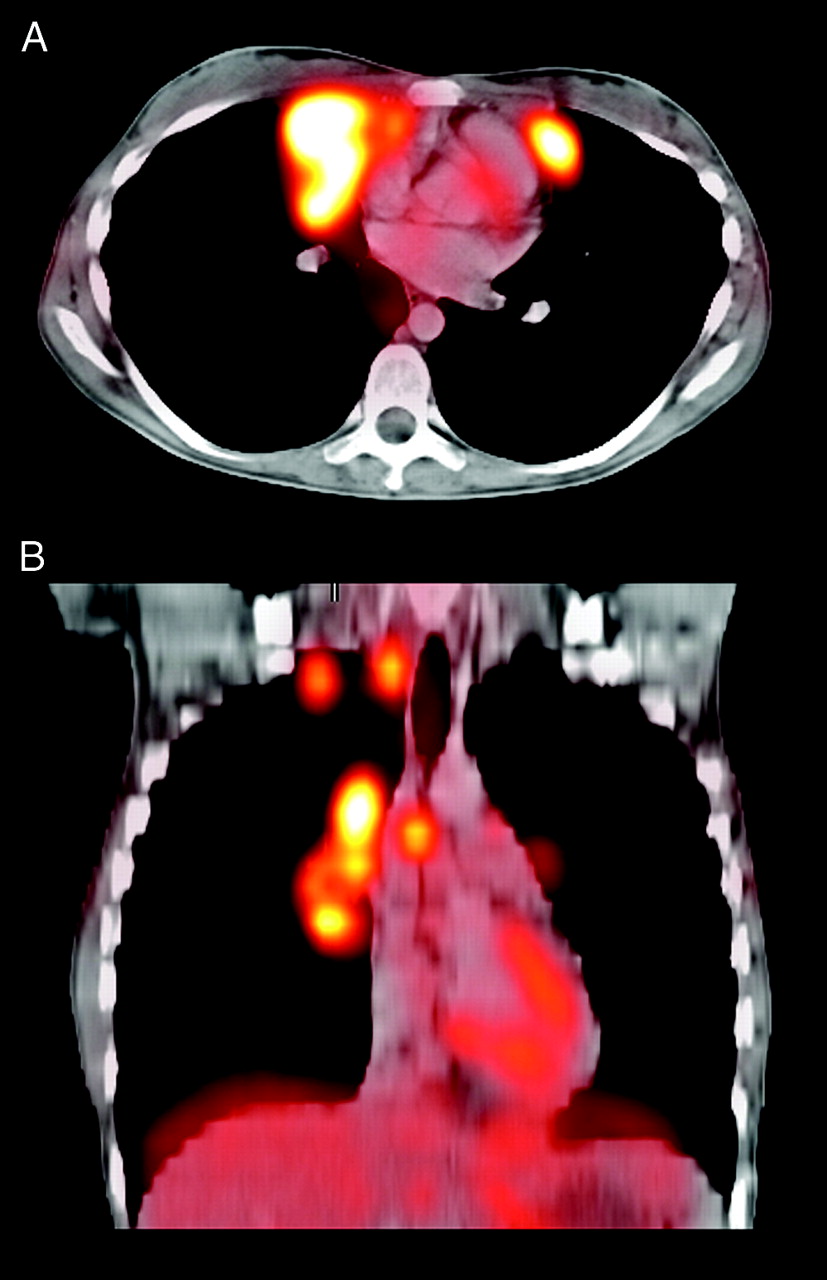
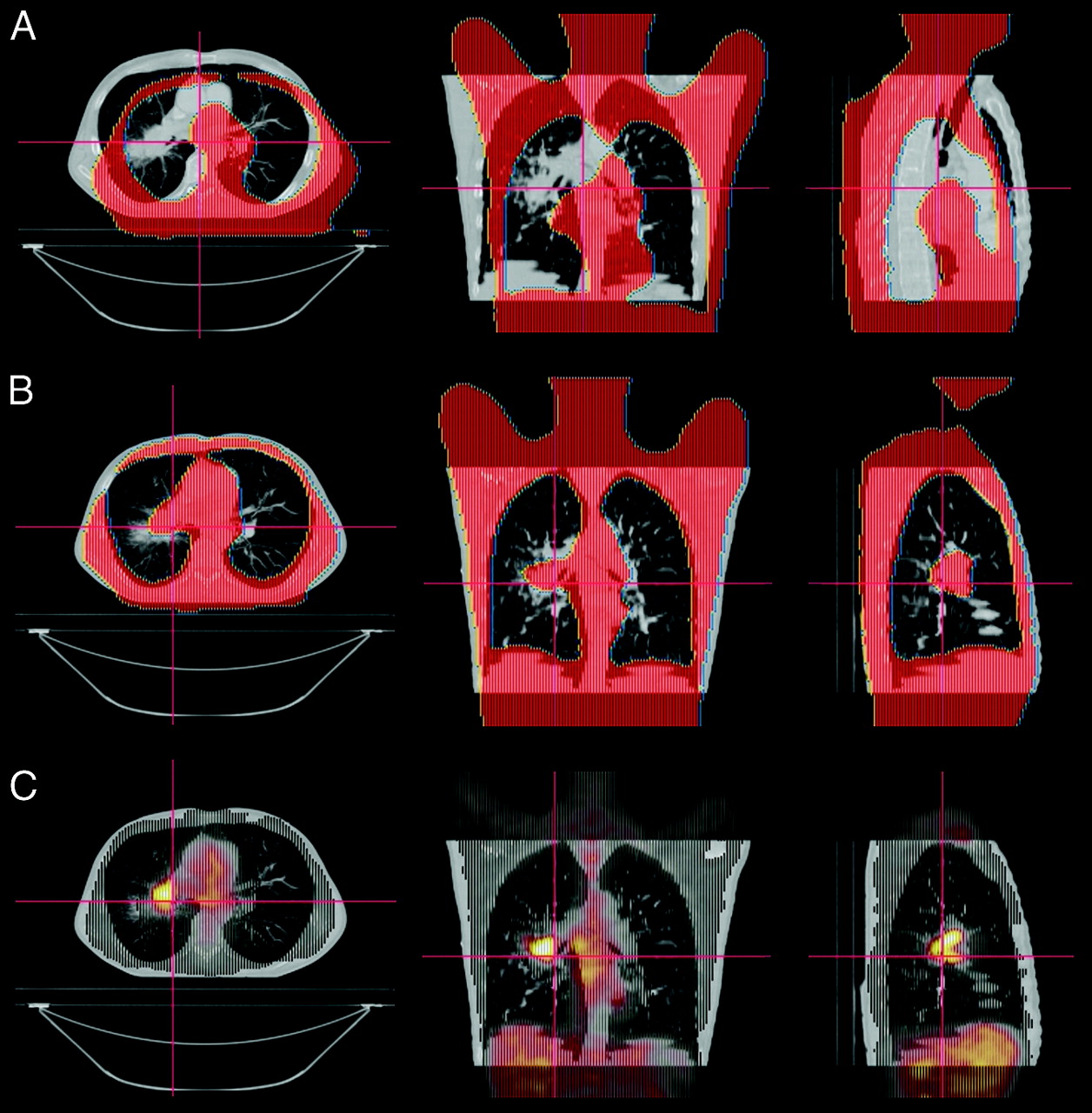
Example of software fusion of 18F-FDG PET and CT images of primary non–small cell lung cancer with lymph node metastasis in mediastinum for IMRT field planning. Patient was scanned for both 18F-FDG PET and CT on flat scanning bed, with arms up in rigid customized support system to minimize positioning differences. CT images were acquired during free tidal breathing, accounting for huge artifacts. 18F-FDG PET images were also acquired during free tidal breathing but show much more reliable delineation of tumor tissue. (A) Transverse slice. (B) Coronal slice.

Sample IMRT field planning of oropharyngeal squamous cell carcinoma. Different levels of radiation dose are drawn in red in 3-dimensional space. Painted in blue is spinal cord that will be spared. Reverse planning was used to calculate optimal shape and intensity of 7 beams.
MRI and dynamic and spectroscopic MR information also can be used to target IMRT and have been shown to very accurately localize prostate cancer (4,5). Fusion of this functional MR information with CT has also been shown to be possible (6).
The potential value of combined modalities is easy to recognize. Joined information may prove synergistic. It allows accurate differentiation between pathologic and normal tissue, with excellent resolution and localization, and it creates opportunities for further optimization of treatment. The question that remains to be answered is whether only a combined PET/CT scanner can live up to this expectation.
LEVELS OF IMAGE FUSION
When reading 2 image studies such as PET and CT, 3 levels of image fusion are possible: visual, software, and hardware fusion. When 2 studies need to be correlated, what level of image fusion is preferred or needed?
Often No Need for Image Fusion
A PET scan without a CT scan is not useless. On the contrary, most PET scanners today operate as stand alones and perform quite well. In most cases, PET images contain enough information to answer relevant clinical questions. Additional information necessary to interpret the images should be retrieved from the referring physician or from previous imaging, such as CT, ultrasound, or MRI.
Visual Fusion
The reviewer traditionally has had a film print or digital display of a previously recorded CT scan next to PET images and overlaid the images in his or her mind while reviewing. This is called visual fusion. Based on clinical experience, Jager et al. (7) estimated that there is a need to look at CT images in only about 20% of cases. They also stated that, in the majority of these selected cases, visual fusion gives sufficient information with no actual need for or additional value from soft- or hardware image fusion. Others emphasize the necessity of an extensive review of CT images in all cases. These 2 opinions, neither founded on evidence-based data, serve as a source of controversy.
Software Fusion
Integration of separate PET and CT image sets into a single study can be achieved with software fusion. Several commercial packages have been developed for this purpose. These packages share a similar set of functions for fusion and visualization.
The most elementary method of image fusion is manual positioning of one scan relative to the other in a 3-dimensional space, with 9 free parameters for adjustment of position, size, and rotation in 3 directions each. This is a very time-consuming procedure and, more important, is highly operator dependent and not very accurate. Marking of recognizable points in both scans (so-called landmarks, either anatomic or artificial) was introduced initially for optimization, but lack of such anatomic points on PET and low correlation of external fiducial markers with internal organ positions limits the applicability of this technique. The true power of these software packages lies in the use of automatic optimization algorithms, which eliminate operator dependency and increase accuracy by considering all parts of both scans simultaneously. Numerous algorithms have been developed for this purpose. Examples include count difference, shape difference, mutual information, normalized mutual information, and others. All currently used algorithms produce fused images, but the results vary in accuracy. It is unclear which algorithm performs best in a specific situation. However, mutual information is generally accepted as the most robust procedure. Both PET emission and transmission images (or even a combination of those in a given ratio) may be considered when optimizing (8). Only rigid transformation algorithms are currently commercially available and widely used. In the near future, elastic transformation will become available, possibly allowing automatic correction of small breathing artifacts and positioning differences (9,10). Still, it is unlikely that advanced techniques in software fusion will ever be able to correct for extreme positioning differences and motion artifacts. Furthermore, patient logistics and network connectivity are relevant issues when performing software image fusion, because each may lead to additional delay.
The software fusion process typically consists of several steps. First, 2 image sets must be loaded into the computer system running the fusion application. If all geometric parameters are correctly defined, both image sets will appear in an integrated image set with a certain displacement and possibly a small rotation along 3 axes. A quick correction of the most obvious displacement may be performed manually. Additional optimization must be achieved by automatic registration, which also will be fast. The resulting integrated image set may be viewed or saved to a picture archiving and communication system. Figure 5 shows an example of the procedure.
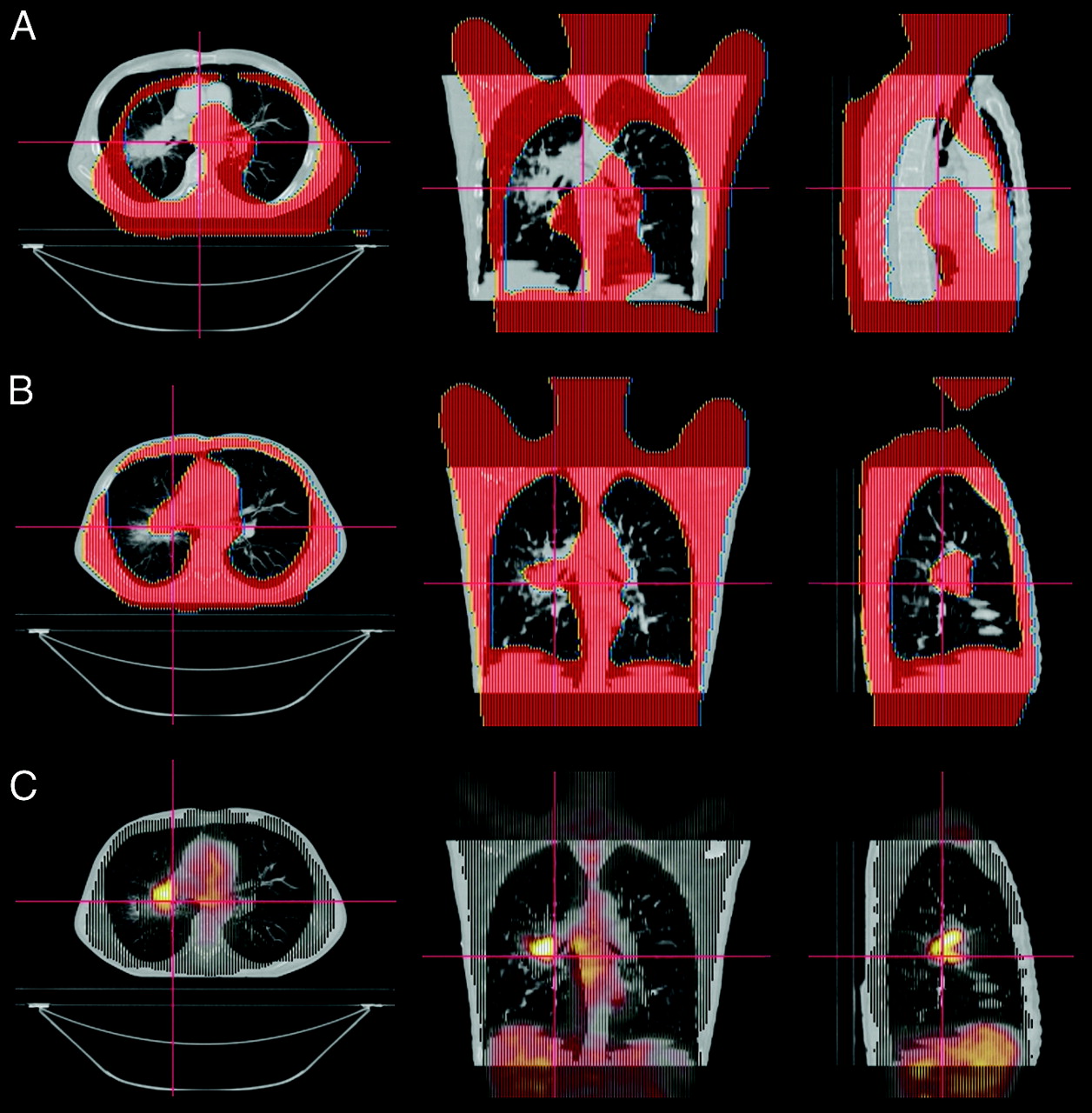
Example of software fusion procedure for 18F-FDG PET and CT images. (A) After loading both scans in fusion software, large shift exists. PET transmission images in CT are displayed for easier recognition of body outlines. (B) Optimized fusion after automatic registration with mutual information algorithm. (C) Final result with 18F-FDG PET emission images displayed in CT.
Hardware Fusion
As stated previously, true hardware image fusion of PET and CT is not yet possible. The term hardware fusion currently refers to a PET/CT scanner, which includes separate scanners positioned in line at a fixed distance. In fact, current combined PET/CT scanners can be described as expensive patient positioning systems that facilitate obtaining a dedicated CT and a dedicated PET in one session with minimal patient movement at the cost of occupation of the CT while scanning PET and vice versa. The acquired image sets are calibrated to be overlaid correctly within a certain error but are not routinely corrected for breathing artifacts or accidental positioning changes between the 2 scans. Because of these inaccuracies, CT-based attenuation correction for the PET images, advocated for its speed of acquisition, will introduce certain artifacts. Software for optimization or correction of these errors in hybrid PET/CT images is not widely used currently.
Nevertheless, the use of a combined PET/CT scanner has several definite advantages over separate scanners. The patient lies on the same bed in the same position. Therefore, the image fusion procedure logistics are easier and probably less prone to artifacts resulting from positioning differences. In addition, total scanning time is shorter when using the CT for attenuation correction of PET data.
A Point of Controversy
The required level of image fusion remains open for debate. It is unclear whether the increased scanning speed and somewhat easier image fusion (when needed) are sufficient compensation for the higher radiation exposure and high cost of a combined PET/CT scanner. No studies have yet addressed this problem as a whole.
Lardinois et al. (11) studied hardware image fusion compared with CT alone, PET alone, and visual correlation with histopathology as a gold standard in staging 49 patients with non–small cell lung cancer. Software image fusion was not performed in this study. The authors found integrated PET/CT significantly more accurate in staging the primary tumor than CT alone, PET alone, or visual image fusion. They reported improved accuracy in staging lymph nodes compared with PET alone, but no significant difference in accuracy was found between integrated PET/CT and visually correlated images. Integrated PET/CT provided additional information over visual fusion in 41% of cases, including more exact localization of tumor sites, precise evaluation of chest wall or mediastinal involvement, and differentiation between tumor and peritumoral inflammation or atelectasis. However, the key questions, whether and to what extent patient management or therapy outcomes were changed, were not addressed.
PROBLEMS AND LIMITATIONS
When using image fusion in daily clinical practice, a certain level of accuracy in positioning one image set relative to the other must be achieved or, better, guaranteed. Does hardware image fusion perform better than software fusion?
Accuracy
The maximum achievable accuracy in image fusion depends on several factors. Most important are patient positioning differences, internal organ movements (e.g., breathing and movement of the heart), attenuation correction artifacts, and errors in the fusion procedure. Figure 6 shows the potential results of some of these effects. To a certain degree, these factors (except for CT-based attenuation correction artifacts) are present in both soft- and hardware fusion. The presence of these errors must be checked and corrected when possible. This can be done with image registration software.
Example of failed software image fusion in patient with B-cell lymphoma. CT images were acquired during breath hold at deep inspiration with arms up. 18F-FDG PET images were acquired during free tidal breathing with arms down. Fusion images show major inaccuracies in upper thorax aperture and in region of diaphragm. (A) Transverse slice. (B) Coronal slice.
Patient Positioning and Movement
Patient positioning should be identical during the PET and CT scans. This implies scanning with the arms either up or down in both scans, with identical support material under the head and neck and with similarly shaped scanning beds. The choice of arm position depends on the purpose of the scan. In most diagnostic procedures, CT scans are acquired with the arms up. PET scans are usually acquired with the arms down for patient comfort during the relatively long scanning period. Compromises may be unavoidable in image fusion.
Patient movement should be minimized during and between scans by instructions and additional support material. Various types of custom-molded support cushions are available for this purpose. When very high accuracy is needed (e.g., in radiotherapy of the head and neck) customized head support devices and immobilizing masks are recommended. Despite best efforts, patient movement can never be ruled out as a source of error.
Patient positioning and motion errors are possible when imaging with separate scanners as well as with integrated PET/CT scanners, although the chance of large positioning differences between scans seems significantly lower in the latter. This problem requires more attention when using separate scanners but can be largely overcome when handled appropriately. Equipment suppliers should facilitate this by providing the same bed for PET and CT.
Organ Movement
Because of the duration of the scan, PET is acquired during free tidal breathing. This implies continuous movement of the thoracic wall, lungs, mediastinum, diaphragm, and upper abdominal organs, leading to displacement (up to several centimeters), rotation, and deformation of organs. Therefore, diagnostic CT scans are usually acquired during deep inspiration breath hold. Standard PET and CT, then, will inevitably contain major differences. The only available solution is the acquisition of the CT scan during free breathing (with the introduction of serious artifacts on CT) or during breath hold in a fixed position. Goerres et al. (12) reported the best match of CT and PET when scanning CT in unforced expiration but also recognized the inability of most patients to hold this position during a whole-body CT. A compromise suggested by Beyer et al. (13) allowed the patient to breathe free at the beginning and end of the CT scan and advocated unforced expiration during scanning of the lower lung and upper abdominal region. This procedure provides an acceptable although still not perfect result in image fusion. Reliability in the diaphragmatic region remains poor. Novel respiratory-gated PET scanning techniques are being developed but are not yet clinically used (14). This problem is not solved, and it persists in both integrated PET/CT and separate scanners.
Considerable motion and displacement of internal organs are often problematic in scans of the pelvic region. This is mainly caused by variations in bladder and rectal filling, which in turn can affect prostate and uterus position. This problem is probably best solved by keeping the interval between the scans as short as possible.
Although combined PET/CT scanning delivers readily aligned image sets, it is not perfect by default. The scans may be slightly misaligned as a result of a calibration error in the relative CT and PET scanner positions. Minor differences in patient positioning may occur, and differences in diaphragm position will exist. A minimal error of several millimeters is considered unavoidable. However, variations in positioning and initial misalignment will be larger when using separate scanners.
Scanner Resolution and Inaccuracy
The minimal error that can be visualized and corrected, either manually or with automatic registration, is limited by the resolution of both scans. For PET and CT this implies an error of approximately 5 mm in the transverse plane and at least 5 mm along the longitudinal axis, depending on the thickness of CT slices. Automatic registration may achieve a somewhat higher accuracy by considering all slices at the same time, but this is difficult to prove.
The total inaccuracy of fusion consists of the added inaccuracies caused by positioning differences, motion artifacts, and the fusion procedure itself. As a rule of thumb, the total minimal theoretic error can be estimated at approximately 10 mm in all directions and probably twice that in the diaphragmatic region. The minimal error may be less in rigid body parts, such as the brain. The minimal error is unavoidable in image fusion, whether a separate or combined PET/CT scanner is used. Many soft- and hardware solutions claim higher accuracy in image fusion, up to 1–2 mm in all directions. Such claims are based on phantom studies and disregard the specific problems inherent when scanning living subjects.
Acceptable Inaccuracy
The required accuracy of image fusion depends on the clinical question that needs to be answered. To correctly distinguish 2 lesions, the error must be smaller than the size of the lesions. The smallest lesion that can be detected with PET is just below 1 cm in diameter. Therefore the maximum level of accuracy that can be achieved is also just below 1 cm in all directions.
In radiotherapy of the head and neck area, with optimal positioning and immobilization, the error in dose delivery is in the order of 2 mm or less (15). Such degree of accuracy cannot be achieved with a PET scanner with 5-mm spatial resolution. The total error of PET/CT fusion must be considered when defining the target volume in radiotherapy. As a consequence, the target volume will increase. On the other hand, the interobserver variations in contouring tumor volumes can be significantly reduced because of the higher specificity of PET information (16). These factors must be weighed against the benefits of higher sensitivity of tumor detection and the availability of additional functional information. It opens a whole new field of research and development.
Because additional error has direct consequences for the size of radiation volumes, every effort must be made to achieve the highest possible accuracy. This means that all imaging, as well as the actual radiotherapy, must be performed with the patient locked in a rigid mask that prevents any movement or variation in positioning. In radiotherapy field planning of the lungs and mediastinum, the CT scan is recorded during free breathing to mimic the situation during radiotherapy. Under these conditions, the CT has an effective total error of several centimeters. Here, the PET scan is considered to have a better resolution, as illustrated in Figure 3. New developments in radiotherapy treatment planning and delivery address this problem. The use of multiple, so-called “slow” CT scans, which use long sampling times for image registration, allows better capture of tumor movement and generates more reproducible target volumes (17). The precision of dose delivery can be improved with respiratory-gated radiotherapy, where dose delivery is adjusted to the breathing motion of organs. Again, for these issues, no significant difference exists between the use of 2 separate scanners and a combined PET/CT scanner.
All errors mentioned here are theoretic estimates. Unfortunately, the real error made in image fusion cannot be assessed objectively, because no gold standard is available. However, methods to evaluate the quality of image fusion have been developed and are used in research settings (18). The human eye is the only available instrument to recognize specific errors in individual cases. This means that for both soft- and hardware solutions, image fusion has no “guaranteed” accuracy—only estimated minimal errors.
ATTENUATION CORRECTION
Advantages
Most institutions perform a transmission scan to correct the emission scan for attenuation. The time needed for the transmission scan using radioactive sources is about 30%–40% of the total scanning time. The CT scan of a PET/CT study can also be used to correct the PET emission for attenuation, thus decreasing the total PET scanning time. It is obvious that such reduction in scanning time will not be achieved when 2-dimensional emission data alone are used to read the PET images.
Another advantage of CT-based attenuation correction is a lower noise level in the CT images compared with that in traditional transmission images, resulting in corrected PET images with less noise.
Disadvantages
Using CT data to correct PET emission data to reduce total scanning time is tempting. However, significant additional errors may be introduced. As indicated previously, positioning and breathing protocol differences between the CT and PET scans will result not only in image fusion errors but also will introduce quite serious artifacts in the attenuation-corrected PET images, especially in the diaphragm region where lesions may be projected in the wrong organ (19). The use of lower energy x-rays instead of a 511-keV transmission source also will result in more artifacts in the area of metallic implants. Overcorrection will result in false hotspots, unless the attenuation correction algorithm is specifically adapted to this problem (20). Serious distortion effects have been demonstrated on PET near dental implants and prostheses (21,22). Dizendorf et al. (23) reported that contrast fluids have some effect but that this did not lead to serious misinterpretations. Uncorrected PET images should be viewed when using CT-based attenuation correction, thereby avoiding serious misinterpretations.
In theory, it is possible to use CT data for attenuation correction of PET data as acquired on a separate PET scanner. However, such a procedure is considered cumbersome because of logistic implications and the very high risk of artifacts.
ADDITIONAL ARGUMENTS
The clinical and technical arguments mentioned previously are perhaps the most important, but the discussion is certainly not limited to these. Several other factors with regard to PET/CT should be considered.
CT Quality
CT scans acquired with a combined PET/CT scanner may not be of the best diagnostic quality. Because the main purpose of the CT scan in this combination is coregistration and attenuation correction, a single-slice, low-energy CT scan with relatively low contrast and resolution and a relatively large slice thickness is sufficient. In some modern scanners a high-resolution, multislice scanner is available, but in most cases the patient has already undergone a high-quality diagnostic CT scan before referral for PET. This limits the need for a second state-of-the-art CT scan.
Radiation Dose
In PET/CT scanning, the patient undergoes a CT scan, regardless of whether a diagnostic CT scan is already available. This implies a second radiation dose. A standard PET emission scan delivers a radiation dose to the body of 5–10 mSv. A traditional germanium-based transmission scan delivers no significant dose to the patient. When using a modern multislice CT, the received dose may be up to 10 mSv for the head, 20 mSv for the chest, and 20 mSv for the abdomen. This would be a significant increase in total radiation to the patient for PET scanning. This extra radiation dose can be decreased by using lower-energy x-rays and thicker slices that are sufficient for CT-based attenuation correction and simple lesion localization in PET/CT scanning. Nevertheless, a total-body CT dose of 10 mSv added to the normal PET emission dose is very common. In nuclear medicine, a trade-off between scanning speed and radiation dose always exists but usually is not that significant.
It is also worth considering that a combined PET/CT scanner delivers a CT scan with every PET scan, needed or not. The CT scan then should be used for diagnosis. It would be poor radiation safety practice to acquire a whole-body CT scan for faster attenuation correction only and not even look at the inherent diagnostic information afterwards.
Eventually, implementation of PET/CT as a common tool in diagnosis may lead to an adaptation of the diagnostic strategy. In certain situations, obtaining a diagnostic CT before PET/CT may not be necessary. Such a strategy is currently under investigation for the diagnostic work-up of patients with suspected lung cancer, and some institutions have already implemented this in routine clinical practice for this diagnosis.
Combination with Other Modalities
The combination of PET and CT may be attractive, but the integration of PET with imaging modalities other than CT can have additional important advantages. MRI is superior to CT in visualization and delineation of soft tissue anatomy. The combination of PET with imaging modalities that do not contribute to radiation dose, such as MRI, would be preferable in terms of radiation safety. The fact that PET/CT is the only available combination right now does not make it a panacea. In the near future, image fusion of PET with other modalities is certain to become an issue, and it would be unwise to direct all attention, efforts, and available budget to a single option. This may even slow down development in other important areas of image fusion.
Economy
The purchase of a combined PET/CT scanner is quite costly and must be adequately justified. The difference in price between a PET/CT unit and a dedicated PET scanner is sufficiently large to warrant considering spending the budget on other, more urgently needed items. This becomes even more of an issue when taking into account the fact that the high-end CT included in a PET/CT scanner will be operated for only 1 min per patient for a total of only 10–20 min per day.
The combination of 2 advanced imaging devices in 1 machine at least doubles the chance of technical failure. Personnel dually trained in PET and CT techniques are needed to adequately operate such a machine. Such factors increase the total costs of ownership.
Competence Issues
When a nuclear medicine department begins using a CT scanner, competence issues may arise with the radiology department. Are the CT images used for localization and attenuation correction only? Are nuclear medicine physicians allowed to review the CT and use it as a diagnostic tool as well? Can these findings end up in the PET report? Should a radiologist always look at the CT images? Can this be done separately, or is a joined image reading session mandatory? On the other hand, the radiotherapy department may want to use a PET/CT scanner to improve radiation treatment planning. Competence and responsibilities of nuclear medicine physicians, radiologists, and radiation oncologists need to be defined.
CONCLUSION
Without reservation, the answer to the question of whether we need CT in combination with PET is yes. However, questions about the required level of image fusion are far from settled. In the authors’ opinion, side-by-side reading of PET and CT (meaning visual image fusion) is sufficient and adequate in many cases. Moreover, scientific data are unavailable to demonstrate unequivocally that state-of-the-art software fusion is less accurate than the hardware fusion provided in current PET/CT scanners. Suggesting the primacy of a combined PET/CT scanner over stand-alone PET and CT is more a matter of belief than of science.
The possession of a PET/CT scanner does not automatically upgrade an institution to the top of its class, and, perhaps more important, an institution with a state-of-the-art PET scanner, state-of-the-art CT scanner, and state-of-the-art software for image fusion is definitely not second class. High quality should be defined by state-of-the-art PET, CT, adequate software for image fusion, and knowledgeable multidisciplinary interpretation. Those institutions starting with clinical PET can perform very well with a stand-alone, dedicated PET scanner, in combination with software fusion when needed. The extra expense of a PET/CT scanner should be weighed against other, possibly more urgent, needs.
Additional research comparing the overall performance of PET/CT scanners with that of separate scanners with software for image fusion is much needed. Furthermore, the continuous development of software for image fusion and respiratory and cardiac gating is not only needed for combined PET and CT imaging but also for fusion of PET with MRI and CT with MRI. For these reasons, it is counterproductive when only PET/CT scanners receive the full attention of the nuclear medicine community.
Footnotes
Received Oct. 17, 2003; revision accepted Nov. 5, 2003.
For correspondence or reprints contact: Wouter V. Vogel, MD, University Medical Center Nijmegen, Department of Nuclear Medicine (565), Postbox 9101, 6500 HB Nijmegen, The Netherlands.
E-mail: w.vogel{at}nucmed.umcn.nl.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Future of Nuclear Medicine, Molecular Imaging, and Theranostics
- Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors
- Evaluation of Image Registration in PET/CT of the Liver and Recommendations for Optimized Imaging
- Introduction