


Abstract
18F-FDG PET offers the radiation oncology community the ability to incorporate biologic information into radiation therapy targets. To date, most of the work in this arena has involved patients with non–small cell lung cancer (NSCLC). The literature suggests that biologic targeting with PET alters the radiation treatment volume significantly in 30%–60% of NSCLC patients for whom definitive therapy is planned. This is mostly the result of the incorporation of regional nodes with 18F-FDG avidity that were previously judged to be uninvolved by CT criteria. The development of the integrated PET/CT scanner is a valuable tool that improves diagnostic accuracy for staging this disease and will increase the accessibility of PET for radiation treatment planning. Its implementation into radiation treatment planning requires strong collaboration between radiation oncologists and nuclear physicians. In this report, we will review the literature on PET-based radiation treatment planning, its potential benefits, and future challenges.
In recent years, technologic advances in PET have created increasing interest in the use of this modality for more accurate tumor staging and treatment planning. The ability to obtain information with PET regarding tumor biology has led to the concept of biologic target volumes in radiation treatment planning (RTP). Use of this biologic information, in addition to the anatomic information obtained by CT or MRI, offers a new opportunity to target cancers for radiation therapy. Although the clinical application of PET has largely been focused on its uses in differentiating benign from malignant disease and for the staging of malignant neoplasms, PET has great potential for RTP. To date, most of this work has involved patients with non–small cell lung cancer (NSCLC). The recent development of the integrated PET/CT scanner promises to facilitate the application of PET in patients receiving definitive radiation therapy for cancer. In this paper, we review the literature on PET-based RTP in NSCLC, its potential benefits, and future challenges.
BACKGROUND
At the present time, clinical oncologic PET is performed almost exclusively with the radiolabeled glucose analog 2-[18F]-FDG. Compared with normal tissues, most tumors have higher metabolic rates for glucose (and for 18F-FDG) (1). 18F-FDG PET allows direct demonstration in vivo of this fundamental biochemical disturbance associated with malignant neoplasms. After injection, 18F-FDG is accumulated intracellularly by membrane glucose transporter proteins and then undergoes phosphorylation by hexokinase to 18F-FDG-6-phosphate (1). However, 18F-FDG-6-phosphate is not further metabolized via glycolytic or glycogen-synthetic pathways, and, because it is charged, cannot diffuse out of cells that have absent or low activity of glucose-6-phosphate. Therefore, 18F-FDG-6-phosphate becomes metabolically “trapped” within the cell. The tissue level of 18F radioactivity reflects the rate of glucose consumption at a specific site.
RTP APPLICATIONS FOR LUNG CANCER
A large body of literature documents the value of PET in the diagnosis and staging of NSCLC. About 10%–30% of patients with stages I–III NSCLC as determined by conventional imaging may be found with PET to have distant metastases (2). An additional 10%–20% may be upstaged by finding regional nodal involvement that was not previously appreciated (3). As a result, 18F-FDG PET offers a potential benefit in treatment planning for these patients (Figs. 1 and 2).

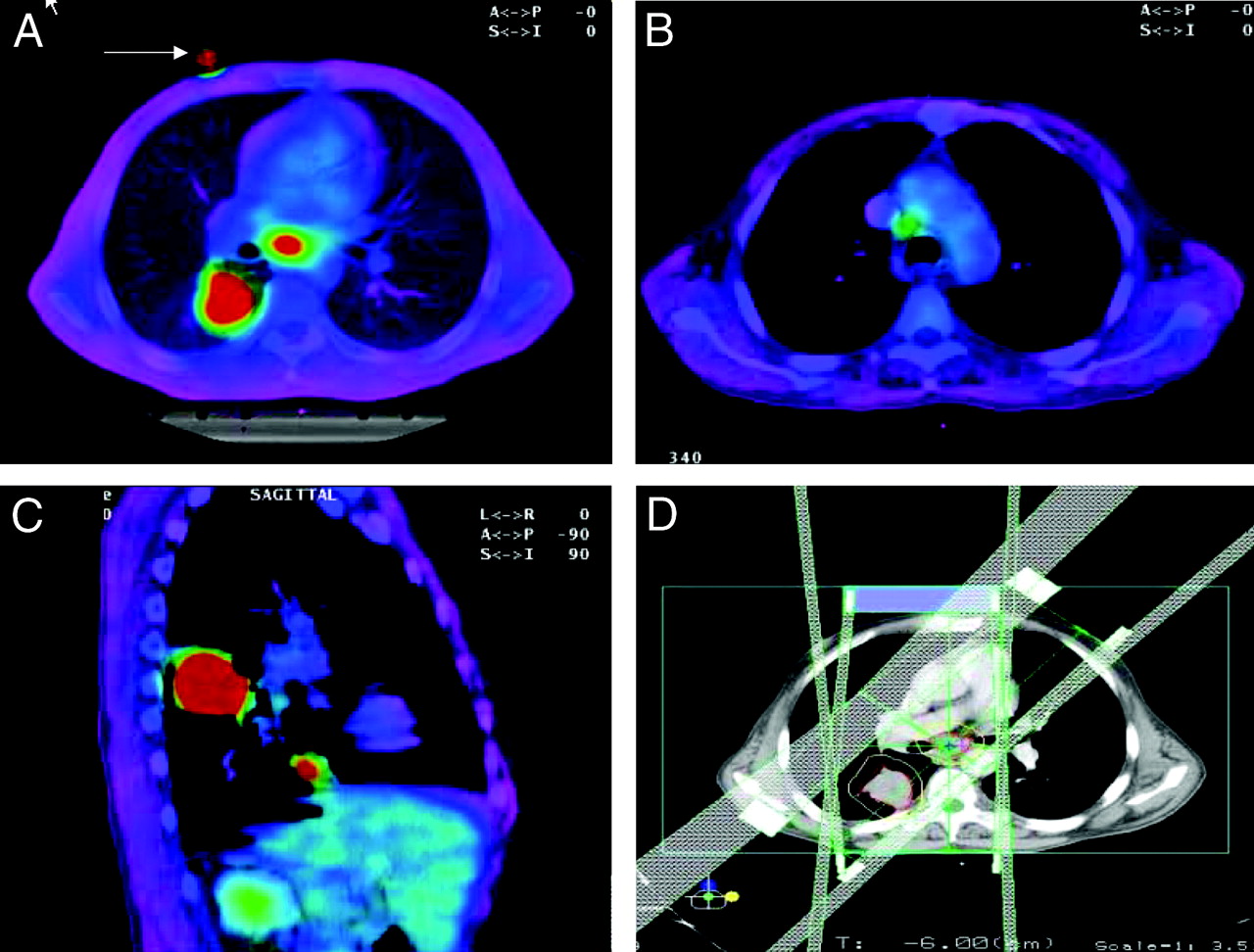
Fused PET/CT images of patient with T4 N2 M0, stage IIIB NSCLC. Patient has 2 primary lesions in right lower lobe (best seen in C) with adenopathy in subcarinal (A) and right paratracheal regions (B). PET and CT images were coregistered with aid of fiducial markers, 1 of which is shown in A. (D) Beam arrangement used to cover biologic target volume.

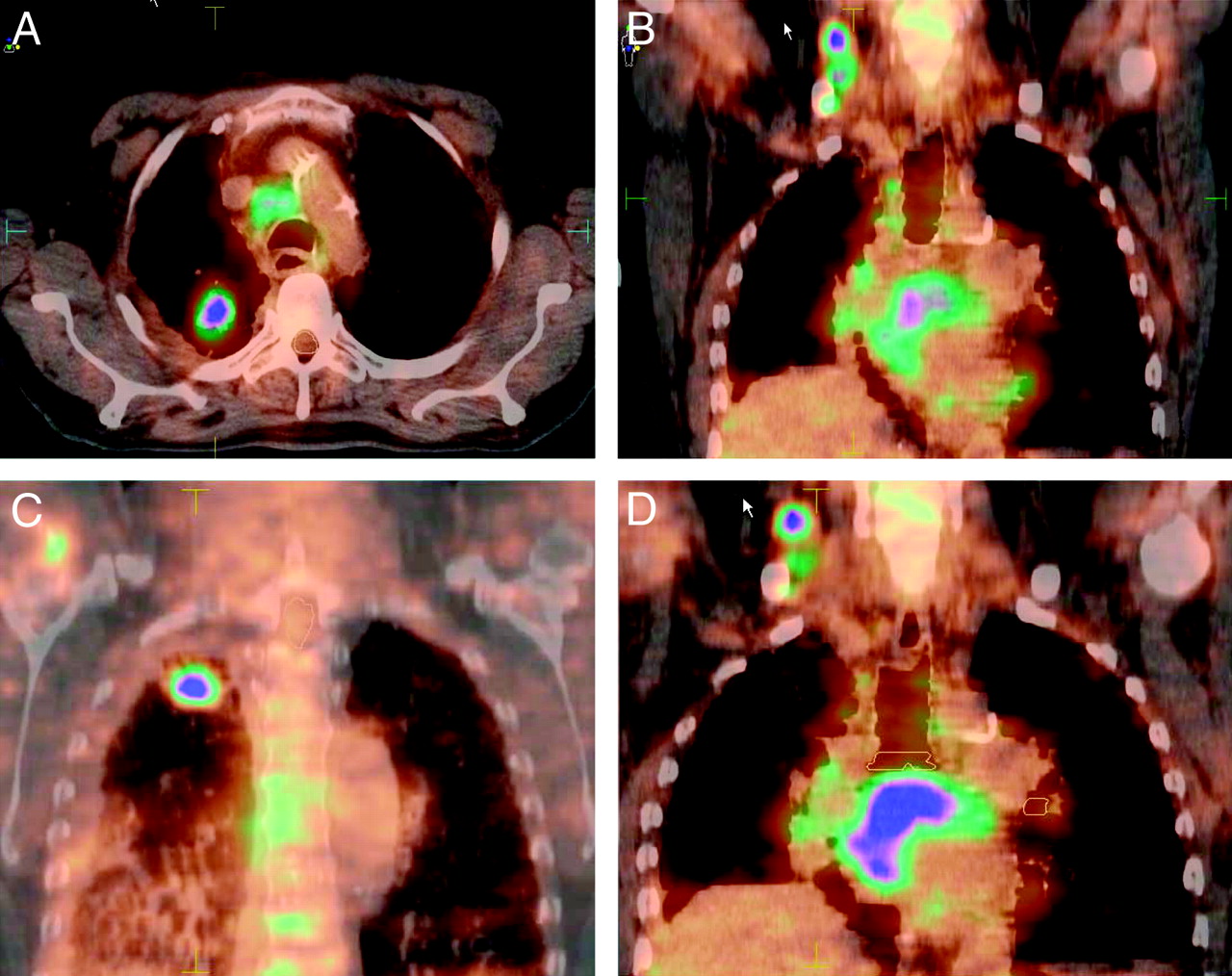
PET/CT images of patient with T2 N3 M0, stage IIIB NSCLC, showing biologic target volume to include right upper lobe lesion (A and C), ipsilateral cervical adenopathy (B and D), and bulky subcarinal adenopathy (D). Cervical adenopathy was not appreciated on previous CT examination of thorax but was detected with PET.
Several investigators have reported results for staging the mediastinal lymph nodes with 18F-FDG PET (4–14). In 1 of the largest studies, Pieterman et al. (14) evaluated 102 patients with resectable NSCLC and compared the results of PET and CT. The sensitivity and specificity of PET for detection of mediastinal metastases were 91% and 86%, respectively. The corresponding values for CT were 75% and 66%, respectively (P < 0.001). PET identified distant metastases not detected by standard methods in 11 of the 102 patients. The use of PET resulted in lowering of the clinical stage in 20 patients and upstaging in 42 patients (4–14). Toloza et al. (15) recently reported a metaanalysis of results comparing CT and PET staging of mediastinal nodes. The pooled sensitivities were 57% and 84% for CT and PET, respectively. The pooled specificities were 82% and 89%, respectively. The sensitivity and specificity of combined CT and PET interpretation ranged from 78% to 93% and from 82 to 95%, respectively. Thus, it is predictable that the combination of PET with CT will provide an improvement over CT alone for targeting radiation therapy.
Several studies have reported the effect of 18F-FDG PET on radiation treatment volumes in bronchogenic carcinoma (16–23) (Table 1). In most of these studies, the additional information provided by PET has been incorporated through side-by-side comparison of CT and PET images or by digital overlays of separately obtained PET and CT data (image fusion). In a retrospective study, Nestle et al. (18) reported that incorporation of PET findings would have altered the shape of the radiation portals in 12 of 34 patients (35%). They used a qualitative visual method to determine target volumes. Kiffer et al. (17) used a method of graphical coregistration of coronal PET reconstructions overlaid on fluoroscopic simulation films. They found inadequate coverage of the tumor delineated on PET in 4 of 15 patients for whom treatment was planned with CT alone. They also reported an improved demarcation of tumors by PET in 3 additional patients with atelectasis. Use of the PET images for planning would have altered the radiation therapy portals in 7 of 15 patients (47%). Vanuytsel et al. (20) reported a theoretic comparison of gross tumor volume (GTV) defined by CT and by coregistered PET + CT. The pathologic extent of nodal disease was mapped by cervical mediastinoscopy in all patients. CT-based and PET + CT–based nodal maps were compared. PET findings altered the theoretic portal volume in 45 of 73 patients (62%).
Reports on Effect of FDG PET Imaging on Radiation Treatment Volumes in Non-Small Cell Lung Cancer
Munley et al. (19) performed a retrospective study of patients with lung cancer who underwent preirradiation SPECT lung perfusion scintigraphy (n = 104) and 18F-FDG PET (n = 35) in addition to the standard CT of the thorax used to perform radiation therapy treatment planning. In the 35 patients in whom CT and PET data were used for treatment planning, 12 (34%) had portions of the beam aperture enlarged beyond the initial design based on the CT scan alone. For the majority of these cases, the PET-defined target volume encompassed the CT-defined target volume so that the treatment planner had confidence that the difference between the target volumes was not the result of a coregistration error. Beam orientation based on the CT-defined target was generally not changed by PET imaging data.
MacManus et al. (24) reported on a prospective trial in which diagnostic PET studies were used for RTP. Among the 102 patients who underwent definitive irradiation, PET led to a significant increase in the target volume in 22 because of inclusion of structures previously considered not involved by tumor. In 16 patients the target volume was significantly reduced, because PET demonstrated areas of lung consolidation or enlarged lymph nodes with low 18F-FDG uptake that were excluded from the treatment volume. In 3 patients, primary tumors were seen on PET that were not identified on CT.
A few recent studies have used radiation therapy simulation based on fusion of CT and 18F-FDG PET. Mah et al. (25) performed RTP via coregistration of 18F-FDG and CT images in 30 patients undergoing definitive radiation therapy for NSCLC. Patients in this prospective study were immobilized for radiation therapy simulation and imaged using a coincidence γ-camera. Treatment was significantly altered in 12 patients (40%). The treatment intent became palliative in 7 patients. The target volume was altered to include nodal disease detected by coincidence imaging in 5 patients. The treatment volumes based on CT were judged to be inadequate in comparison with those based on combined CT and 18F-FDG imaging in 17%–29% of the cases, depending on the physician who contoured the volumes.
Giraud et al. (21) used γ-camera coincidence imaging of 18F-FDG fused with simulation CT images using external fiducial markers. Significant alterations in treatment were seen for 5 of the 11 patients (45%). Additional nodal disease was detected in 4, and metastatic disease was detected in 1. Erdi et al. (22) reported on 11 patients with NSCLC studied with a dedicated PET scanner who underwent sequential CT and PET simulations. The planning target volume (PTV) increased in 7 of 11 patients (64%) to incorporate additional regional nodal disease. PET also helped to differentiate tumor from atelectasis in 2 patients. In summary, these reported studies suggest a significant alteration in tumor volume coverage in approximately 30%–60% of patients with NSCLC whose treatment was planned using 18F-FDG images (Table 1).
We have prospectively evaluated 26 patients with stages I–III NSCLC referred for definitive radiation therapy or chemoradiation therapy (J.D. Bradley et al., Int. J. Radiat. Oncol. Biol. Phys., in press). All patients underwent CT simulation for radiation therapy followed immediately by 18F-FDG PET. Each patient was accompanied to the PET scanner by a trained radiation therapy technologist and positioned using custom immobilization and external lasers. External fiducial markers were used to fuse the 2 image datasets for RTP. The CT alone and PET/CT coregistered images for each patient were maintained separately. The target volume contours were delineated by separate radiation oncologists and compared. 18F-FDG PET findings altered the American Joint Committee on Cancer TNM stage in 8 of 26 patients (31%), and 2 patients who were diagnosed with metastatic disease based on 18F-FDG PET received palliative radiation therapy. Of the 24 patients whose treatment was planned using 3-dimensional conformal radiation therapy, PET significantly altered the radiation therapy volume outlined in 14 (58%). PET helped to distinguish tumor from atelectasis in 3 patients. Unsuspected nodal disease was detected by PET in 10 patients. A separate tumor focus within the same lobe of the lung was detected in 1 patient. Our results are similar to those in other studies described here.
FUTURE CHALLENGES
Although the incorporation of PET into RTP promises substantial benefits, achieving this in routine clinical practice poses several important challenges. These relate to the interpretation of PET images, proper coregistration of PET and CT images, computer software required for image transfer to and acceptance by treatment planning systems, and mechanisms to account for tumor motion. Most important is the need to validate that this technology improves patient outcomes.
PET Image Interpretation
Contoured target volumes are subject to interpretations that vary among observers. In a report from Mah et al. (25), 3 radiation oncologists independently defined the GTV using first CT data alone and then fused CT and 18F-FDG PET images. Target definition with 18F-FDG PET varied, depending on the physicians reading the studies, leading to a reduction in PTV from 24% to 70% in some cases and an increase from 30% to 76% in others. Radiation oncologists are not trained to interpret PET images. Strong collaboration is required between radiation oncology and nuclear medicine specialists for proper interpretation of images. In addition, reliable tools for tumor thresholding need to be developed. PET images are usually interpreted qualitatively in nuclear medicine but need to be interpreted quantitatively in radiation oncology, where edge detection is required for tumor contouring (Fig. 3).

PET images in patient with right hilar cancer. (A) PET threshold is set at 40% of maximum standard uptake value (SUV) of tumor. (B) PET threshold is set at 30% of maximum SUV. If delineating this tumor using PET alone, different threshold settings would result in different target volumes.
Image Registration
Problems with image coregistration arise from differences in patient positioning between routine PET acquisition and radiation therapy delivery. Proper coregistration requires identical patient set-up for both PET imaging and radiation treatment. Patients receiving radiation therapy are treated on a flat tabletop and are often immobilized using custom body molds. A flat tabletop insert, transfer of patient immobilization devices to the PET unit, and assurance that these immobilization devices are properly applied all aid in PET image acquisition for radiation oncology. Proper patient alignment is aided by the use of external lasers (identical to those in the simulator and radiation treatment rooms) and by having a radiation therapist accompany the patient to the PET facility to help with immobilization and positioning.
Coregistration of PET and CT images obtained with an integrated PET/CT scanner leads to improved image interpretation. Lardinois et al. (26) recently reported a prospective study of 50 patients with suspected or proven NSCLC and compared the accuracy of interpretations of CT alone, PET alone, visually correlated PET and CT, and the combined PET/CT data. Histopathologic staging was the reference standard for both nodal and distant metastases. The integrated PET/CT interpretations provided additional information in comparison with interpretations based on visual correlation of PET and CT in 20 of 49 patients. The diagnostic accuracy was improved with the integrated study for both tumor (P = 0.001) and nodal (P = 0.013) staging. Thus, it is reasonable to expect that the information provided by integrated PET/CT will increase the accuracy of RTP in a similar manner. Although as yet no reports of radiation treatment planning using the integrated PET/CT unit have appeared in the literature, we and others have begun to use such devices for the treatment planning process in patients with NSCLC. The initial experience suggests that we have significantly improved image coregistration. However, inherent differences between PET and CT data acquisition, especially with regard to respiratory motion, have not been successfully addressed with current PET/CT scanners. Fixing these deficiencies is an important goal of current research in this area.
PET Image Accessibility
Accessibility of the images remains one of the main difficulties for radiation oncology applications. For images to be transferred and accepted, a common electronic language is required. Most new PET/CT scanners export images in Digital Imaging and Communications in Medicine (DICOM) standard format. However, many older PET scanners do not. Likewise, some RTP software systems do not accept DICOM images. This problem is likely to be solved with future software releases, but consumers should be aware of these software requirements when considering their own needs with regard to PET-based RTP.
Tumor Motion
Tumor motion secondary to ventilation is problematic for RTP of lung cancer, especially for lesions residing in the lower lobes. Four-dimensional (4D) imaging has demonstrated that these lesions may move up to 3 cm in a single dimension and that such lesions typically move in trajectories involving each of the x, y, and z coordinates (27–29). For RTP, 3 principal methods are used to account for tumor excursion. The first is to fuse CT images obtained at end-tidal inspiration and end-tidal expiration to obtain a composite tumor volume within the limits of tidal breathing (4D method) (29). The second method is to gate the linear accelerator to “beam on” during specific phases of the ventilatory cycle when the tumor is within the radiation therapy portal (gating method). The third method is to gate the patient by breath hold maneuvers by an active breath control device (ABC) or with deep inspiration breath hold (DIBH) (30–33). Each of these methods has its advantages and disadvantages with respect to radiation treatment delivery. The 4D method is simple to implement but enlarges the radiation treatment volume, which leads to increased normal tissue doses. The gating method is available via hard- and software from vendors and is currently being implemented in some clinics with either stereotactic radiotherapy or intensity modulated radiation therapy expertise. The ABC and DIBH techniques may be of limited use in the lung cancer population with compromised lung function.
The incorporation of PET into RTP will affect each method of radiation therapy. The addition of PET simplifies the 4D volume method. Whereas spiral CT scanning takes seconds (and is performed with breath holding), PET imaging takes several minutes. Thus, the PET tumor volume itself provides the composite 4D volume that accounts for tumor excursion. Implementation of the gating method using PET/CT–based RTP would require gated PET images. Thus, in addition to the technologic requirements for gating the linear accelerator, an institution would need a mechanism to gate the PET acquisition. This method has an advantage in yielding smaller radiation therapy volumes and lower radiation dose to normal tissues, but its implementation will require intensive research and development. Investigators at Memorial-Sloan Kettering Cancer Center have developed a camera-based respiratory gating system to link each phase of the respiratory trace with PET images acquired during that phase of the respiratory cycle (34).
Will Biologic Target Volumes Affect Patient Outcome?
Finally, we need to demonstrate whether the use of PET in RTP will improve patient outcome beyond the information gained with diagnostic PET. Mac Manus et al. (24) have reported on a prospective study demonstrating that diagnostic PET studies obtained for staging are predictive of outcome. In the study, 153 patients with unresectable NSCLC who were candidates for radical radiation therapy underwent PET imaging after conventional staging. Distant metastases were detected by PET in 28 patients (18%) in the lung, extrathoracic lymph nodes, bone, adrenal, liver and other abdominal sites, and skin. In several patients, multiple metastatic sites were detected. Extensive regional nodal disease was detected in 18 (12%). After PET, 107 patients (70%) were judged to be potentially eligible for curative treatment: radiation therapy with concurrent platinum chemotherapy in 68, radiation therapy alone in 34, and definitive surgery in 5 patients. The 5 surgical patients had been considered inoperable before PET was performed. In the remaining 46 patients (30%), palliative therapy was given after PET. Patients treated with definitive treatment had a significantly better 2-y survival (44%) than those treated for palliation (0%). With both CT and PET staging, about 75% of patients with stage I NSCLC survived 2 y in contrast to 45% of those with stage II and III disease. There were no 2-y survivors with stage IV disease. Additional prospective trials are needed to demonstrate the impact of PET-based RTP on patient outcomes. The Radiation Therapy Oncology Group is developing a limited-institution pilot study for patients with stages I–III NSCLC for whom radiation therapy is planned using information from integrated PET/CT scanners. This small study has been difficult to initiate because of PET image transfer issues described previously. The answer to the question of whether improvements in outcome can be achieved awaits future studies.
Potential Applications for Other Radiopharmaceuticals
Imaging with 18F-FDG represents only a first step in the application of PET in oncology. Other radiopharmaceuticals that interrogate molecular targets other than glucose transporter proteins and hexokinase can provide important information about tumor biology that also should be exploitable for RTP. One such example is Cu(II)-diacetyl-bis-N-(4)-methylthiosemicarbazone (Cu-ATSM), which can be labeled with several positron-emitting radionuclides of copper. PET with Cu-ATSM reliably identifies regions of hypoxia within tumor. We have previously shown that tumor-to-muscle ratios on Cu-ATSM PET in patients with NSCLC are predictive of response to radiation therapy (35). These more radioresistant volumes of tumor can potentially be selectively targeted with higher doses of radiation. The development of intensity-modulated radiation therapy, a tool to deliver radiation doses more conformally, can potentially be used to target these hypoxic regions and thus to deliver heterogeneously designed radiation doses (36). Another example is 3′-deoxy-3′-[18F]fluorothymidine (FLT), which assesses tumor cell proliferation (37,38). FLT is taken up by cells and phosphorylated by thymidine kinase 1. FLT-monophosphate is trapped within the cell, and its concentration provides a measure of cellular thymidine kinase activity, which reflects the rate of cell proliferation. Knowledge of patient-specific tumor proliferation rates may conceptually aid in selecting patients for altered fractionation schedules. The development of innovative radiopharmaceuticals will continue to provide opportunities for the exploitation of biologic targets.
Footnotes
Received Sep. 17, 2003; revision accepted Nov. 3, 2003.
For correspondence or reprints contact: Jeffrey D. Bradley, MD, Department of Radiation Oncology, Washington University School of Medicine, 4921 Parkview Place, St. Louis, MO 63110.
E-mail: bradley{at}radonc.wustl.edu
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Positron emission tomography imaging approaches for external beam radiation therapies: current status and future developments
- 18F-FDG PET/CT for Image-Guided and Intensity-Modulated Radiotherapy
- Postacquisition Detection of Tumor Motion in the Lung and Upper Abdomen Using List-Mode PET Data: A Feasibility Study
- Introduction
- Commonly Used Imaging Techniques for Diagnosis and Staging